Objective: It is well-established that vertebroplasty has effects on sagittal parameters due to various pathologies of the spine. Our objective in the study was to reveal the impact of vertebroplasty that was applied to compression fractures due to trauma on sagittal parameters.
Material and method: Fourteen patients with the injury score > 4, based on the thoracolumbar injury classification score (TLICS), and with type A fractures, based on the AO Spine thoracolumbar injury classification score (TLAOSIS), were included in the study. Scoliosis radiographs were shot preoperatively and at 1st, 6th, and 12th months during the postoperative period, and measurements were performed using the software of Surgimap (Nemaris, Inc). Spinopelvic parameters of each patient including pelvic incidence (PI), sacral slope (SS), pelvic tilt (PT), lumbar lordosis (LL), thoracic kyphosis (TC), thoracolumbar kyphosis (TLC), cervical lordosis (CL), and sagittal vertical axis (SVA) were assessed. Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI) assessments of the patients were performed as well. Moreover, health-related quality of life was assessed with the Medical Outcome Study Short Form-36 prior to surgery and in the 1st month following the surgery.
Results: Spinopelvic parameter values of the patients were assessed statistically through the analysis of the Friedman test before surgery, and in the 1st month, 6th month, and 12th month during the postoperative period. It was found out that the changes in the pelvic tilt and sacral slope values of the patients between preoperative and 1st month, 6th month and 12th month, 1st month and 6th month, 1st month and 12th month, 6th month and 12th month were at the level of p = 0.37, and the changes were not significant. The change in lumbar lordosis value was p < 0.01 and was significant. The changes in thoracolumbar kyphosis values at preoperative and 1st month, preoperative and 6th month, as well as preoperative and 12th month, were p < 0.001, and the changes were significant. The changes in thoracic kyphosis values between preoperative and 1st month, preoperative and 6th month, as well as preoperative and 12th month, were at the level of p < 0.001 and the changes were significant. The changes in cervical lordosis and sagittal vertical axis values at preoperative and 1st month, preoperative and 6th month, as well as preoperative and 12th month, were at p = 0.002 and p < 0.001, respectively, and they were significant. Statistical analysis of the values of the Visual Analog Scale and Oswestry Disability Index Medical Outcome Study Short Form-36 life quality scale was p < 0.001, based on the results of the Friedman test, and significant.
Conclusion: Vertebroplasty is an efficient technique for relieving pain in thoracic fractures that have a score of 4 and over, based on the thoracolumbar injury classification score (TLICS), and that are type A, based on the AO Spine thoracolumbar injury classification score (TLAOSIS). Elimination of pain in the acute period is effective in ameliorating the sagittal parameters of patients.
Vertebroplasty, Sagittal parameters, Thoracic fracture
Sagittal balance is the optimal standing posture of a person through using the minimum energy. It attempts to ensure this balance with the bone morphology, the structures of the discs, muscles, and ligaments as well as by the compensation mechanisms against the potential deterioration that might occur in them [1]. Vertebral fractures occur due to changes in the structure of the bone. Percutaneous vertebroplasty (PVP) is a well-accepted, safe and effective minimally invasive treatment method for the treatment of vertebral compression fractures, which are induced by osteoporosis, trauma, malignancy, and metabolic causes [2,3]. It ensures stabilization in the treatment of minor fractures of the vertebra, which does not lead to neurological deficits, while the exothermic reaction feature of the cement used during the procedure blocks pain receptors by damaging the nerve endings that convey pain. It provides both stabilization and has an impact on pain [4].
Studies related to the impact of sagittal parameters of local kyphosis due to vertebral compression fractures have been reported in the literature. Our objective in this study is to reveal the effects of vertebroplasty on the global sagittal alignment in trauma-related fractures.
The patients who presented with spinal fractures due to trauma between January 2019 and December 2021 in Bahcelievler Memorial Hospital were included in the study.
Inclusion criteria for the patients participated in the study:
1. Those with the injury score > 4, based on the thoracolumbar injury classification score (TLICS)
2. Those with type A fractures, based on the AO Spine thoracolumbar injury classification score (TLAOSIS) (Figure 1)
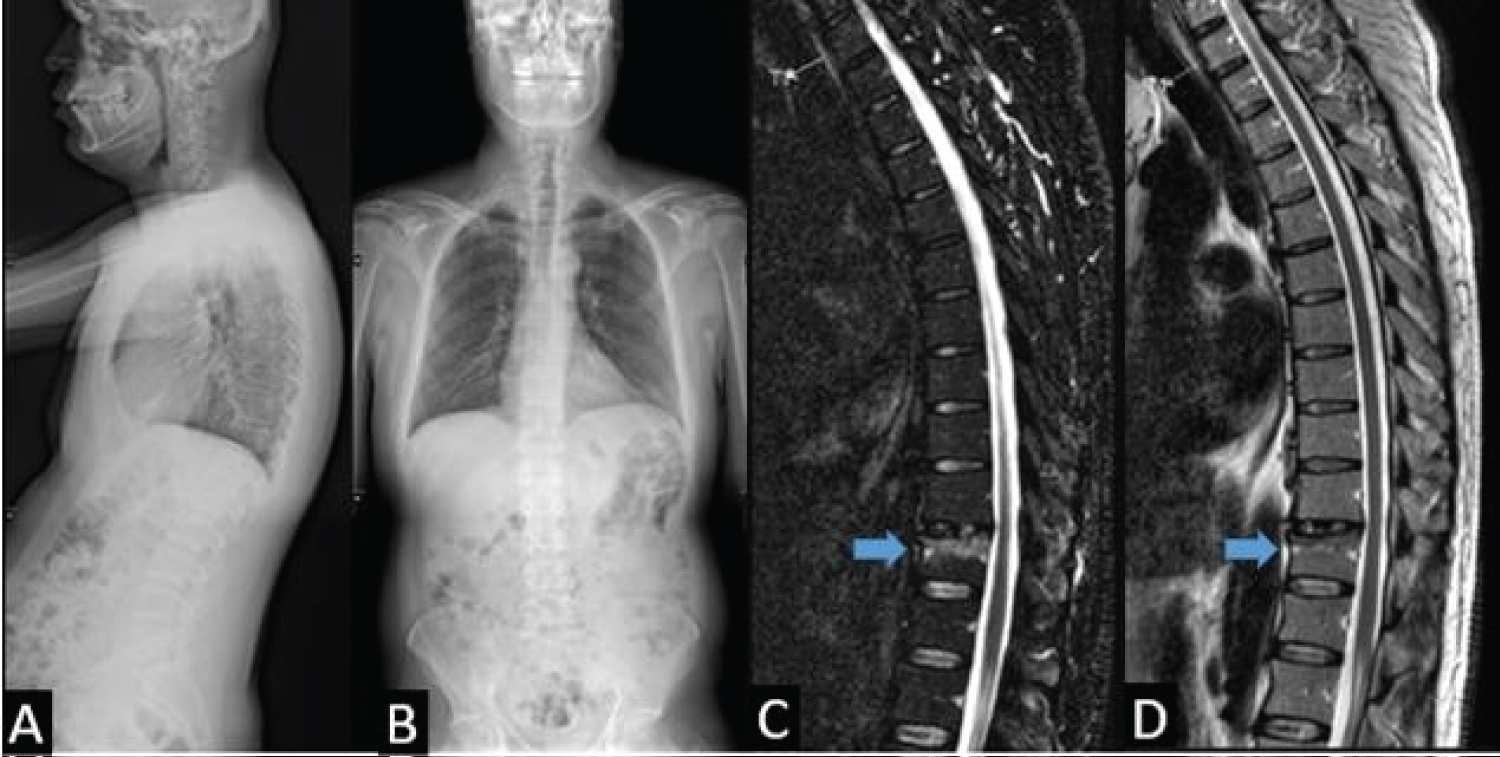 Figure 1: Thoracic 11 vertebra Type A1 fracture according to the AO Spine thoracolumbar injury classification. A) Lateral scoliosis radiograph; B) Posterioanterior scoliosis radiograph; C) Short tau inversion recovery magnetic resonance imaging, blue arrow, edema; D) T2- weighted image, blue arrow, edema.
View Figure 1
Figure 1: Thoracic 11 vertebra Type A1 fracture according to the AO Spine thoracolumbar injury classification. A) Lateral scoliosis radiograph; B) Posterioanterior scoliosis radiograph; C) Short tau inversion recovery magnetic resonance imaging, blue arrow, edema; D) T2- weighted image, blue arrow, edema.
View Figure 1
3. The patients with severe back pain that does not relieve despite medication and rest, which lasted for three weeks or more
4. The patients with a visual analog scale (VAS) 7 and above
Exclusion Criteria:
1. Patients with neurological deficits
2. Those with a traumatic disc
3. Non-type A fractures, based on the TLAOSIS
4. The patients who have local infection at the application site
5. The patients with bleeding diathesis
6. The patients with a known medical history of allergies to the substances to be administered
Upon informing all patients verbally and in writing about the procedure, written consent forms were obtained from all of them that they gave consent to the application. The ethics approval of the Istanbul Bahcelievler Memorial Hospital ethics committee was obtained.
20 patients were included in the study in accordance with the above-mentioned criteria. Standard scoliosis radiographs were obtained from all patients who met the admission criteria to assess the sagittal parameters. It was ensured that the appropriate intensity was maintained between the thoracic cavity, where the beam penetrates easily, and the lumbosacral region, where it is more challenging to penetrate by using a balancing filter between the patient and the X-ray source for a standard and high-quality capture. All shots were taken while the patients were standing. The patients were shot by keeping the legs with their knees together, with their feet shoulder-width apart, the elbows bent, and their hands closed bilaterally in the subclavicular fossa. The sagittal parameters of the patients were measured preoperatively and at first month postoperatively.
The spinopelvic values were measured via Surgimap (Nemaris, Inc), using scoliosis radiographs. Spinopelvic parameter measurements including pelvic incidence (PI), sacral slope (SS), pelvic tilt (PT), lumbar lordosis (LL), thoracic kyphosis (TK), thoracolumbar kyphosis (TLK), cervical lordosis (CL), and sagittal vertical axis (SVA) were made for each patient. The sagittal parameters of the patients were measured preoperatively and at first month postoperatively. Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI) assessments of the patients were performed preoperatively and at first month during the postoperative period.
The patients were placed in the prone position with the table neutral under general anesthesia. Following the completion of sterile procedures, the fractured vertebra was detected via a C-arm scope. All applications were performed using the unilateral and transpedicular approach. After the skin-subcutaneous infiltration with 1% lidocaine, a 0.5 cm long incision was performed on the skin with a scalpel. An 11 G 150 mm long vertebroplasty needle (SOMATEX® Medical Technologies, Teltow, Germany) was inserted through this incision towards the upper outer part of the pedicle. Forward movements were performed through a c-arm scope, utilizing anteroposterior and lateral views. Once the needle reached the cortex, the procedure was carried on using the lateral view. Upon passing the cortex, the tip of the needle was advanced to the anterior third of the corpus. At this phase, bone cement (Vertebro X, SOMATEX® Medical Technologies, Teltow, Germany) was begun to be prepared. After waiting until the cement consistency reached toothpaste-like consistency, the cement in the 2 ml injectors was carefully injected into the fractured vertebral corpus under the guidance of fluoroscopy. If no problem was experienced, cement injection was continued until the cementum reached the posterior third border of the corpus and, at the same time, until it was observed that the cementum passed to the opposite side in the AP image. Upon achieving sufficient filling of the vertebral corpus, the insertion site was dressed, and the procedure was completed. After completing the procedure, a fluoroscopy image was shot for follow-up (Figure 2). After the patient was awakened, neurological examinations were conducted, and he was transferred to the service. The patients who were followed up throughout one day following the procedure were discharged upon. Control scoliosis radiography was performed preoperatively and in the first month after surgery (Figure 3). Spinopelvik parameters of the captured scoliosis radiographs were remeasured through the software of Surgimap on the computer (Figure 4).
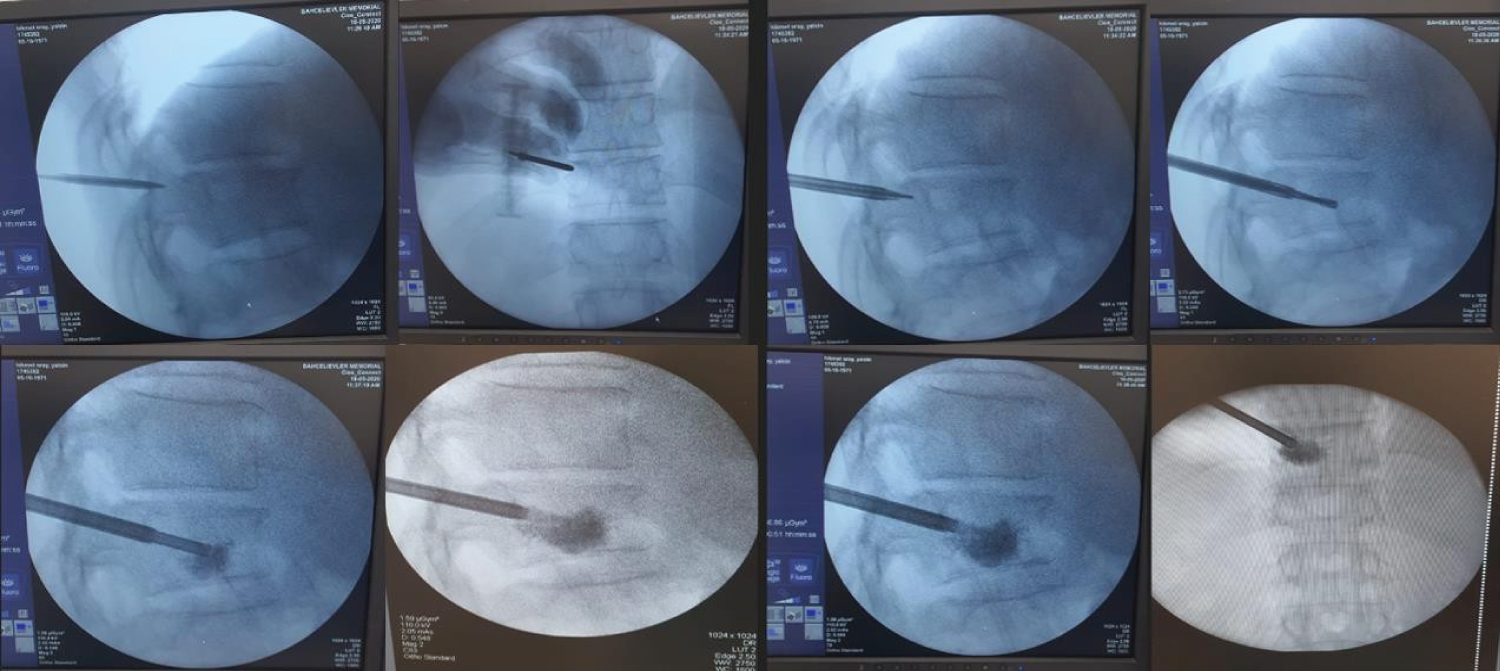 Figure 2: Vertebroplasty for Thoracic 11 vertebral fractures under the guidance of fluoroscopy.
View Figure 2
Figure 2: Vertebroplasty for Thoracic 11 vertebral fractures under the guidance of fluoroscopy.
View Figure 2
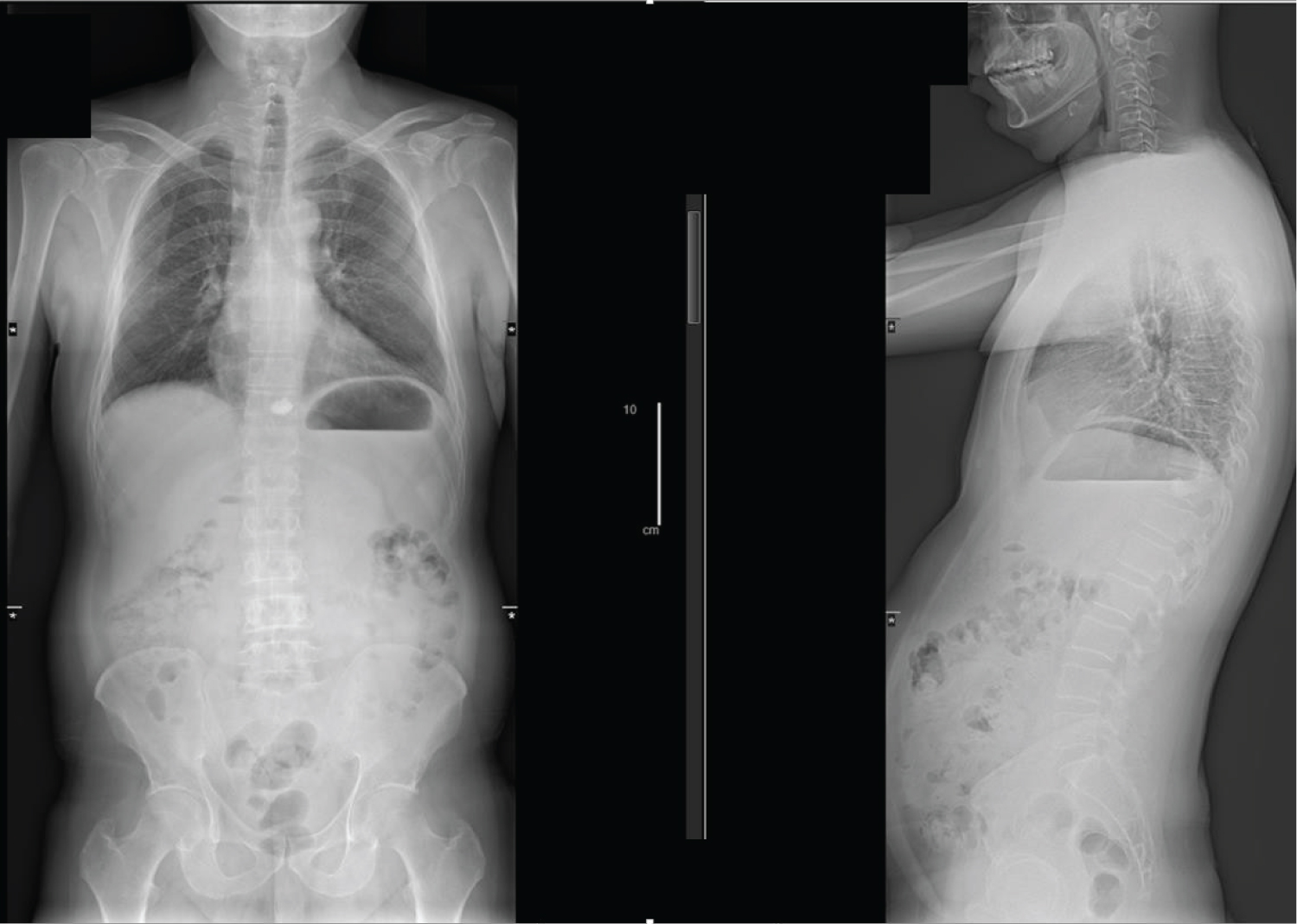 Figure 3: Control scoliosis radiography after undergoing vertebroplasty for the 11th thoracic vertebra (T11).
View Figure 3
Figure 3: Control scoliosis radiography after undergoing vertebroplasty for the 11th thoracic vertebra (T11).
View Figure 3
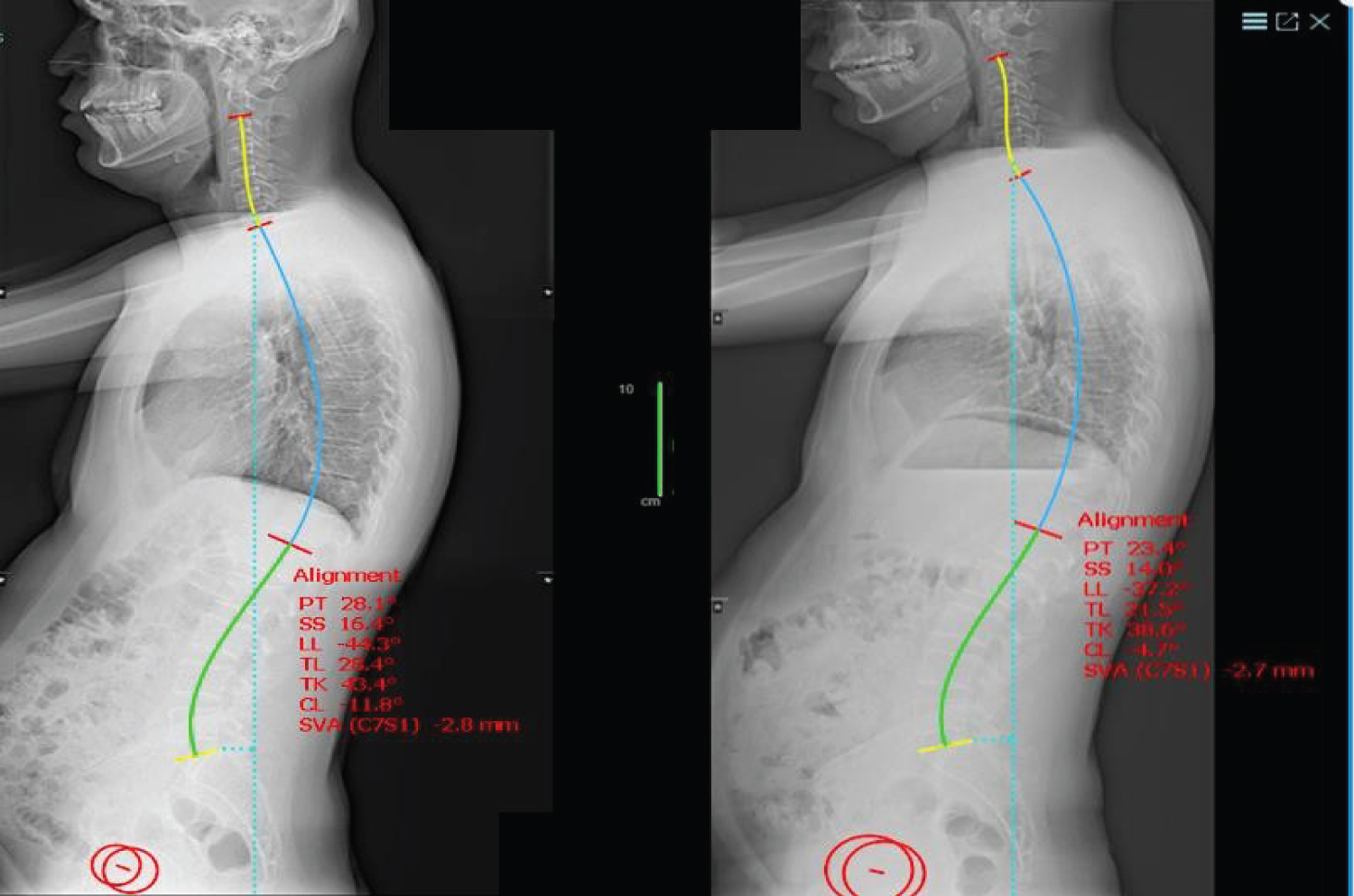 Figure 4: The spinopelvic parameters measured using the Surgimap before and after undergoing vertebroplasty.
View Figure 4
Figure 4: The spinopelvic parameters measured using the Surgimap before and after undergoing vertebroplasty.
View Figure 4
A total of 20 patients (consisting of 12 females and 8 males) with a score of 4 > according to the TLICS, as well as who had type A fractures, based on the TLAOSIS classification, between 8th thoracic and 12th thoracic were included in the study. The age of the patients ranged between 38 and 61, and the mean age was 47.42. The mean age was 47.25 for females and 47.66 for males. Distribution of the fractures regarding levels in a total of 20 patients were as follows; at T12 in 55% (11 patients) of them, at T11 in 25% (5 patients) of them, at T10 in 5% (1 patient) of them, at T9 in 10% (2 patients) of them and T8 in 5% (1 patient). PI, PT, SS, LL, TK, TLK, CL, and SVA values of the spinopelvic parameters during the preoperative period and at first month during the postoperative period were assessed statistically through the analysis of the Paired Samples test. It was determined that the changes in the PT, SS and LL values of the patients between preoperative and first month postoperative were at the level of p = 0.659, p = 0.716, p = 0.012; and the changes were not significant. It was determined that the changes in the TL, TK, CL and SVA values of the patients between preoperative and first month postoperative were at the level of p < 0.001 and the changes were significant based on the results of the Paired Samples test (Table 1).
Table 1: Statistical data of sagittal parameters (PRE: Preoperative, POST: Postoperative, first month). View Table 1
VAS and ODI values of the patients in the preoperative period, and in the first month during the postoperative period are separately presented in Table 2 as minimum, maximum, mean, and standard deviation. To analyze the data Wilcoxon Signed Ranks Test was used. Statistical analysis was conducted by an independent statistician who was blind to surgical procedures. Statistical analysis of VAS and ODI values was p < 0.001, and the results were significant based on the Wilcoxon Signed Ranks test. Statistically significant values are summarized in Table 2.
Table 2: Statistical data of VAS and ODI scales (PRE: Preoperative, POST: Postoperative, first month, Min: Minimum, Max: Maximum). View Table 2
The primary objective of vertebroplasty is to ensure stabilization and reduce pain through the impact of heat by placing bone cement on the corpus part of the fractured vertebra [5]. There are previously published articles about the effects of vertebral body fractures on sagittal balance [6]. Anterior wedge deformities develop in compression fractures due to osteoporosis, and hence, kyphotic changes occur. The affected vertebral is not limited to the kyphosis fractured area of the vertebra, but it also influences the global spine alignment. The increase in kyphosis due to fracture would displace the SVA forward. Ultimately, this will lead to the center of gravity in the vertebra to shift forward. Lumbar region wedge deformity, improvement in lordosis, wedge deformity in the thoracic area, an increase in thoracic kyphosis, and an increase in SVA in both cases occur [7]. Increased thoracic hyperkyphosis due to increased sagittal imbalance can be compensated by the increase in lumbar lordosis [8]. Kyphoplasty application induces the forward displacement of the SVA and enables sagittal balance by fixing the kyphotic deterioration by providing bone restoration of sagittal deformities [9]. Postoperative recovery in SVA following kyphoplasty is also associated with the correction of this angulation [10]. Particularly kyphoplasty ameliorates the condition of the pelvis by providing a sagittal balance on the pelvic retroversion that occurs in osteoporotic fractures [11]. In addition to bone restoration, it has a corrective effect on sagittal alignment through relieving pain caused by the fracture [12]. There are also studies in the literature related to the effects of the factors, which cause low back and back pain, on sagittal balance. Both lumbar lordosis and thoracic kyphosis are significantly reduced in degenerative disc diseases or disc diseases and are characterized by a flat spine. To prevent posterior overload in pain due to degeneration or disc disorder, lumbar lordosis and thoracic kyphosis secondary to the patient’s analgesic posture would wane, albeit this change is due to the loss of disc height in the degenerative process [13]. Changes occur in spinal parameters that are secondary to pain caused by paraspinal muscle pathologies. Lumbar lordosis and thoracic kyphosis decrease in cases impacting the lower lumbar region, whereas, in problems experienced in the muscle group of L2 and above, an increase occurs in SVA positive values associated with the rise of thoracic kyphosis [14]. Back extension muscles generate a preventive force against thoracic kyphosis. It has a protective effect on lordosis in the lumbar region. As it cannot generate its protective forces in muscle pathologies, it leads to the deterioration in sagittal balance [15,16]. In our study, we detected an increase in TK and TLK parameters following the fractures in the lower thoracic region. We considered that pain could cause deterioration in parameters by preventing the function of the muscle group, which has protective properties of the sagittal sequence, in line with the literature. Meanwhile, changes in the parameters of LL, CL, and SVA occur as a result of compensation mechanisms. We determined that the compensation mechanism disappeared with the complete relief in the pain and, thus, the sagittal parameters ameliorated in the period following the PVP application.
90% of traumatic spine fractures occur in the thoracolumbar region, and most of these are compression fractures. In compression fractures, the anterior column is influenced, and the posterior column and ligament structures are preserved. Stability depends on the angular deformity and the amount of collapse. Generally, less than 50% height loss and less than 20 degrees angular deformity are considered stable [17]. Thoracolumbar injury classification (TLICS), which is based on injury morphology, neurological condition, and ligament injury, has been used for surgical decisions in recent years. Based on this classification, surgery is recommended for patients who have above four points [18]. The general approach is to provide stabilization with short-segment posterior instrumentation, while the discussions on the surgical treatment method keep on. Yet, there is a risk of kyphotic deformity because of the weakness of the front column and the risk of system malfunctions due to overload on the system in this approach. Hence, cement-assisted instrumentation application is utilized to provide solutions to these problems [19]. There are few studies in the literature related to the use of VP in spine fractures caused by trauma. Chen, et al. revealed that there was a significant amelioration in pain, based on the results of VP application in patients with traumatic spine fractures where conservative treatment failed [20]. Huwart, et al. unveiled the successful results of computed tomography-guided VP application in traumatic spine fractures in their study, which was performed with a larger series of patients [21]. Likewise, we found out in our study that the VP application was effective on pain in traumatic fractures.
There are various studies related to the use of posterior instrumentation in thoracolumbar fractures and VP applications. It is basically revealed in these studies that VP application could be beneficial in preventing kyphotic angulation through providing support to the anterior of the fracture and preventing inadequacy, fusion problems, and adjacent segment disorders that might be induced by instrumentation, and also has favorable effects on the sagittal parameters to be obtained [22-25]. Moreover, no kyphosis angulation was detected in our study during a one-year follow-up. Thus, we are of the opinion that the VP application could have a protective effect in kyphosis angulation, and it could be a guideline in traumatic patients; though, it has a shorter follow-up period.
We determined as a result of our study that the VP application was efficient in pain control and an effective method on sagittal parameters in appropriately selected patient groups in thoracic fractures.
The limited number of cases and the short follow-up period are two primary factors that limit our study. There is a need for new studies with larger sized populations and longer follow-up periods to be performed in the future.
Vertebroplasty is an efficient technique for relieving pain in thoracic fractures that have a score of 4 and over, based on the thoracolumbar injury classification score (TLICS), and that are type A, based on the AO Spine thoracolumbar injury classification score (TLAOSIS). Elimination of pain in the acute period is effective in ameliorating the sagittal parameters of patients.
There is no declaration of conflict of interest.
There is no financial support for our work.