Central venous catheter placement is associated with known risks and complications [1]. Its proper placement is necessary for long-term use. However, their mispositioning is not uncommon. But mispositioning of the catheter tip into the contralateral subclavian vein is extremely rare. After obtaining the informed written consent, we present an image of a 48-year-old female who presented to emergency with traumatic right above elbow amputation and blunt chest trauma. Because of difficult peripheral intravenous access, a central venous access was placed in the right subclavian vein under ultrasound guidance. The procedure was uneventful but the chest X-ray revealed the tip of the catheter to be present in the opposite subclavian vein (Figure 1). The catheter was removed, and the right internal jugular vein was correctly cannulated (Figure 2). The likely cause for this misplacement may be that the guidewire in our case must have passed through the right subclavian vein, the right brachiocephalic vein, the left brachiocephalic vein, and finally the left subclavian vein.
 Figure 1: Chest X-ray showing central venous catheter tip in the contralateral (left) subclavian vein.
View Figure 1
Figure 1: Chest X-ray showing central venous catheter tip in the contralateral (left) subclavian vein.
View Figure 1
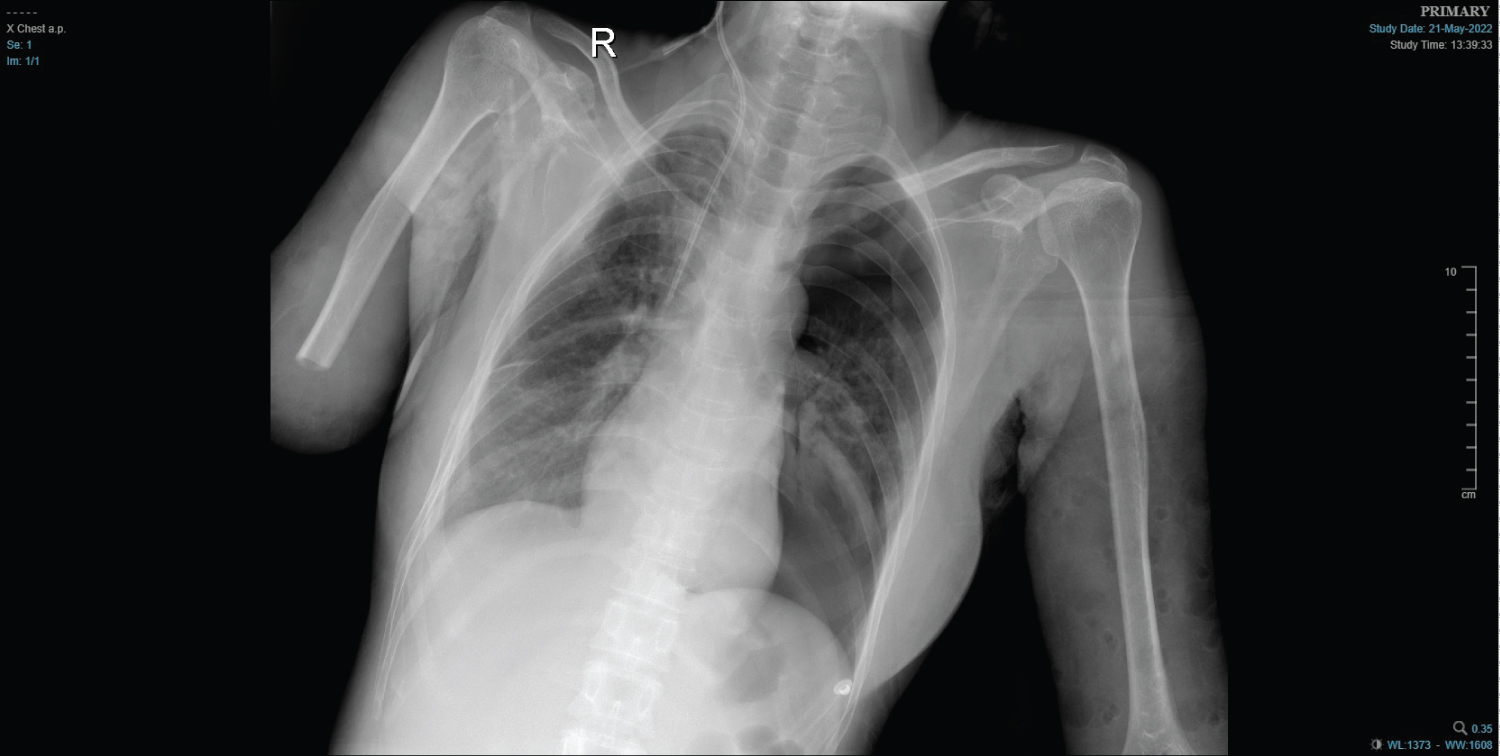 Figure 2: Chest X-ray showing correct placement of right internal jugular vein venous catheter.
View Figure 2
Figure 2: Chest X-ray showing correct placement of right internal jugular vein venous catheter.
View Figure 2
The subclavian vein catheter is most commonly misplaced in the right internal jugular vein [2] rather than the opposite subclavian vein. The causes may be a more horizontal orientation of the right and left brachiocephalic trunks, a longer insertion path (> 18 cm), and a changed orientation of the J-tip of the guidewire during the insertion [3].
Despite following recommended measures like lowering the shoulder, putting pressure over the supraclavicular fossa, using ultrasound for vein and guidewire locations, and observing for atrial ectopic, there is still a chance for catheter tip malposition. But because of several anatomic advantage like larger diameter, relatively constant position, absent valves along with reduced risk of infection and thrombosis [4], it should not deter the clinician from using it as one of the sites for central venous access.
None.