Brunner's gland, Hyperplasia, Ampulla of vater, Epigastric pain, Unusual cause
A 49-year-old man with a history of chronic hepatitis B presented to our outpatient clinic with occasional epigastric pain and intermittent fullness lasting 3 months. Duodenoscopy revealed ~1.5-cm broad-based polypoid ampullary mass with smooth and hyperemic mucosa (Figure 1A).
Endoscopic ultrasonography (EUS) revealed an ampullary mass with hypoechoic and heterogeneous echogenicity involving mucosal and submucosal layers without an evidence of extension into either the biliary or pancreatic duct (Figure 1B). Further, Endoscopic papillectomy (EP) was performed to remove the mass (Figure 2A), and a plastic stent was placed into the pancreatic duct to reduce the risk of postprocedural pancreatitis (Figure 2B). The histological examination showed marked Brunner's gland hyperplasia with proliferating lobular-shaped Brunner's glands separated by fibrous septa and cystic dilatations of the glandular acini and ducts (Figure 2C, hematoxylin-eosin staining, 40x). The patient was finally diagnosed with Brunner's gland hyperplasia (BGH) of the ampulla of Vater. He was discharged after EP without any complications.
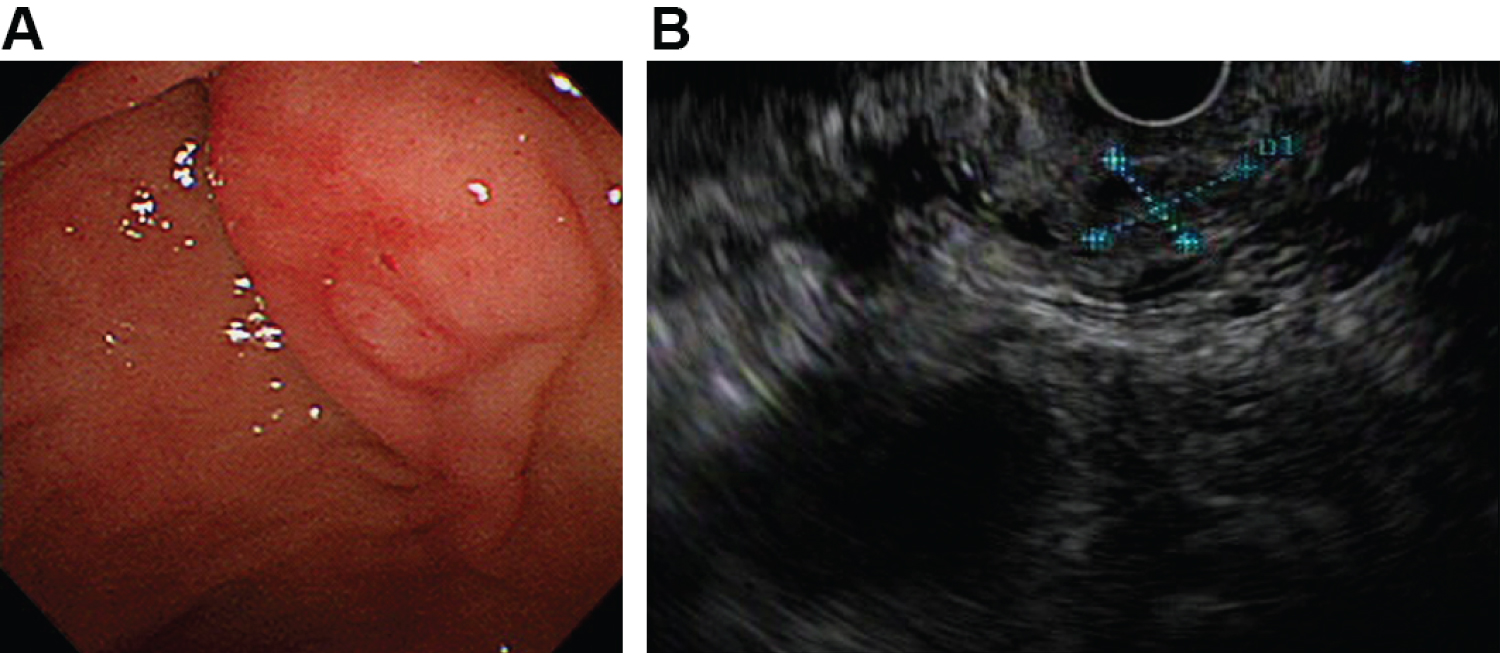 Figure 1: A) Duodenoscopy revealing a 1.5-cm broad-based polypoid ampullary mass with smooth and hyperemic mucosa; B) Endoscopic ultrasonography performed using the olympus GF-UCT260 linear-array echoendoscope indicating a heterogenous hypoechoic mass located in the mucosal and submucosal layers. View Figure 1
Figure 1: A) Duodenoscopy revealing a 1.5-cm broad-based polypoid ampullary mass with smooth and hyperemic mucosa; B) Endoscopic ultrasonography performed using the olympus GF-UCT260 linear-array echoendoscope indicating a heterogenous hypoechoic mass located in the mucosal and submucosal layers. View Figure 1
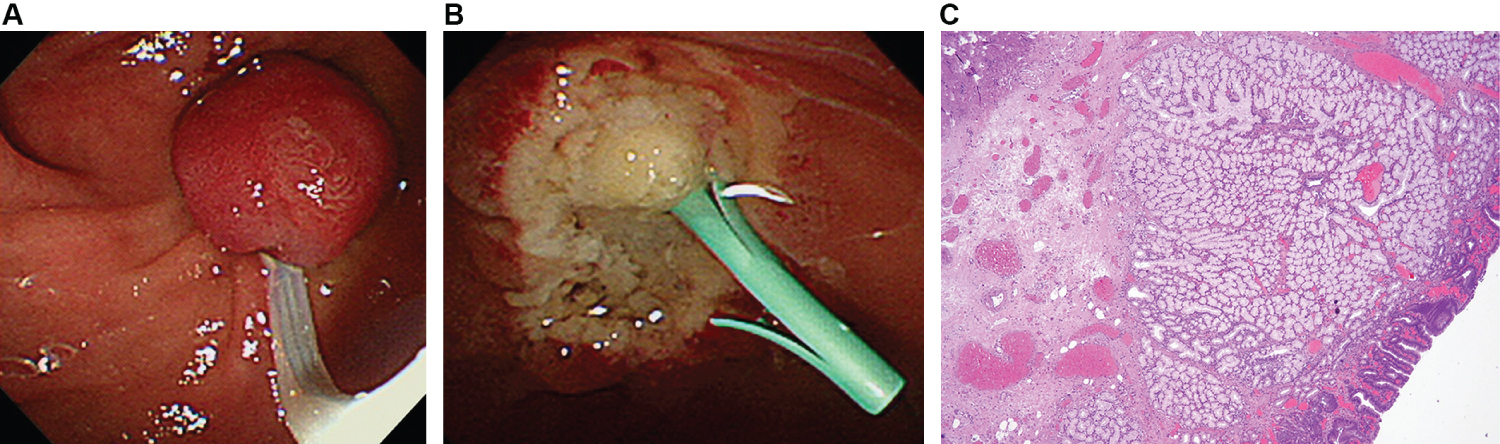 Figure 2: A) Endoscopic papillectomy performed for the removal of ampullary mass; B) A plastic stent placed into pancreatic duct to reduce the risk of postprocedural pancreatitis; C) Histopathological examination of the duodenal lesions by hematoxylin and eosin staining (x40 magnification) showed Brunner's glands with a lobular configuration separated by fibrous septa and some cystic dilatations of the glandular acini and ducts. View Figure 2
Figure 2: A) Endoscopic papillectomy performed for the removal of ampullary mass; B) A plastic stent placed into pancreatic duct to reduce the risk of postprocedural pancreatitis; C) Histopathological examination of the duodenal lesions by hematoxylin and eosin staining (x40 magnification) showed Brunner's glands with a lobular configuration separated by fibrous septa and some cystic dilatations of the glandular acini and ducts. View Figure 2
BGH rarely occurs at the ampulla of Vater. BGH presents sporadically and is accompanied by abdominal pain, hemorrhage, jaundice, or obstruction [1]. Endoscopically, BGH may appear as solitary or multiple and mucosal or submucosal nodules, and may manifest as a heterogenous hypoechoic mass located in the mucosal and submucosal layers on EUS [2]. For treatment, surgical resection has been used to treat ampullary BGH [3,4]. Nevertheless, by offering a safe and effective alternative to surgery that enables a correct diagnosis, EP is considered to be the first-line treatment in patients with benign ampullary masses [3-5]. However, the application of EP for treatment of ampullary BGH has not been reported yet. Herein, we report this ampullary mass with unusual imaging features to indicate that BGH should be the mostly suspected diagnosis and EP can be considered after the completion of a more definite evaluation including EUS.
All authors declare they have nothing to disclose.
None.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
This paper does not contain any identifiable data of any participant in any form; hence, this section is not applicable.
The concept and design of the study: Yi Hua Wu, Wen Hsin Huang; Statistical analysis: Chi Ying Yang; Interpreted the results: Kai-Po Chang; Analyzed the data and drafted the manuscript: Yi Hua Wu.