Operating theatres are heavily budgeted departments in health facilities. Theatre turnaround time (TAT) is used as one modality in determining the efficiency of health service delivery. Factors that correlate with TAT in the Kenyan setting are largely unknown. The main objective of this study was to determine the factors affecting turnaround time in Kenyatta National Hospital's main theatres.
This was a descriptive observational study done in September and October 2021. Data on personnel, surgical, equipment, consumable and infrastructural factors was collected. A structured questionnaire was administered both physically and digitally. Bivariate chi-square tests of association and multinomial logistic regression were used to evaluate the nature of the associations between the various factors and TAT.
There was a significant relationship between personnel, surgical, equipment, and consumable factors with TAT (p < 0.05). These included: prolonged nursing handover time (p = 0.000), staff shortage (p = 0.039), lack of support from theatre managers (p = 0.020), the urgency of surgery (p = 0.025), lack of blood (p = 0.000) and inadequacy in the supply of drapes and gowns (p = 0.019). There was availability of anesthesia machines (0.019), drugs (p = 0.041), stretchers, and wheelchairs (p = 0.022) reducing TAT. Others findings were unreliability of electricity (p = 0.011) and oxygen supply (P = 0.023) and difficulty accessing main theatres from the surgical wards and ICU (p = 0.000).
It is hoped that the study findings can be used to address the multiple factors affecting TAT and surgical patient service delivery.
Turnaround time, Operating theatre, Intensive care unit (ICU), Post-operative care unit (PACU).
Theatre turnaround time (TAT) is the time between a patient being taken to the post anaesthesia care unit (PACU) and the next patient being wheeled into the operating theatre [1,2]. It is the minimum time needed to clear theatre in preparation for the next case [3,4].
Operating theatre (OT) efficiency is directly associated with reduced TAT. There is improved patient outcome, reduced hospital stays, and optimized costs for health resource allocation [5-7]. Various factors are associated with optimized OT efficiencies including enhanced timelines, staff collaboration and motivation, improved job satisfaction, and process mapping [5,8].
Previous studies have been done on various factors affecting TAT in divergent healthcare settings. A study done in Karachi, identified personnel, equipment factors, and scheduling of cases to be associated with increased TAT [1]. A study on reasons for delay in turnover time in OT showed that 47% were due to healthcare system issues such as management and planning [9]. Other studies have identified delays in starting the case, equipment, and infrastructural factors as predictors of TAT in the OT [3,10].
Personnel factors affecting TAT include staff issues such as low numbers compared to work burden, lack of collaboration [10,11] and prolonged nursing handover time causing delays [1,12].These increase TAT. Staff motivation through incentives [9,13] decreases TAT. Capacity building through training improves theatre efficiency and its output [12,14].
Surgical factors shown to increase TAT include complexity of surgeries leading to mental fatigue [15,16], ASA physical status [17], poor patient preparation [18,19] and unavailability of blood during surgery [20-22].
Infrastructural factors affecting TAT include accessibility of theatres from surgical wards [23], lack of lifts to ferry patients [23], availability of surgical ICU and PACU [24,25], availability of water, electricity and oxygen [26].
Despite the knowledge of the preexisting predictors of TAT, there is limited research in Kenya.This study examined the association between factors identified in other studies and the TAT in Kenyatta national Hospital (KNH). KNH is a tertiary, teaching, and referral hospital in the East and Central African region. This study will give a Sub-Saharan Africa specific view on TAT which may improve the output of operating theatres.
This was a descriptive observational study done in September and October 2021.The sample consisted of staff affiliated to KNH, University of Nairobi (UON) and the Kenya Medical Training College (KMTC). We included all the staff working in the 12 main theatres. They included surgeons, anaesthesiologists, registered clinical officer (C.O) anaesthetist, qualified nurses, theatre service attendants (TSA), postgraduate students in surgery and anaesthesia (registrars), cleaners and porters. Only those participants who consented to participate were included in the study.
Proportionate stratified sampling was used to allocate 400 out of the 840 total staff working in the main theatres. The staff were subcategorized into 5 strata based on speciality and level of qualification. These were consultants, both surgeons and anaesthesologists (82 responded out of 173), nurses (46 responded out of 97), registrars (223 responded out of 468), C.O. anaesthetists (19 responded out of 40), and support staff including TSAs, cleaners, and porters (30 responded out of 62).
Data was collected using a questionnaire that was administered both physically (paper-based) and digitally using the KoBo Toolbox. A pilot study was carried out at the maternity theatres beforehand to assess the feasibility of the data collection tool. Data collected contained staff demographics and variables on personnel, surgical, equipment, consumables, and infrastructural factors. These variables were expressed in a 5 level Likert scale (1. Strongly disagree; 2. Disagree; 3. Neither agree nor disagree; 4. Agree; 5. Strongly agree). The response variable was TAT, representing the existence of delays between surgeries at KNH main theatres. The predictor variables were the variables corresponding to personnel, surgical, equipment, consumables, and infrastructural factors.
The study proposal was reviewed and approved by KNH-UON ethics research committee (P415/05/2021).
Stata 15.1 (Stata Corporation, College Station, TX) was used for data analysis. The significance level was α = 0.05. Univariate descriptive methods like frequencies and proportions was used to describe the study participants. The associations between TAT estimates and variables on different factors were initially assessed using chi-square (χ2). The multinomial logistic regression model was used to identify each factor's influence and nature of association with TAT. The coefficients (β), standard errors (SE), 95% confidence intervals (CI) and the p-values were used to explain the associations between various factors and TAT.
Of the 400 participants in the study, 57.75% were male and 42.25% were female. Majority were in the 30-39 age group while over 50 age group was the least represented. The registrar's strata were the most represented. For institutional affiliation, majority of the staff were from UON. In terms of the work experience, 89.00% had worked for more than one year (Table 1).
Table 1: Demographic characteristics. View Table 1
Majority of the staff, 27.00% agreed with the statement, while 20.75% strongly agreed that there are many delays between surgeries at KNH main theatres (Figure 1).
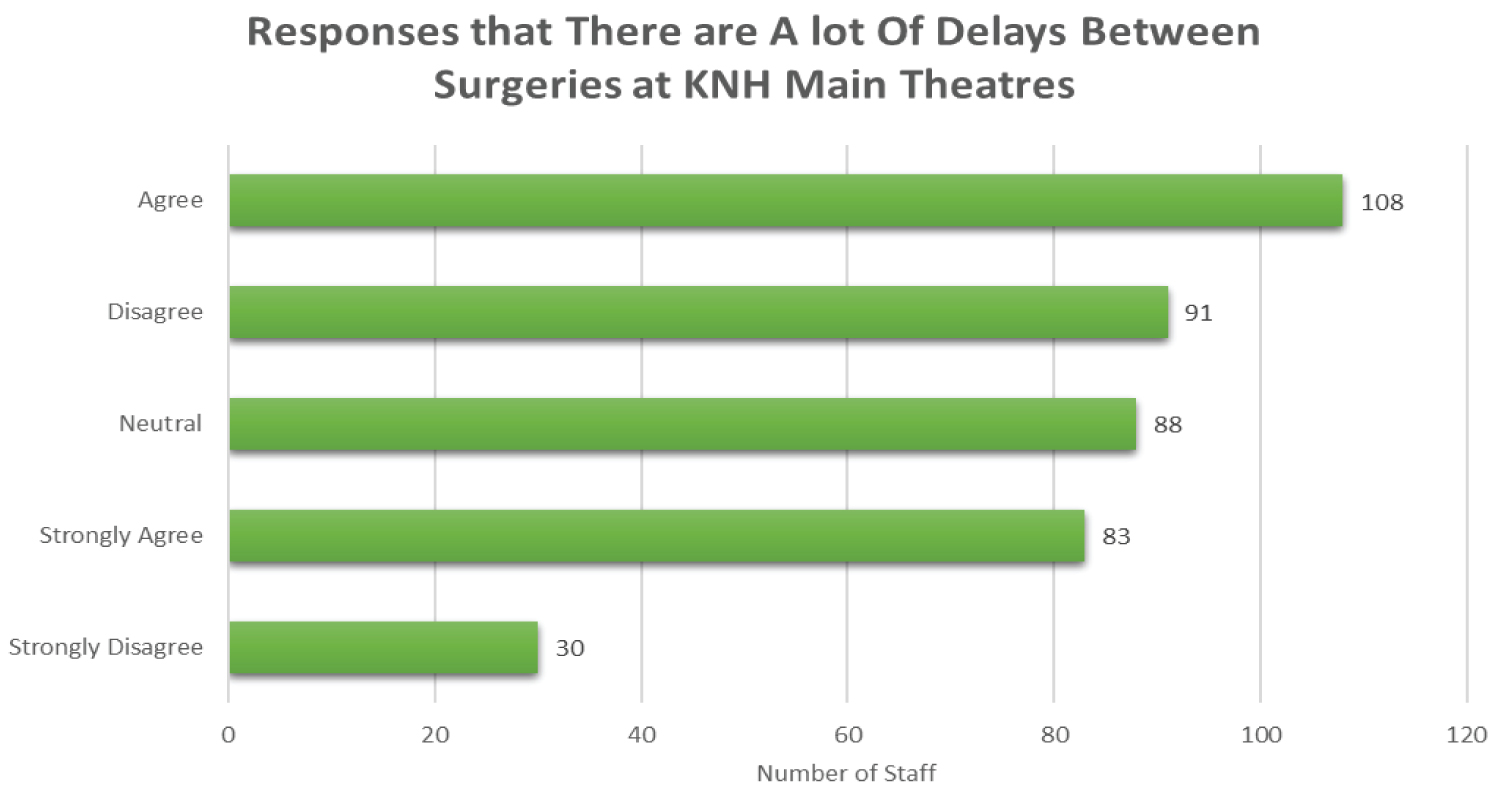 Figure 1: Perception towards delay at KNH.
View Figure 1
Figure 1: Perception towards delay at KNH.
View Figure 1
Table 2 represents the perception of the staff towards different factors believed to affect TAT. The general expression of the staff indicating whether they think that there exist major delays between surgeries was the major response variable. The personnel, surgical, equipment, consumables, and infrastructural factors were the explanatory variables.
Table 2: Bivariate and Multinomial Regression Analysis Results. View Table 2
All personnel, surgical, equipment and consumable factors were significantly associated with TAT (p < 0.05). All the infrastructural factors were significantly associated with TAT except water supply (Table 2).
Personnel factors: Prolonged nursing handover time during shift change, major staff shortage and lack of support from the theatre managers increased TAT. Theatre staff being insufficiently qualified for their jobs, staff training needs not being adequately met, lack of staff motivation, staff not being highly overworked, not being late to the workplace, not absconding from work and good teamwork amongst staff, had no significant impact on TAT, p > 0.05 (Table 2).
Surgical factors: Adequacy in numbers of surgical sets and patient being prepared well for surgery preoperatively had no significant association with the delays between surgeries (p > 0.05). Theatre preparation for emergency surgeries compared to elective surgeries increased delays between surgeries (p < 0.05). There was increased theatre preparation time in emergency cases compared to elective cases. The efficiency and adequacy of response of blood transfusion units to the theatre's blood transfusion requests also had significant influence on TAT (< 0.05).
Equipment and consumables factors: Availability of enough anaesthesia machines and anaesthetic drugs; and adequacy in number of stretchers and wheelchairs decreased TAT. Inadequate supply of drapes and gowns increased TAT. The inadequacy and unreliability of laboratory support for patients did not have a significant influence on the delays between surgeries (p > 0.05).
Infrastructural factors: Water supply, ICU space for deserving surgical patients and sufficient PACU space for patients post operatively had no significant influence in TAT (> 0.05). Reliability of electricity supply decreased TAT (p < 0.05). Lack of adequacy and reliability of oxygen supply and lack of ease of accessibility of the main theatres from the surgical wards and ICU increased TAT (p < 0.05).
Participants were asked to give opinions on factors not listed in the variables that they thought influenced TAT in KNH main theatres. It was identified that few patient porters caused delays in moving patients to and from theatres. Consultant surgeons' delay in joining junior surgeons/registrars during complicated surgeries caused delays. Inadequate number of lifts with habitual malfunctions were also associated with delays.
TAT is a quality marker for theatre efficiency. The aspects that include personnel, surgical, equipment, consumable and infrastructural factors are associated with TAT in KNH main theatres. This is similar to previous studies on TAT [1,9,10].
Inadequate staffing increased TAT. This mirrors a study conducted in Malawi which indicated that there were few staff and too many patients leading to 40% wanting to resign [27]. There were few patient porters causing delays in movement to and from theatre; similarly observed by Haldar, et al. [23]. Studies have shown that staff collaboration and teamwork between staff and management were associated with decreased delays in theatres [27,28]. Similarly, D Nina, et al. emphasized the importance of feedback and positive reinforcement to the staff by hospital administration as a way of reducing TAT [13]. In this study, lack of supportive theatre managers caused delays between surgeries. We cannot conclude that staff's performance was affected by lack of motivation. This contrast other studies on staff motivation and performance in theatres [9,10].
Prolonged nursing handover time during shift change increased TAT. Studies have shown that delay caused by nurses is mainly due to miscommunication and incomplete handover.
An audit done in India to assess the causes of delay in theatres showed myriad factors associated with delays between surgeries [29]. Some of these factors did not have influence in TAT in our study as they were inconclusive. These included lack of staff lateness to work, lack of sufficient job qualification or absconding work.
Staff capacity building through training had no influence on TAT in KNH. This is dissimilar to study by Weller, et al. where staff training improved performance and theatre output [14]. This could be due to the fact that KNH is a training center therefore the staff in theatres are continuously trained.
The urgency of the surgery had a significant impact on TAT. Theatre preparation for emergency surgeries compared to elective surgery was associated with increased delays. A similar observation was made on a study conducted by Essen, et al. [30]. This could be due to the OT reorganization needed to accommodate the age and ASA status of the patient and the type of surgery [17]. Inefficiency of blood transfusion units during surgeries increased TAT. Similarly, Kajja, et al. indicated increased delays in surgery where higher amount of blood units was needed peri-operatively [20].
Lack of adequate and reliable supply of drapes and gowns increased TAT at KNH main theatres. Drapes and gowns are essential in theatres to ensure sterility during surgical procedures [31]. Kieser, et al. showed that irregular supply of drapes and gowns can cause delays in theatres [31]. Adequate numbers of anaesthesia machines and reliable supply of anaesthetic drugs reduced TAT. In contrast, 29% of the cases were postponed in Tanzania due to faulty anaesthesia machines [32] and Charana, et al. found inadequate drug supply in selected surgical camps in Kenya affecting quality of anaesthesia [33].
In this study, we found that there is adequate number of stretchers and wheelchairs which is associated with reduced delays pre- and post-operatively [34].
Oxygen supply in KNH main theatre was inadequate and unreliable increasing TAT. Similarly, Linden, et al., showed that insufficient oxygen, affected safe surgical services in Uganda [20]. However, the surge in Covid-19 pandemic in April 2021, leading to shortage of oxygen supply in Kenya, hence KNH main theatres, could have led to this finding. Adequate supply of electricity in the main theatres was associated with decreased TAT between surgeries. In Uganda, insufficient supply of electricity affected surgical service delivery [29]. Lack of ease of accessibility of main theatres from the surgical wards and ICU was significantly associated with delays. This is similar to a study by Haldar, et al. [23].
There existed no significant association between water supply, availability of ICU and PACU space, and the theatre TAT in KNH. This contrasts previous studies [25,26]. This could indicate that KNH main theatre is well equipped and adequately planned to take care of patients post-operatively.
The outcomes of this study indicated multiple factors affecting TAT at KNH. The nature of the associations and influence, both positive and negative were estimated. Personnel, surgical, equipment, consumable, and infrastructural factors each had a unique outcome. This study informs the myriad drivers, facilitators and barriers towards effective main theatres operation. There is need to utilize the research output of this study to influence the healthcare system to improve the KNH theatre operation mechanisms and the overall surgical patients service delivery.
The following were the major recommendations identified in this study to influence the operation of main theatres;
1. The number of staff in the theatres should be increased to reduce workload and improve service delivery.
2. Use of feedback and positive reinforcement by theatre managers to the theatre staff.
3. Collaboration and teamwork between blood transfusion unit and KNH main theatre to ensure timely blood transfusion requests.
4. Ensuring adequate and reliable oxygen supply in the theatres.
5. Ensuring adequate and reliable supply of drapes and gowns.
6. Investment in infrastructure in order to reduce the effects of distance between main theatre, surgical wards and ICU by building theatres next to these units or on each surgical floor.
7. Availing enough, functional lifts, and general infrastructural improvement.
8. In-depth analysis of the everyday running of theatre operations will enhance the identification of further factors and gaps that contribute to increased TAT.
The study was conducted on a large sample size across all cadres working in KNH theatre.
It was a unicentre analysis. Factors affecting TAT in day case surgeries and emergencies in KNH were not truly reflected as they were excluded from the study. COVID-19 pandemic may have contributed to findings in some factors like oxygen supply leading to bias.
No conflict of interest from the authors.
Belinda Adda Namisi: manuscript writing, design supervision; Vernon Mark Gacii: Supervision, review; Caroline H. Karugu: Data analysis.