The brachial plexus which innervates the upper limb has afferent from the cervical and thoracic part of the spinal cord. Due to its proximity to the other important vascular and nervous structures, which is mainly responsible for the post block complications like temporary paralysis of the phrenic, recurrent laryngeal nerves or Horner's syndrome [1,2].
Horner's Syndrome consists of the set of signs and symptoms which manifest due to the blockade of the ipsilateral sympathetic pathway that innervates head, face and eye. It mainly presents with the triad of ptosis, miosis and anhidrosis [3]. Various studies have reported occurrence of Horner syndrome after interscalene brachial plexus block to be between 4-37.5% depending upon block technique, drug volume, concentration, and mode of delivery like a single bolus injection or a continuous infusion [4].
We describe a case of 22 years young male weighing 65 kg, with no comorbidities, having proximal humerus fracture was planned for open reduction and internal fixation. Plan of anesthesia was ultrasound (US) guided interscalene brachial plexus block. Block preparation was done as per institutional protocols. Block was performed with the patient in supine position with the patient's head facing away from the side to be blocked. The knowledge of anatomical landmarks substantially facilitates and shortens the time to obtain the desired ultrasound image for an in-plane approach. Under all aseptic and antiseptic precautions, and under the guidance of US, anatomical land marks were identified. The tissue space between anterior and middle scalene muscles was identified. The needle was inserted in-plane toward the brachial plexus. A small volume of saline is injected through the needle to confirm proper needle placement. After confirmation, Inj. Ropivacaine (0.5%, 20 ml) was given. After ten minutes, patient started to develop redness in eye (Figure 1A, Chemosis), unequal pupil size (Figure 1B, Miosis) and dropping of eyelid (Figure 1C, Ptosis) of same side where block was performed. The above clinical triad was suggestive of Horner's syndrome. The patient was observed in preoperative area and symptoms resolved by the time surgery were done. Postoperative course was uneventful.
None.
None.
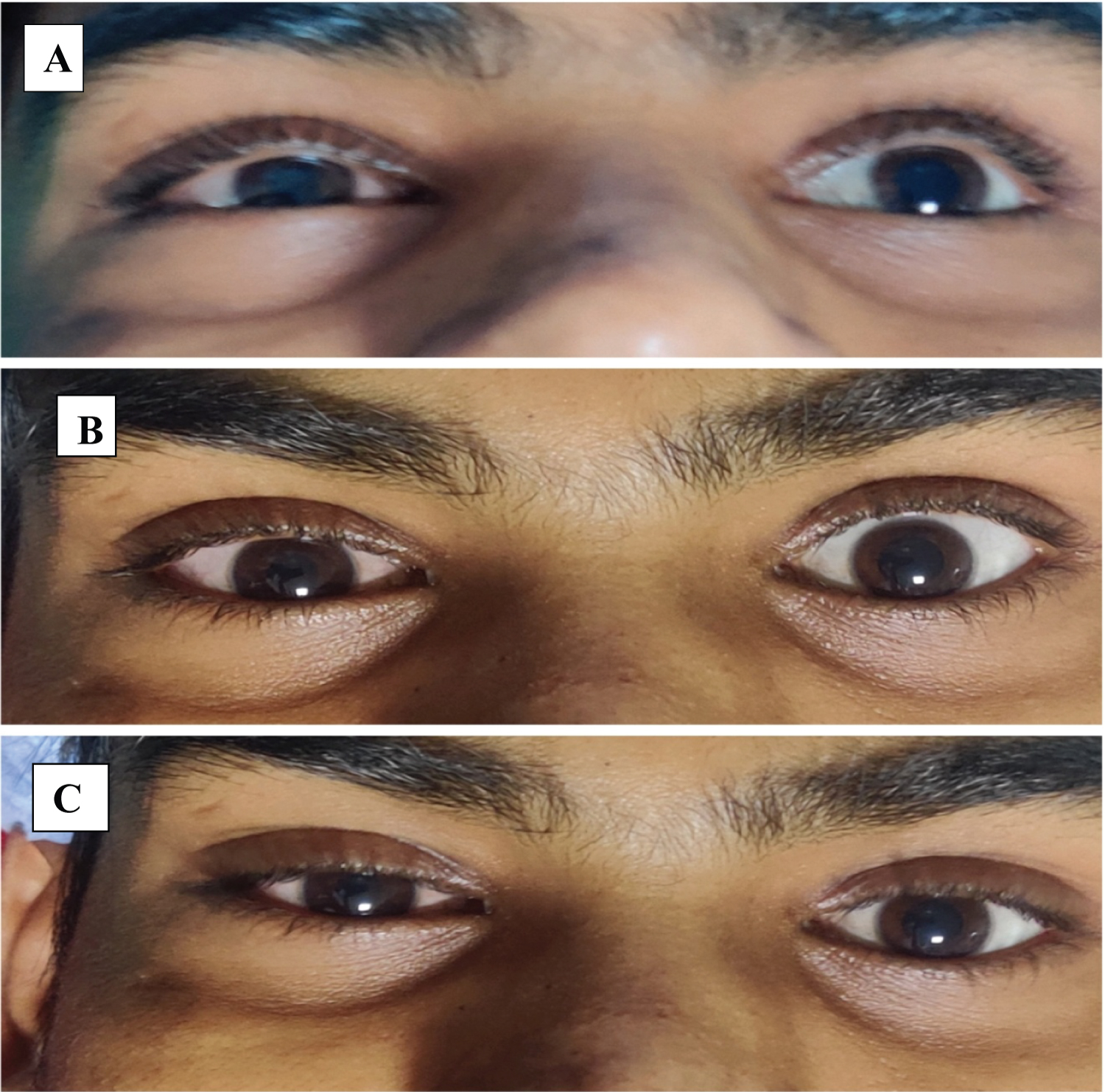
Figure 1: Figure showing presence of chemosis (A), miosis (B) ptosis (C).