

International Journal of Surgery Research and Practice
Tumor Grading, Architectural Growth Pattern and Angiogenesis Proprieties Correlation in Surgical Patients Treated for HCC
Wlodzimierz Otto1*, Maria Kr�l2, Urszula Wilkowojska2, Ewa Wilczek3, Boguslaw Najnigier1, Janusz Sierdzinski4* and Marek Krawczyk1
1Department of General, Transplant & Liver Surgery, Central Teaching Hospital, Medical University of Warsaw, Poland
2Department of Oncology, Hematology & Internal Medicine, Medical University of Warsaw, Poland
3Department of Pathology, Medical University of Warsaw, Poland
4Department of Medical Informatics & Telemedicine, Central Teaching Hospital, Medical University of Warsaw, Poland
*Corresponding authors: Wlodzimierz Otto, Professor of Surgery, MD, PhD, Department of General, Transplant & Liver Surgery, Central Teaching Hospital, Medical University of Warsaw, Banacha 1a, Warsaw 02-097, Poland, Tel: +48 22 599 2546, E-mail: wotto@wum.edu.pl
Janusz Sierdzinski, PhD, Department of Medical Informatics & Telemedicine, Central Teaching Hospital, Medical University of Warsaw, Banacha 1a, Warsaw 02-097, Poland, Tel: +48 22 658 2997, E-mail: jsierdzinski@wum.edu.pl
Int J Surg Res Pract, IJSRP-1-014, (Volume 1, Issue 1), Original Article; ISSN: 2378-3397
Received: August 28, 2014 | Accepted: November 23, 2014 | Published: November 28, 2014
Citation: Otto W, Krol M, Wilkowojska U, Wilczek E, Najnigier B, et al. (2014) Tumor Grading, Architectural Growth Pattern and Angiogenesis Proprieties Correlation in Surgical Patients Treated for HCC. Int J Surg Res Pract 1:014. 10.23937/2378-3397/1410014
Copyright: © 2014 Otto W, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Tumor grading and architectural growth patterns impact the results, but the unfavorable tumor biology is revealed no sooner than on explant examination. Thus, they are not concerned in preoperative calculations.
Aim of study: To evaluate the correlation between circulating EPCS, soluble angiogenesis factors and architectural growth patterns of HCC in surgical patients.
Methods: The study reported on 159 patients treated for HCC in 2009/2013; 58 were suitable for surgery, 55 for liver transplantation and 46 for palliation. The rate of circulating EPCs was assessed by the flow cytometer; the serum VEGF concentration was measured by ELISA. The tissue samples were examined for tumor grading and architectural growth patterns of HCC, and for the expression of VGEF/VEGFR-2 by immunohistochemical staining. The data were analyzed statistically.
Results: There were 58 trabecular, 43 tubular, and 58 solid tumors of HCC. There were significant differences in the rate of circulating HSCs and EPCs in the blood of their possessors (Chisq=5.8, p< 0.05 and Chisq=7.14, p< 0.02, respectively). The rate of circulating EPCs correlated with the concentration of VEGFR-2 within the tumor tissue according to the grade of HCC differentiation (r=0.5 p< 0.02, r=-0.24, p< 0.01, r=-0.5, p< 0.004, for Grade I, II, and III, respectively).
Conclusion: Angiogenesis capability of the tumor corresponds to its histologic features. The results indicate a benefit from the evaluation of angiogenesis factors in the course of patients� selection to the treatment options.
Introduction
Hepatocellular carcinoma is a systemic process, developing in the majority of patients upon post-inflammatory or alcohol-induced liver cirrhosis. The only potentially curative options are surgical resection and liver transplantation. The relevant clinical scoring systems provide criteria for the eligibility of patients as concerns liver sufficiency and tumor development. Many reports indicate that up to 40% of patients have tumor recurrence and stress that a significant percentage of them is revealed within the first year of follow-up, however [1-6]. Certainly, such clinical experience indicates the need for criteria that would be based to a larger extent on tumor biology [7,8].
Some new hopes for a more effective system of clinical evaluation concern the mechanism of angiogenesis that is fundamental for the HCC growth. The tumor stimulates the process of angiogenesis by shifting the balance between stimulators and inhibitors of angiogenesis towards pro-angiogenesis factors [9-11]. Tumor-derived cytokines, especially the vascular endothelial growth factor (VEGF), foster the population of stem and progenitor cells in peripheral blood circulation. The increase of circulating progenitor cells and the serum VEGF concentration were found in several studies to be associated with a more aggressive propriety of HCC. It is assumed that the evaluation of the preoperative level of angiogenesis factors may indicate unfavorable tumor biology prior to the decision concerning the treatment option. The patient selection for the procedure could thus be more judicious and predictive [12-15].
The purpose of the study was to assess the correlation between the level of soluble angiogenesis factors in the peripheral blood circulation, the expression of angiogenesis factors in on-explant HCC tumor tissue and the histologic characteristics of HCC, including tumor vascular invasion, grading and architectural growth pattern, in surgical patients.
Material
General considerations
The study was carried out prospectively on 159 patients with hepatocellular carcinoma treated from 2009 to 2013 at the Department of General, Transplant and Liver Surgery, in cooperation with The Laboratory of Cytometer, Department of Oncology, Hematology and Internal Medicine, and the Department of Pathology, The Central Teaching Hospital, Medical University of Warsaw, Banacha 1a, Warsaw, Poland. The study constitutes part of research projects granted by the National Science Centre (Grant No. NN 403 177940 [E 154] of the National Science Centre, Poland). The study protocol was approved by the Bioethics Committee of Medical University of Warsaw, and an informed consent was obtained from all patients undergoing the procedure
Including criteria - group of patientsThe study covered patients with HCC selected to the appropriate treatment procedure according to the TNM classification, the BCLC (Barcelona Clinic Liver Cancer) score system, the Child-Pugh classification and the Milan criteria. None of them had been pretreated for HCC.
Group A � Liver resection: Fifty eight patients (36 males, 22 females, median age 56 years)presented with a single tumor at the I-II clinical stage (T1/T2,N0,M0), A1-A4 BCLC classification, with proper liver function (healthy liver or cirrhotic liver in the Child-Pugh class A), and were selected for liver resection. In 29 HCC developed in a healthy liver, in 29 due to liver cirrhosis caused by viral hepatitis (HBV/HCV), with the component of alcoholic liver disease (ALD) present in 9 of them. No evidence of gross vascular invasion and no regional nodes or distant metastases were present. The median serum alpha-fetoprotein (AFP) for all 58 patients was 13.50ng/ml, SD+/-14557. There were no significant post-operative complications related to the procedure in the reported group.
Group B � Liver transplantation: Fifty five patients (38 males, 17 females, median age 51 years) presented with liver cirrhosis caused by viral hepatitis (HBV/HCV), with the component of alcoholic disease (ALD) confirmed in 10 of them. They were diagnosed with a single tumor of < 5cm or 3 tumors with a total diameter of < 3cm (all fulfilling the Milan criteria), at the clinical stage I-IITNM, A1-A4BCLC, and with liver cirrhosis of Class A-B according to the Child-Pugh classification. They were qualified for liver transplantation, and successfully transplanted in 2009/2010. No evidence of gross vascular invasion and no regional nodes or distant metastases were present. The median serum alpha-fetoprotein (AFP) for all 55 patients was 43.35ng/mL, SD+/-3444.47. There were no significant post-operative complications related to the procedure of liver transplantation in the reported group.
Group C � Palliative non-surgical treatment: Forty six patients (26 males, 20 females, median age 63 years) presented with advanced HCC. The stage of cancer development disqualified them from the operation, and they were indicated for palliative treatment. In 38 patients liver cirrhosis developed due to viral hepatitis (HBV/HCV), with the component of alcoholic disease confirmed in 10 of them. In 8 patients the tumor developed in a healthy liver. In 35% of them evidence of gross vascular invasion was present, in 15% the regional lymphnodes were invaded, in 12% distant metastases were present, as well. None of them had been pretreated for HCC but 62% presented with a history of treatment for liver dysfunction and portal hypertension; 9 patients were clinically evaluated as belonging to Class A, 25 to Class B, and 12 to Class C, according to the Child-Pugh classification. The median serum alpha-fetoprotein (AFP) for all 46 patients was 59.05ng/ml, SD+/-17048. All patients underwent USG guided biopsy of the tumor prior to the treatment.
Excluding criteria
The excluding criteria were age>80, diagnosed coexistence of coronary heart disease, past history of myocardial infarction, extensive burns, ischemic legs against vascular inflammation and atherosclerosis, extra hepatic pathology precluding surgery, past history of angiogenesis-inhibiting chemotherapy, statins� therapy or gene therapy.
Methods
Clinical considerations
The clinical diagnosis and assessment of liver function and cancer staging in patients with hepatocellular carcinoma were based on the clinical view, laboratory tests - blood morphology, levels of albumin, bilirubin, transaminases� activities (ASTAT, ALAT), alkaline phosphatase (AFP), coagulation factors (INR, platelet count-PLT), the level of alpha-fetoprotein (AFP) in the serum and the screening tests - ultrasound (ultrasound and Doppler ultrasound), computed tomography (CT) and magnetic resonance imaging (MRI).
Flow cytometer measurements
The identification of the desired cell fraction was achieved by the standard enumeration of human endothelial progenitor cells by surface markers expression according to the procedure approved by MiltenyiBiotec, Germany. Samples of 2 ml of fresh peripheral venous blood were collected from each patient into a tube containing K3EDTA, and processed within 1 hour. Seven test tubes containing 100�L of fresh blood each + 40�L EPC Staining Cocktail composed of surface antibodies (10�L CD34 FITC BD Biosciences, 10�L CD133 PE MiltenyiBiotec, 10�L CD45 Per CP BD Biosciences and 10�L CD309 APC MiltenyiBiotec) constituted the measured sample; 3 test tubes containing 100�L of fresh blood each + 40�L EPC Cocktail (10�L CD34 FITC BD Biosciences, 10�L CD133 PE MiltenyiBiotec, 10 �L CD45 Per CP BD Biosciences but 10�L Isotype ControlMiltenyiBiotec) constituted the control. After 20 minutes of incubation, red cells were lysed with FACS Lysing Solution (BD Biosciences), incubated again for 10 minutes, rinsed in CellWash (BD Sciences) and pooled.
Then the samples were consecutively analyzed with the flow cytometer FACS CANTO II (BD Biosciences). The data were analyzed by using the multiparametric cells gating strategy approved by the International Society of Hematology and Graft Engineering (ISHAGE). The circulating hematopoietic stem cells were defined by the phenotype of CD34+, CD133+, CD45dim and quantified as percentage within the white blood cells population (%HSCs/WBC). The endothelial progenitor stem cells were defined by the phenotype of CD34+, CD133+, CD45dim, CD309+, and quantified as percentage within the hematopoietic stem cells subpopulation (% EPCs/HSCs).
Serologic evaluation
Serum samples for the evaluation of the vascular endothelial growth factor (VEGF) were collected from the patients simultaneously with the blood collection. They were drawn into a serum separator and centrifuged at 3,000rpm for 10 minutes, then stored at -80�C. The VEGF levels were measured with an enzyme-linked immunosorbent assay kit designed to measure human serum VEGF concentration (Quantikine Human VEGF Immunoassay; R&D Systems, Minneapolis, MN, USA); 100�L recombinant human VEGF standard and serum sample were serially diluted and pipetted onto a microtiter plate coated with murine monoclonal antibody specific for human VEGF and incubated for 2 hours at room temperature. After washing, a horseradish peroxidase-linked polyclonal antibody specific for VGEF was added, and after further washing tetramethylbenzidine was added. The sensitivity of the assay was 9pg/mL, and the coefficients of variation of intra-assay and inter-assay determination were in the range of 4.4-6.7% and 6.2-8.8%, as indicated by the producer. The VEGF concentration in each sample was measured in duplicate by an investigator blinded to the clinical information.
Pathologic study
On explant analysis: The explanted tissues (livers or parts of tumor-containing tissue) from the 113 resected and transplanted patients as well as thick needle tissue samples biopsied from the 46 patients undergoing palliative treatment were examined by an expert pathologist with experience in liver cirrhosis and HCC pathology. The pathologist was unaware of the pre-operative rates of circulating HSCs and EPCs enumeration, and levels of serum VEGF concentrations. Surgical specimens were fixed in 10% formalin and embedded in paraffin. 4�m-thick sections were cut from blocks and stained with hematoxylin and eosin to study the features of HCC, and the tumor surrounding liver tissue. Advances in liver cirrhosis were evaluated, and the absence of microsatellite lesions corresponding to intrahepatic metastases was confirmed. Serial sections on the explanted livers were performed to confirm the tumor stage within the Milan criteria. Then each tumor was also graded as moderately and poorly differentiated according to the WHO system of classification (modified Edmondson-Steiner system), tumor architectural growth pattern, and presence of microvascular invasion.
Immunohistochemical evaluation: Representative regions of blocks were identified and prepared for immunohistochemical staining; sections were deparaffinized in xylene, rehydrated through graded series of ethanol, and treated with 3% hydrogen peroxidase to block endogenous peroxidase. Then, they were incubated with the 10% goat serum to reduce non-specific binding and with primary antibodies over night at 4�C. Immunohistochemical detection of VEGF and VEGFR-2 (CD309+) was performed with rabbit polyclonal antibodies (Millipore), and anti-rabbit ImmPress System (Vector Laboratories). The surrounding liver tissue on the side of the tumor served as an internal positive control. The negative control was obtained by replacing the polyclonal antibody with non-immunized rabbit serum. The sections were examined by two independent pathologists without the knowledge of the clinic-pathological data. For each section, five random areas were selected in x400 fields, and the number of cells with positively stained cytoplasm was counted. The rate of positive cells was calculated by averaging the five counts, and graded as: low < 25%, moderate 25 � 50 %, and high > 50%.
Statistical analysis
A descriptive analysis was computed for all variables. The data for clinical settings prior to the treatment were collected in each group. Pathologic investigations concerning the type of cirrhosis, number of lesions, tumor grading, tumor architectural growth pattern, and tumor microvascular invasion were carried out on the explants obtained from patients who underwent surgery and on tissue specimens biopsied from patients who received non-surgical palliative treatment. The quantitative data of pre-transplant rates of HSCs and EPCs enumeration, the serum VEGF, and the rates of VEGF/VEGFR-2 expression within the tumor tissue were expressed as median, and mean +/- SD. A univariate analysis was performed to assess the relationships between the angiogenesis factors and the rates of circulating hematopoietic stem cells (%HSCs/WBC), the rates of endothelial progenitor cells (%EPCs/HSCs),the serum VEGF concentration, the expression of VEGF and VEGFR-2 in the tumor tissue, by using Chi-square tests, Kruskal-Wallis analysis, and Test U Mann-Whitney. The correlation between the variables was estimated with the Spearman correlation coefficient. Results with a p-value of less than 0.05 were considered as statistically significant.
Results
Clinical settlements
The patients from the groups qualified to particular treatment options (liver resection - Group A, liver transplantation- Group B, palliative treatment- Group C), differed in terms of the history of the disease, the clinical status, and the picture at the time of presentation. Mean values of platelet count (PLT) were 160 x109/L (SD +/-74000) in Group A, 75 x 109/L (SD +/-46000) in Group B, and 123 x 109/L (SD +/-82000) in Group C (Chisq=50.32, p< 0.001); mean values of INR were 1.06 (SD +/-0.14) in Group A, 1.21 (SD +/-0.17) in Group B, and 1.13 (SD +/-0.13) in Group C (Chisq=31.13, p< 0.001); mean values of alpha-fetoprotein (AFP) level were 15.5ng/mL (SD +/-14557) in Group A, 43.35ng/mL (SD =/-3444) in Group B, and 59.05ng/mL (SD +/-17048) in Group C (Chisq=6.2, p< 0.04).
Pathologic findings and tumor angiogenesis potential
Pathologic evaluation confirmed that all patients had a hepatocellular carcinoma. There were not microsatellites nodules corresponding to intrahepatic metastases found in any of the patients who underwent hepatectomy, or additional tumors that were unrecognized prior to the operation in those who underwent partial liver resection. Pathologic examination showed that the patients selected to particular treatment options by the standard systems of clinical classification differed significantly by the tumor growth pattern and by the presence of the tumor microvascular invasion. The differences in the grade of tumor differentiation appeared to be not significant, however. The data related to pathologic findings are presented in Table 1. Certainly, the patients presented with a different angiogenesis potential of the tumor as exhibited by the significant differences of the level and the expression of all angiogenesis factors evaluated in the study. The values and the results of statistical analysis are presented in Table 2.
![]()
Table 1: Results of pathologic investigation indicating the number of tumors in relation to the grade of development, growth patterns and vessel invasion in 159 HCC patients.
View Table 1
![]()
Table 2: The different angiogenesis potential of the patient treated with liver resection, liver transplantation and palliatively for HCC .
View Table 2
Tumor angiogenesis propriety and tumor growth pattern
The mean rates of the circulating hematopoietic stem cells within the WBC (%HSCs/WBC) gradually increased from 0.012 % (SD +/-0.009) in the trabecular,0.0143 % (SD +/-0.0079) in the acinar, to 0.0181 % (SD +/-0.008) in the solid tumors (Chisq=5.8, p< 0.05) whereas the rates of the circulating endothelial progenitor cells within the hematopoietic stem cells population (%EPCs/HSCs) gradually decreased from 3.43 (SD +/-2.1) in the trabecular, 3.14% (SD +/-6.1 in the acinar, to 2.91% (SD +/-4.5) in the solid tumors (Chisq=7.14, p< 0.02) (Figure 1). The changes found in the rates of the circulating hematopoietic and endothelial progenitor cells were accompanied by significant changes in the mean levels of serum VEGF concentration that ranged from 231.25pg/mL (SD +/-230) in the trabecular, 358.83 pg/mL (SD +/-107) in the acinar, to 240.20 pg/mL (SD +/-168) in the solid tumors (Chisq=6.3, p< 0.05), and in the mean levels of VEGFR-2expression within the tumor tissue, that were established at 47.2 % (SD +/-12.1) in the trabecular, 44.0 % (SD +/-6.1) in the acinar, and 49.1 % (SD +/-14.5) in the solid tumors (Chisq=7.24, p< 0.02) (Figure 2).
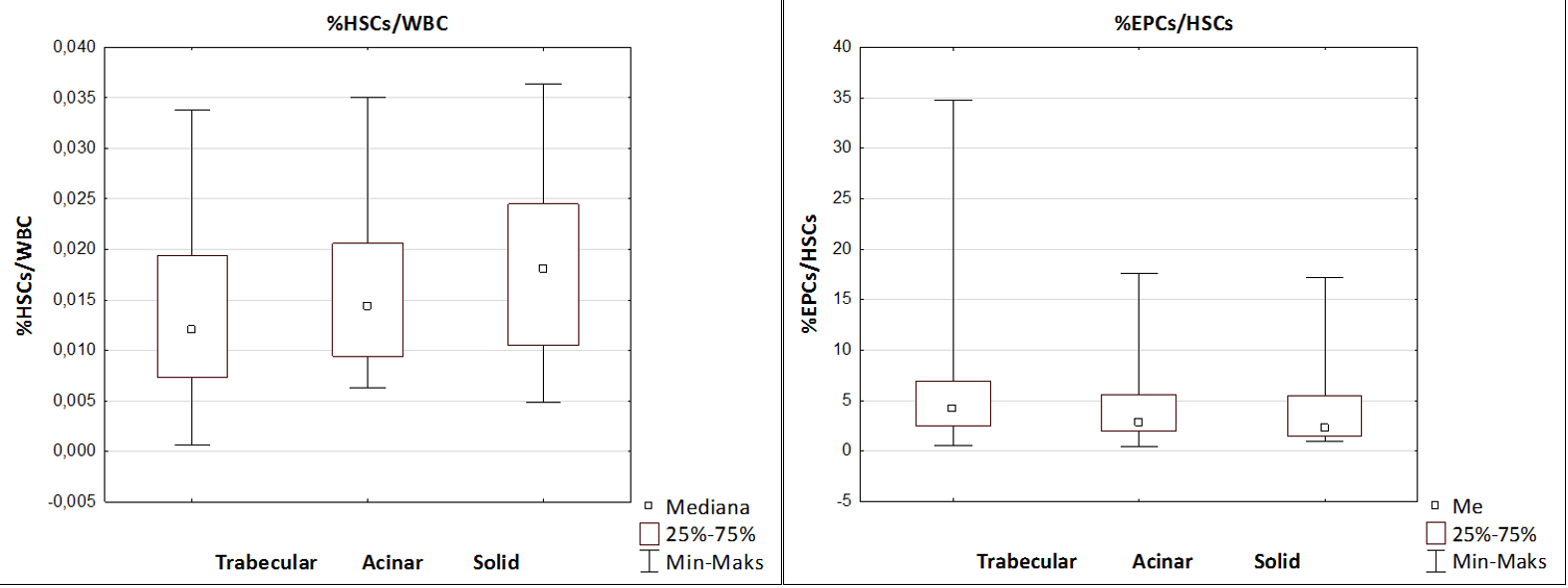 Figure 1: The rates of circulating hematopoietic stem cells within the WBC (%HSCs/WBC) and endothelial progenitor cells within the HSCs (%EPCs/HSCs)
in trabecular, acinar and solid tumor growth patterns in 159 surgical patients treated for HCC.
View Figure 1
Figure 1: The rates of circulating hematopoietic stem cells within the WBC (%HSCs/WBC) and endothelial progenitor cells within the HSCs (%EPCs/HSCs)
in trabecular, acinar and solid tumor growth patterns in 159 surgical patients treated for HCC.
View Figure 1
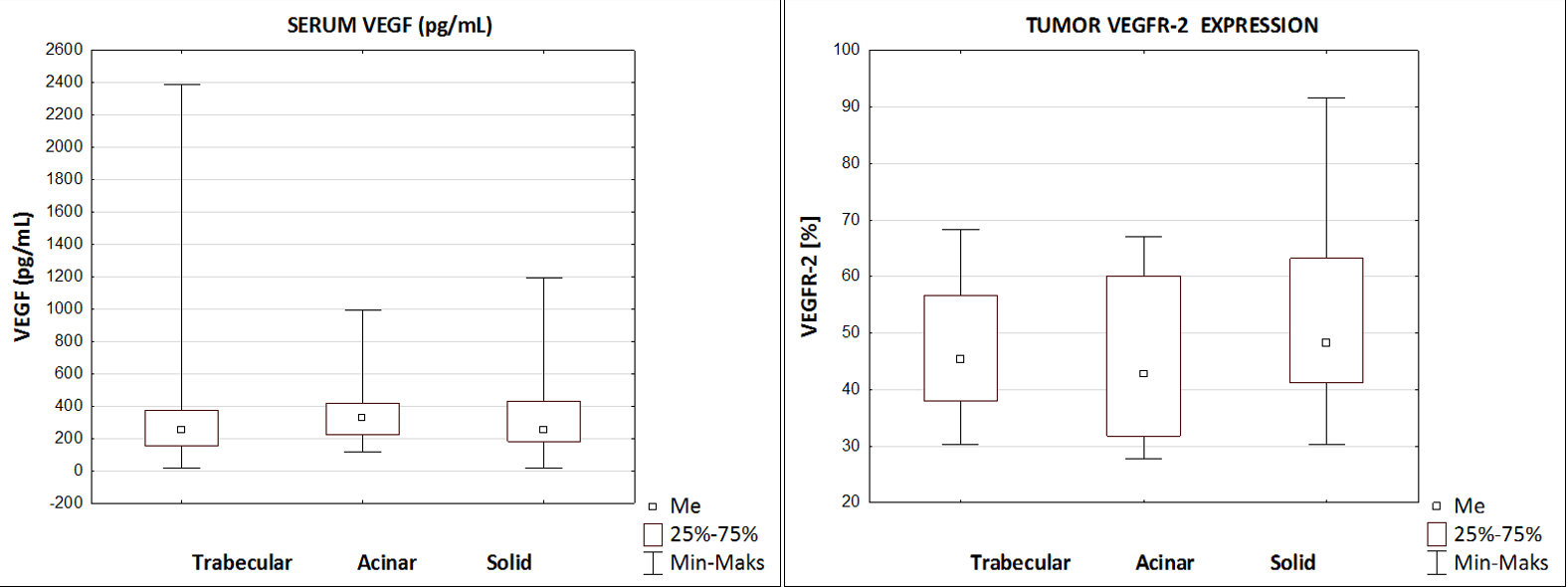 Figure 2: The levels of serum VEGF concentration and tumor tissue VEGFR-2 expression in trabecular, acinar and solid tumor growth patterns in 159 surgical
patients treated for HCC.
View Figure 2
Figure 2: The levels of serum VEGF concentration and tumor tissue VEGFR-2 expression in trabecular, acinar and solid tumor growth patterns in 159 surgical
patients treated for HCC.
View Figure 2
Tumor angiogenesis propriety and tumor grade of differentiation
The mean rates of the circulating hematopoietic stem cells within WBC (%HSCs/WBC) gradually increased from 0.0091 % (SD +/-0.007) in Grade I, 0.0151 % (SD +/-0.007) in Grade II, to 0.0165 % (SD +/-0.008) in Grade III tumors ( Chisq=5.82, p< 0.05) whereas the mean rates of the circulating endothelial progenitor cells within the hematopoietic stem cells (%EPCs/HSCs) gradually decreased from 6.71 % (SD +/- 4.36) in Grade I, by 2,61 % (SD +/- 4.81) in Grade II, and 2.60 % (SD +/-4.55) in Grade III tumors (Chisq=8.24, p< 0.02), respectively (Figure 3). The changes in the rates of the studied cells populations were accompanied by significant changes in the mean levels of serum VEGF concentration, that was 215.36pg/mL (SD +/-136) in Grade I, 306.23 pg/mL (SD +/-277) in Grade II, and 277.77pg/mL (SD +/-258) in Grade III tumors (Chisq=7.20, p< 0.02), and in the levels of VEGFR-2 expression within the tumor tissue, that was 44.3% (SD +/-10.5) in Grade I, 45.6% (SD +/-10.5) in Grade II, 45.5% (SD +/-12.3) in Grade III (Chisq=8.26, p< 0.001), respectively (Figure 4).
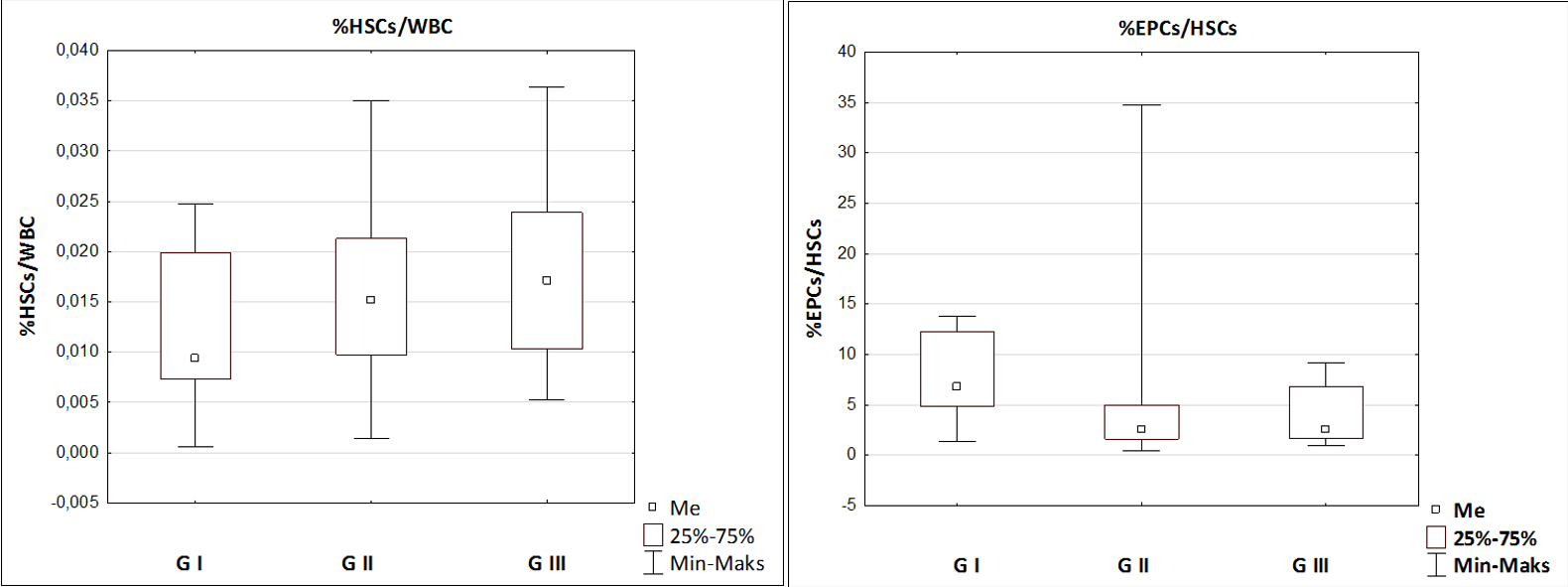 Figure 3: The rates of circulating hematopoietic stem cells within the WBC (%HSCs/WBC) and endothelial progenitor cells within the HSCs (%EPCs/HSCs) in Grade I � Grade III tumors in 159 surgical patients treated for HCC.
View Figure 3
Figure 3: The rates of circulating hematopoietic stem cells within the WBC (%HSCs/WBC) and endothelial progenitor cells within the HSCs (%EPCs/HSCs) in Grade I � Grade III tumors in 159 surgical patients treated for HCC.
View Figure 3
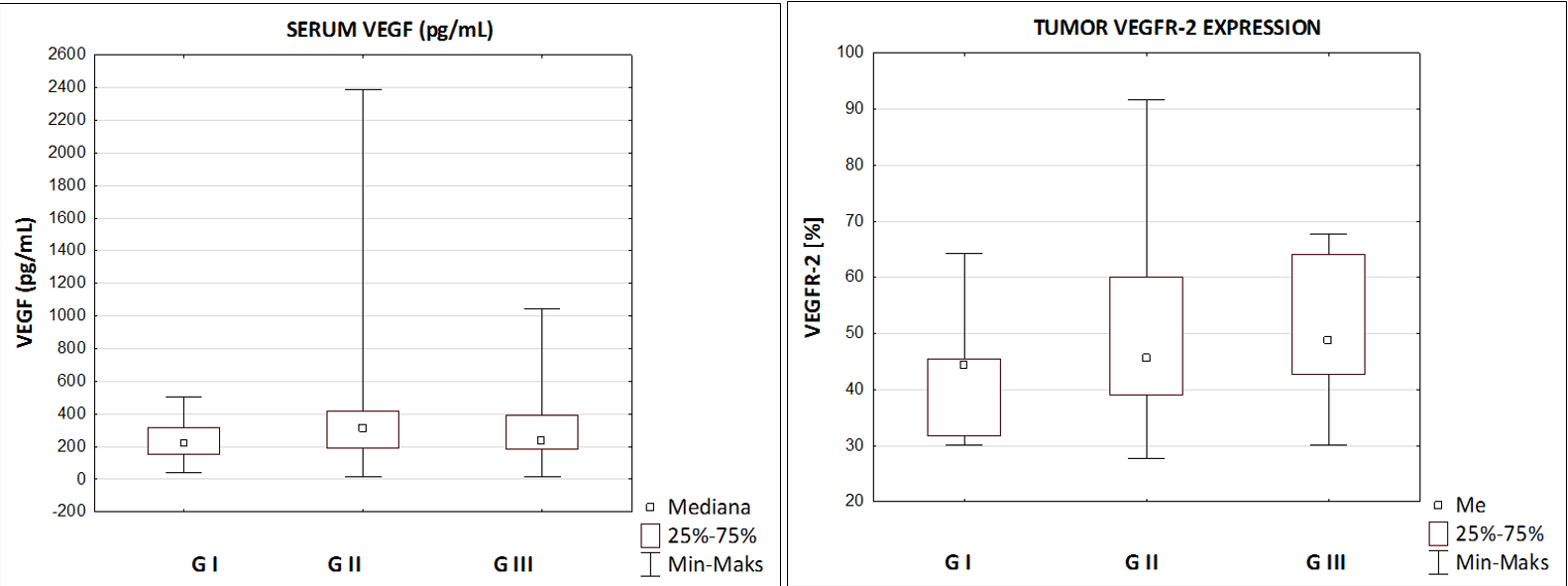 Figure 4: The levels of serum VEGF concentration and tumor tissue VEGFR-2 expression in Grade I - Grade III tumors in 159 surgical patients treated for HCC.
View Figure 4
Figure 4: The levels of serum VEGF concentration and tumor tissue VEGFR-2 expression in Grade I - Grade III tumors in 159 surgical patients treated for HCC.
View Figure 4
Tumor angiogenesis potential and tumor histology correlations
The study showed some interesting correlations between the variables and indicates the increment of angiogenesis potential according to the tumor grading, its architectural growth pattern, and the presence of the microvascular invasion to the surrounding liver tissue. The rates of the circulating hematopoietic stem cells within WBC (%HSCs/WBC) were found to correlate with the tumor tissue expression of VEGFR-2 within Grade II tumors (r=0.26, p< 0.005),within Grade III tumors (r=0.44, p< 0.01), and within the solid tumors (r=0.41, p< 0.001), (Figure 5).
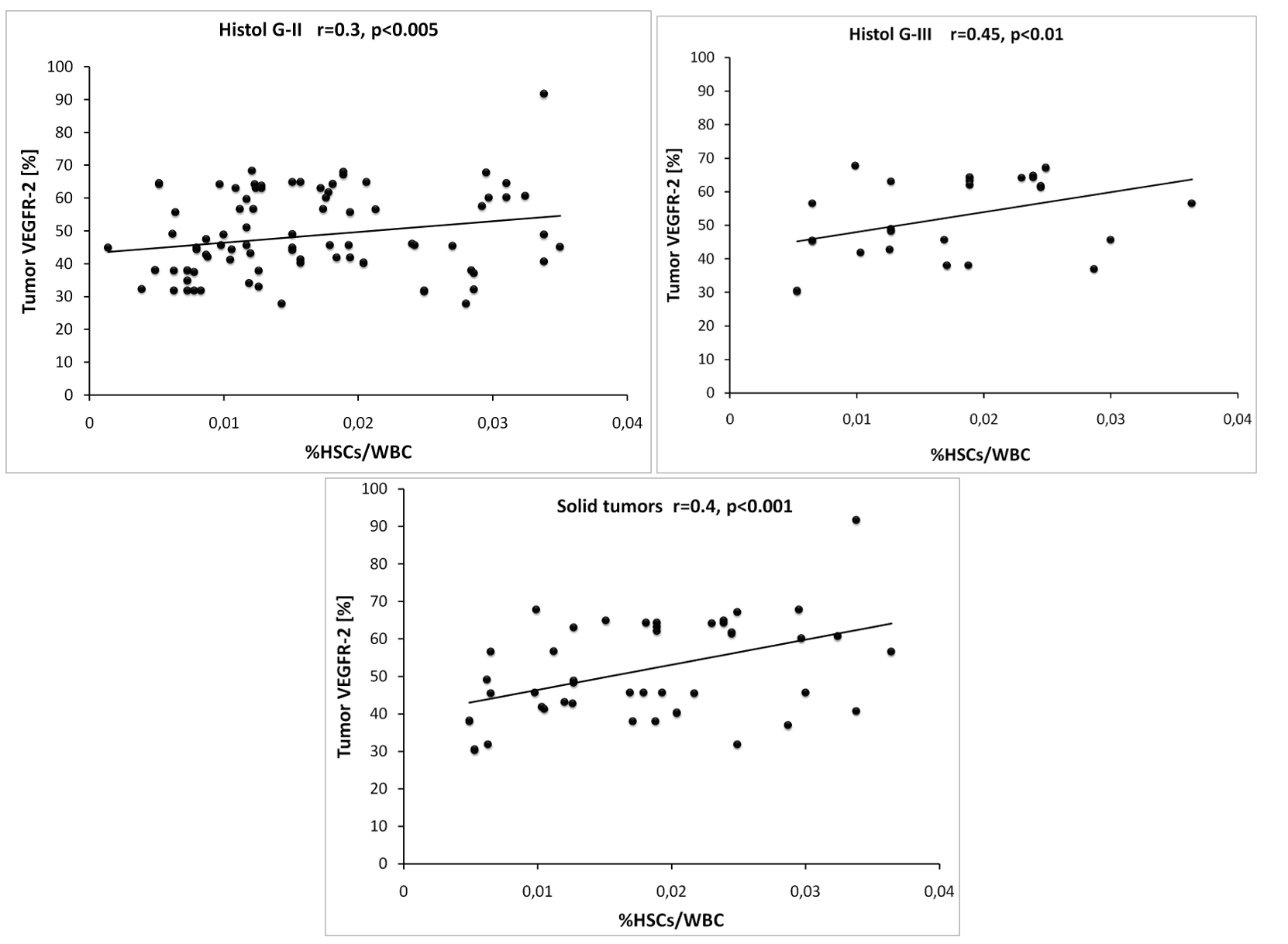 Figure 5:The correlations between the rates of hematiopoietic stem cells within WBC (%HSCs/WBC) and tumor tissue VEGFR-2 expression in surgical patients treated for HCC.
View Figure 5
Figure 5:The correlations between the rates of hematiopoietic stem cells within WBC (%HSCs/WBC) and tumor tissue VEGFR-2 expression in surgical patients treated for HCC.
View Figure 5
On the other hand, the rates of the circulating endothelial progenitor cells within the hematopoietic stem cells population (%EPCs/HSCs) were found to correlate with the level of serum VEGF concentration within the Grade III tumors (r= - 0.5, p< 0.004) (Figure 6). The rates of the circulating hematopoietic stem cells (%HSCs/WBC) and endothelial progenitor cells (%EPCs/HSCs) were found to correlate with the tumor tissue VEGFR-2 expression within the tumors revealing the microvascular invasion to the surrounding liver: r=0.44, p< 0.001 for HSCs/WBC, and r=- 0.3, p< 0.02 for EPCs/HSCs, respectively (Figure 7).
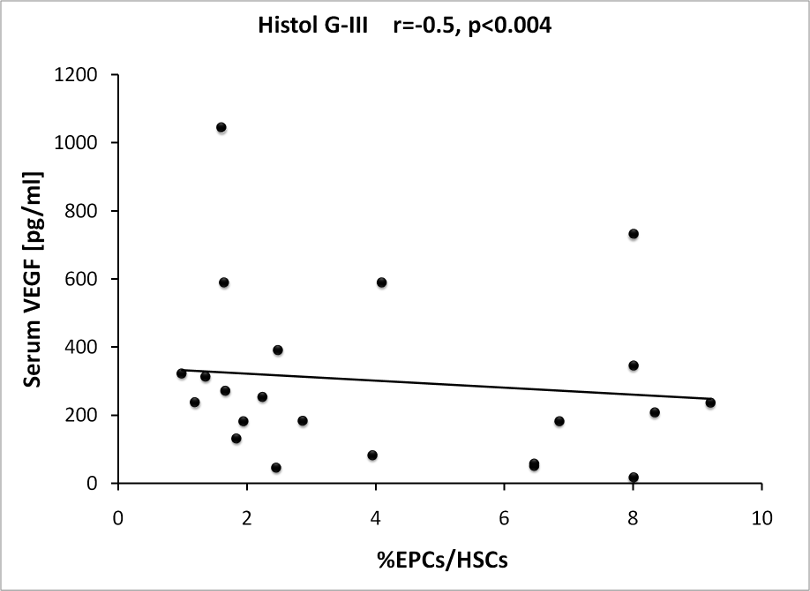 Figure 6:The correlations between the rates of endothelial progenitor cells within hematopoietic stem cells (%EPCs/HSCs) and tumor tissue VEGFR-2 expression and the serum VEGF concentration in surgical patients treated for HCC.
View Figure 6
Figure 6:The correlations between the rates of endothelial progenitor cells within hematopoietic stem cells (%EPCs/HSCs) and tumor tissue VEGFR-2 expression and the serum VEGF concentration in surgical patients treated for HCC.
View Figure 6
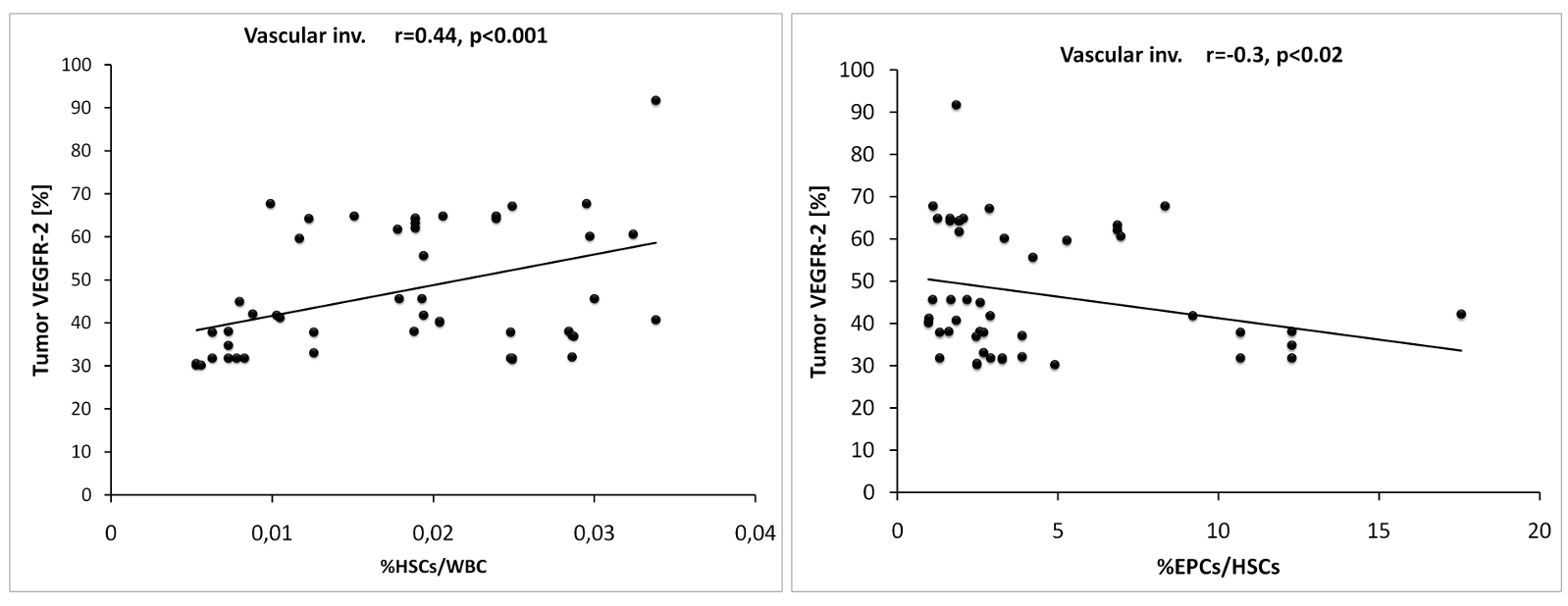 Figure 7:The correlations between the rates of hematopoietic stem cells within WBC (%HSCs/WBC) and endothelial progenitor cells within HSCs (%EPCs/HSCs) and tumor tissue VEGFR-2 expression in tumors exhibiting presence of microvascular invasion to surrounding liver tissue in suegical patients treated for HCC.
View Figure 7
Figure 7:The correlations between the rates of hematopoietic stem cells within WBC (%HSCs/WBC) and endothelial progenitor cells within HSCs (%EPCs/HSCs) and tumor tissue VEGFR-2 expression in tumors exhibiting presence of microvascular invasion to surrounding liver tissue in suegical patients treated for HCC.
View Figure 7
Discussion
There are approximately 150-175 patients undergoing treatment for hepatocellular carcinoma at the Department of General, Transplant & Liver Surgery, Medical University of Warsaw every year. More than seven hundred fifty of these patients were considered and evaluated for treatment in the years 2009-2013. Almost 80% of them presented with liver cirrhosis, and approximately 75% of them were found suitable only for palliative non-surgical treatment, unfortunately. Radical treatment by liver resection or liver transplantation was indicated to a mere 25 - 30 % of patients. According to the generally accepted staging systems that are used as a standard at our Department for the evaluation of patients with HCC, these with preserved liver function were indicated for liver resection, those with poor hepatic function due to liver cirrhosis were qualified for liver transplantation. The rate of 5-year overall survival approximated up to 82%, and the tumor relapse at the 5-year follow-up did not exceed 25%. The experience we have gained so far indicates the need for new selection criteria that would be based, to a larger extent, on tumor biology [7,16,17].
The systems of clinical classification that are currently used for the selection of patients with hepatocellular carcinoma allow to estimate the grade of liver function, stage of tumor development, and provide the rationale for the treatment option. Unfortunately, none of them involves the correlation of the tumor stage and the tumor aggressive proprieties with the treatment outcome, in general. Thus, the prognosis remains partially unpredictable due to the unique biology of the tumor [14,18,19]. As it was shown in our study, the patients for liver resection were characterized by single, different in size, non-advanced tumors, and normal liver function; those for liver transplantation also had non-advanced, single or multifocal lesions that fulfilled the Milan criteria, and liver failure; those selected for the palliative treatment had extremely advanced pathological changes. Although, the presentation and the status of each patient qualified to the most suitable option of treatment seemed to be uniform from the clinical point of view, the patients differed significantly by the variations of the tumor histologic architectural growth pattern, the stage of tumor differentiation, and other biological proprieties, as indicated by an explant histologic analysis. Thus, even within the same group, the patients presented with different levels of tumor angiogenesis potential, as it was shown in our study by the significantly different values and levels of the soluble angiogenesis factors. Undoubtedly, the reference criteria on which we based the selection of patients may seem to be very deceptive. This is stressed in many studies reporting the importance of the unique tumor biology [5,8,14,18].
A previous study from our group reported an effective identification in the peripheral circulation of HCC patients of Hematopoietic Stem Cells (HSCs) and Endothelial Progenitor Cells (EPCs). The study conducted on 133 patients with HCC showed that the rates of hematopoietic stem cells, as well as the rates of endothelial progenitor cells, increase in the peripheral blood circulation of patients with liver cirrhosis, reaching the highest level in patients with HCC, in comparison to the volunteers with a healthy liver. Moreover, it was shown that the rate of hematopoietic stem cells within the white blood cells (%HSCs/WBC) gradually increases whereas the rate of Endothelial Progenitor Cells within the fraction of Hematopoietic Stem Cells (%EPCs/HSCs) gradually decreases depending on the stage of clinical tumor development [19,20]. Both cell fractions are known as the timber for tumor angiogenesis. According to many reports, the positive reaction with the monoclonal antibodies CD34, CD133, and CD309 is the characteristic and most restrictive form of determining their phenotype sand recognizing them in the population of white blood cells [11,21,22]. As indicated by other researchers, increased rates of progenitor cells were found in the peripheral circulation of HCC patients in contrast to healthy subjects and to non-tumor patients with liver cirrhosis. Gradual changes of both these biomarkers are also observed in Child�s B and C patients with liver cirrhosis as compared to those in Child�s A. The results confirmed the suggestions of the potential clinical utility encouraged by the others [10,12,20,22].
The important finding of the present study is that the rates of cells participating in tumor angiogenesis vary inpatients selected to the same treatment option by the standard and well established systems of classification. Certainly, such results should not surprise since patients present with different kinds of tumors. Despite the similarities in the clinical settings and the parallel status of the patients at the time of the presentation that lead to the appropriate treatment modality, patients differ from one another very much by the type of the tumor architectural growth pattern and the presence of microvascular invasion to the surrounding liver tissue. Thus, the variation in the rates of hematopoietic stem cells and endothelial progenitor cells seems to indicate the principal importance of the tumor biology for the angiogenesis potential of HCC, this means for the course of the disease and the ultimate treatment outcome. The suggestion is strongly supported by the findings indicating significant divergence in the levels of the laboratory data (INR, platelet counts, and alpha-fetoprotein) as well as in the values and levels of angiogenesis fostering agents varying according to the tumor biology. The differences in the levels of both cell fractions (HSCs and EPCs), that are known to be the timber for new vessels creation, seemed to be dependent upon the tumor architectural growth pattern and the grading of the tumor dissimilarity. A similar and significant interdependence occurred between the tumor tissue expressions of the VEGFR-2and the rates of circulating progenitor cells. The rates of hematopoietic stem cells (HSCs) and endothelial progenitor cells (EPCs) correlated significantly with the expression of the VEGFR-2 in the tumor tissue, and with the level of the serum VEGF cytokine concentration in the peripheral blood circulation. Nevertheless the suggestions indicating gradual changes in the level of the circulating hematopoietic stem cells and the endothelial progenitor cells from the tumor angiogenesis proprieties should yet be verified.
The potential prognostic implications of the present findings correspond to the results reported by others in the field of non-invasive measuring tumor parameters [15-12,22]. The biologic characteristics of the tumor were shown to be critical in determining the invasiveness and prognosis of HCC [2,8,18]. Beerepoot et al. [19] reported a functional analysis indicating an increase in circulating endothelial cells in patients with progressive disease, and showed that the cell level could be modulated by chemiotherapy. Baocun Sun et al. [8] reported an association of the endothelial cells and vasculogenic mimicry with the high tumor grade. The mechanisms of endothelial progenitor cell recruitment into the new vessels in HCC as well as the mechanisms of the capilarization that occurred according to the tumor growth, development and differentiation were described [2,9,18-24].
A reliable classification of the HCC patients and a responsible outcome prediction, especially concerning the surgical modalities of treatment, are still under discussion. The question is whether the measuring of the circulating angiogenesis biomarkers will be advantageous to other non-invasive methods for the purpose of the prognostic stratification. It is technically simple, easily accessible, and may provide information that could be available prior to the decision time. Being aware of the study limitations, and the ambiguous interpretation of the results, we would tend to support this approach.
Conclusions
The study supports the concept of mutual and positive relationship between the activity of progenitor cells and the progress of cancer. Thus, the identification of cells such as HSCs and EPCs in the peripheral blood of patients with HCC could assist in assessing the prognosis and the decision process of choosing the treatment method.
Acknowledgments
The authors wish to thank all cooperators from the Department of General, Transplant & Liver Surgery, the Department of Oncology, Haematology & Internal Medicine, and the Department of Pathology, Central University Hospital, Medical University of Warsaw for their contribution to this project.
Funding
This work was supported by the National Science Centre, Poland (grant No. NN 403 17794 [E154])
Declaration
The study protocol was approved by the Bioethics Committee of Medical University of Warsaw, and an informed consent was obtained from all patients undergoing the procedure
Authorship statements
| Name & Academic Degree | Wlodzimierz Otto, Professor of Surgery, MD, PhD |
| Department / Institution | General, Transplant & Liver Surgery, Medical University of Warsaw, Warsaw, Poland |
| E-mail Address | wotto@wum.edu.pl |
| Contribution to the paper | Study concept and design, acquisition of data, analysis and interpretation of the data, revision of the manuscript for intellectual content, drafting of the manuscript, study supervision, corresponding author |
| Conflict of interest | No conflict of interest |
| Name & Academic Degree | Maria Krol, MD |
| Department / Institution | Hematology, Oncology & Internal Medicine, Medical University of Warsaw, Warsaw, Poland |
| E-mail Address | makroll@post.pl |
| Contribution to the paper | Acquisition of data, cytometer analysis, interpretation of the data, revision of the manuscript for intellectual content |
| Conflict of interest | No conflict of interest |
| Name & Academic Degree | Urszula Wilkowojska |
| Department / Institution | Hematology, Oncology & Internal Medicine, Medical University of Warsaw, Warsaw, Poland |
| E-mail Address | grzewil5@wp.pl |
| Contribution to the paper | Acquisition of data, serologic analysis and interpretation of the data, revision of the manuscript |
| Conflict of interest | No conflict of interest |
| Name & Academic Degree | Ewa Wilczek, MD |
| Department / Institution | Dept. Pathology, Medical University of Warsaw, Warsaw, Poland |
| E-mail Address | ewa.wilczek@wum.edu.pl |
| Contribution to the paper | Histologic-pathologic study, acquisition of data, analysis and interpretation of the data, revision of the manuscript |
| Conflict of interest | No conflict of interest |
| Name & Academic Degree | Boguslaw Najnigier, MD |
| Department / Institution | General, Transplant & Liver Surgery, Medical University of Warsaw, Warsaw, Poland |
| E-mail Address | boguslaw.najnigier@wum.edu.pl |
| Contribution to the paper | Acquisition of data, drafting of the manuscript, administrative issues |
| Conflict of interest | No conflict of interest |
| Name / Academic Degree | Janusz Sierdzinski, PhD |
| Department / Institution | Medical Informatics and Telemedicine, Medical University of Warsaw, Warsaw, Poland |
| E-mail Address | jsierdzinski@wum.edu.pl |
| Contribution to the paper | Analysis and interpretation of the data, statistical analysis, drafting of the manuscript, corresponding author |
| Conflict of interest | No conflict of interest |
| Name / Academic Degree | Marek Krawczyk, Professor of Surgery, MD, PhD, Head of Department |
| Department / Institution | General, Transplant & Liver Surgery, Medical University of Warsaw, Warsaw, Poland |
| E-mail Address | marek.krawczyk@wum.edu.pl |
| Contribution to the paper | Critical revision of the manuscript for important intellectual content |
| Conflict of interest | No conflict of interest |
References
-
Trevisani F, Cantarini MC, Wands JR, Bernardi M (2008) Recent advances in the natural history of hepatocellular carcinoma. Carcinogenesis 29: 1299-1305.
-
Yang ZF, Poon RT (2008) Vascular changes in hepatocellular carcinoma. Anat Rec (Hoboken) 291: 721-734.
-
Welker MW, Bechstein WO, Zeuzem S, Trojan J (2013) Recurrent hepatocellular carcinoma after liver transplantation- an emerging clinical challenge. Transplant International 26: 109-118.
-
Chan EY, Larson AM, Fix OK, Yeh MM, Levy AE, et al. (2008) Identifying risk for recurrent hepatocellular carcinoma after liver transplantation: implications for surveillance studies and new adjuvant therapies. Liver Transpl 14: 956-965. .
-
Fan ST, Yang ZF, Ho DW, Ng MN, Yu WC, et al. (2011) Prediction of posthepatectomy recurrence of hepatocellular carcinoma by circulating cancer stem cells: a prospective study. Ann Surg 254: 569-576..
-
Guo RP, Zhong C, Shi M, Zhang CQ, Wei W, et al. (2006) Clinical value of apoptosis and angiogenesis factors in estimating the prognosis of hepatocellular carcinoma. J Cancer Res ClinOncol 132: 547-555.
-
Dudek K, Kornasiewicz O, Remiszewski P, Kobryn K, Ziarkiewicz-Wroblewska B, et al. (2009) Impact of tumor characteristic on the outcome of liver transplantation in patients with hepatocellular carcinoma. Transplant Proc 41: 3135-3137.
-
Sun B, Zhang S, Zhang D, Du J, Guo H, et al. (2006) Vasculogenic mimicry is associated with high tumor grade, invasion and metastasis, and short survival in patients with hepatocellular carcinoma. Oncol Rep 16: 693-698.
-
Franchito A, Onori P, Renzi A, Carpino G, Mancinelli G, et al. (2013) Expression of vascular endothelial growth factor and their receptors by hepatic progenitor cells in human liver diseases. Hepatobiliary Surg Nutr 2: 2304-2312.
-
Yegin EG, Siykhymbayew A, Eren F, Bekiroglu N, Ozdogan OC (2013) Prognostic implication of serum vascular endothelial growth factor in advanced hepatocellular carcinoma staging. Ann Hepatol 12: 915-925.
-
Zhu K, Dai Z, Zhou J (2013) Biomarkers for hepatocellular carcinoma: progression in early diagnosis, prognosis, and personalized therapy. Biomark Res 1: 10.
-
Chen CH, Chang LT, Tung WC, Chen YL, Chang CL, et al. (2012) Levels and values of circulating endothelial progenitor cells, soluble angiogenic factors, and mononuclear cell apoptosis in liver cirrhosis patients. J Biomed Sci 19: 66.
-
Mathonnet M, Descottes B, Valleix D, Labrousse F, Denizot Y (2006) VEGF in hepatocellular carcinoma and surrounding cirrhotic liver tissues. World J Gastroenterol 12: 830-831.
-
Paradis V (2013) Histopathology of hepatocellular carcinoma. Recent Results Cancer Res 190: 21-32.
-
Poon RT, Ng IO, Lau C, Zhu LX, Yu WC, et al. (2001) Serum vascular endothelial growth factor predicts venous invasion in hepatocellular carcinoma: a prospective study. Ann Surg 233: 227-235.
-
Grat M, Kornasiewicz O, Lewandowski Z, Skalski M, Zieniewicz K, et al. (2013) The impact of surgical technique on the results of liver transplantation in patients with hepatocellular carcinoma. Ann Transplant 18: 448-459.
-
Grat M, Kornasiewicz O, Holowko W, Lewandowski Z, Zieniewicz K, et al. (2013) Evaluation of total tumor volume and pretransplantation a-fetoproteine level as selection criteria for liver transplantation in patients with hepatocellular carcinoma. Transplanation Proceedings 45:1899-1903.
-
Eguchi S, Takatsuki M, Hidaka M, Soyama A, Tomonaga T, et al. (2010) Predictor for histological microvascular invasion of hepatocelular carcinoma: a lesion from 229 consecutive cases of curative liver resection. World J Surgery 34: 1034-1038.
-
Beerepoot LV, Mehra N, Vermaat JSP, Zonnenberg BA, Gebbing MFGB, et al. (2004) Increased levels of viable circulating endothelial cells are an indicator of progressive disease in cancer patients. Annals of Oncology 15: 139-145
-
Otto W, Krol M, Maciaszczyk M, Sierdzinski J, Najnigier B, et al. (2013) Identification and significance of circulating endothelial progenitor cells in patients with hepatocellular carcinoma. Nowotwory Journal of Oncology 5: 383-394.
-
Krol M, Urbanowska E, Feliksbrot M (2005) Phenotype characteristic CD34+ cells from umbilical cord-derived blood and products of leucoferesis in stimulated healthy donors. Adv Clin Exp Med 14: 877-884.
-
Fadini GP, Baesso I, Albiero M, Sartore S, Agostini C, et al. (2008) Technical notes on endothelial progenitor cells: ways to escape from the knowledge plateau. Atherosclerosis 197: 496-503.
-
Yu DC, Chen J, Sun XT, Zhuang LY, Jiang CP, et al. (2010) Mechanism of endothelial progenitor cell recruitment into neo-vessels in adjacent non-tumor tissues in hepatocellular carcinoma. BMC Cancer 10: 435.
-
Tseng PL, Tai MH, Huang CC, Wang CC, Lin JW, et al. (2008) Overexpression of VEGF is associated with positive p53 immunostaining in hepatocellular carcinoma (HCC) and adverse outcome of HCC patients. J Surg Oncol 98: 349-357.
