A 45-year-old woman came to the internal Medical School A of Mohammed V Military Hospital, complaining of mild recurrent epistaxis related to telangiectasia at the nasal septum and chronic iron deficiency anemia requiring frequent blood transfusions with iron infusions.
During his physical exam, we noticed telangiectasia lesions spread throughout her lower lip, tongue (Figure 1A), face, soft palate (Figure 1B) and outer ear (Figure 1C). Doing anterior rhinoscopy, we noticed hematic points on her septal mucosa and her right middle turbinate.
The diagnosis of Rendu-Osler disease has been mentioned. In the genetic study, A deleterious mutation c.52del.p.val18* was found on the AVCRL1 gene. Biological examinations showed anemia at 9 g/dL with ferritinemia at 6 μg/L (normal > 25), and anicteric hepatic cholestasis with alkaline phosphatases at 415 U/L (normal < 120). Esogastroduodenal fibroscopy did not find angiodysplastic lesions. Hepatic Doppler ultrasound, then thoracoabdominal computed tomography (CT) revealed a dilated common hepatic artery, 5 mm in diameter, without other arteriovenous malformations.
There was no improvement, despite nasal mechage, iron infusion and repeated blood transfusions. The patient was treated with bevacizumab at a dose of 5 mg/kg/infusion every 2 weeks and was given 6 cycles.
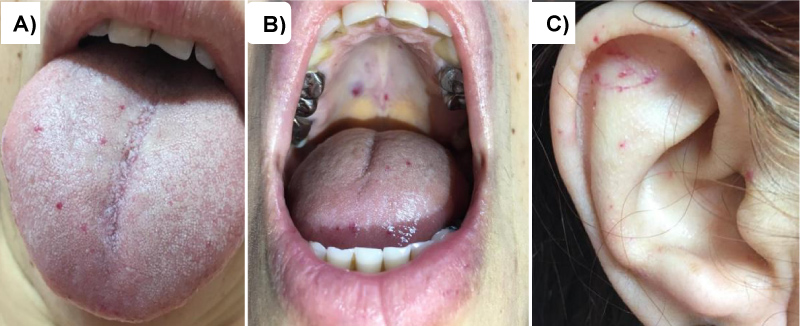
Figure 1: Telangiectasia lesions, A) Tongue, B) Soft palate, C) Outer ear.