Transanal endoscopic microsurgery (TEMS) is minimally invasive, safe and highly effective treatment modality for resecting small rectal lesion like adenomas, early stage carcinoma and strictures. We describe an unusual case of massive subcutaneous emphysema and hypercarbia secondary to TEMS leading to ventilatory difficulty and post-operative mechanical ventilation. Extra peritoneal insufflation of CO2 at high pressure, for prolonged duration and extent of tissue dissection are some of the predisposing factor leading to rare but life threatening respiratory complications. Intra operative management should consist of changing from nitrous oxide if we are using it to air and oxygen, expediting the surgery, reducing the insufflation pressure and careful extubation while postoperatively conservative management should be considered with close monitoring of the patient for timely intervention if condition of the patient deteriorates.
TEMS: Transanal Endoscopic Microsurgery; ASA: American Society of Anesthesiologist; PEEP: Positive End Expiratory Pressure; FiO2: Fraction of Inspired Oxygen; ETCO2-: End Tidal Carbondiaoxide
Carcinoma of rectum is one of the most common cancer of gastrointestinal tract in adults leading to morbidity and mortality worldwide. Highly invasive form of rectal cancer is preceded by development of adenomas. Among adenomas tubullovillous and villous adenomas have high incidence of transformation to invasive colorectal cancer [1].
Transanal endoscopic microsurgery (TEM) is a minimally technique which is developed for the resection of benign rectal lesions. Transanal endoscopic microsurgery was introduced in 1983. It has emerged as one of the safer, highly effective and minimally invasive method of resecting rectal lesions like adenoma, early stage carcinoma and stricture [2]. TEM has the advantage of good visualization, better exposure and allowing use of both hands during procedure resulting in more precise excision of lesions as compared to previous used technique. One of the major benefit of using TEM is the significantly lower morbidity and mortality as compared to traditional technique of treating rectal lesions like abdominoperineal resection and low anterior resection [3]. Quality of life after TEM is better because functional integrity of anal sphincter is preserved and damage to autonomic nerves is averted. Intra operative and postoperative complication associated with TEM are rare and include bleeding, perforation, incontinence and rectal stricture [4].
Our case report is unique because it shows one of the potentially life threatening but rare complication of TEMS that is massive intraperitoneal, subcutaneous emphysema and hypercarbia necessitating post-operative ventilatory support and monitoring in intensive care unit.
A 77 year old man presented with three episodes of rectal bleeding. Colonoscopy revealed several sessile polyp throughout the length of colon. There was also presence of a one large polyp measuring 4 cm in diameter located at approximately 10 cm from the anal verge. Pathology report showed tubular adenoma with high grade dysplasia but CT scan of abdomen, pelvic MRI and rectal ultrasonography did not show any sign of invasive growth, pathologic lymph nodes or systemic spread. Since the lesion was small and patient was not willing to consent to a more invasive procedure such as abdominal perineal resection, so TEMS was planned. The patient was ASA physical status class 2 with history of hypertension well controlled with metoprolol and past history of head injury for which he was on phenytoin for last 10 years. His pulmonary function was within normal limit with no history of smoking and chest disease.
After pre oxygenation, General anesthesia was induced with fentanyl, Propofol and atracurium and endotracheal tube was placed. Volume controlled ventilation was used during the surgery with peak airway pressures was between 15 to 17 cm of H2O without PEEP. Anesthesia was maintained using oxygen, nitrous oxide and desflurane. Morphine, paracetamol and ketorolac was given for intraoperative analgesia.
Patient was placed in lithotomy position with head tilted slightly downwards. Carbon dioxide was insufflated at rate of 6L/min while maintaining intraluminal pressure below 12 mm of Hg.
Table 1: Prevention strategies and differential diagnoses for subcutaneous emphysema. View Table 1
Initial course of the surgery was uneventful but after 2 hours there was sudden rise in end tidal CO2 which coincided with rise in peak airway pressure from 17 to 28 cm of H2O and fall in oxygen saturation from 99% to 94% despite no change in patient position or tidal volume. On auscultation, chest sounds was within normal limit. Patient's core body temperature was normal and hemodynamics was stable. Minute ventilation was increased, FiO2 was increased from 30% before incident to 100% and Nitrous oxide was replaced with air as there was high suspicion of undetected pneumothorax. But the issue did not resolved with increased minute ventilation and atracurium was given with the hope that adequate muscle relaxation might improve ventilation and result in reduction of EtCO2 and peak airway pressure which proved futile. Physical examination revealed massive subcutaneous emphysema involving the neck, anterior abdominal wall, and scrotum extending up to both thighs. No signs of peritoneal perforation was noted during the procedure and bladder drainage was clear. It was decided to shift the patient to intensive care unit as even after completion of procedure, patient showed saturation of 95%, ETCO2 of 48 mm of Hg and peak airway pressure of 25 cm of water.
Neuromuscular paralysis was reversed with neostigmine and glycopyrrolate but patient was not extubated and shifted to intensive care unit. Immediate chest X ray was done which confirmed the presence of subcutaneous emphysema but there was no sign of pneumothorax (Figure 1). Arterial blood gas analysis at FiO2 of 100% and volume controlled ventilation showed respiratory acidosis.
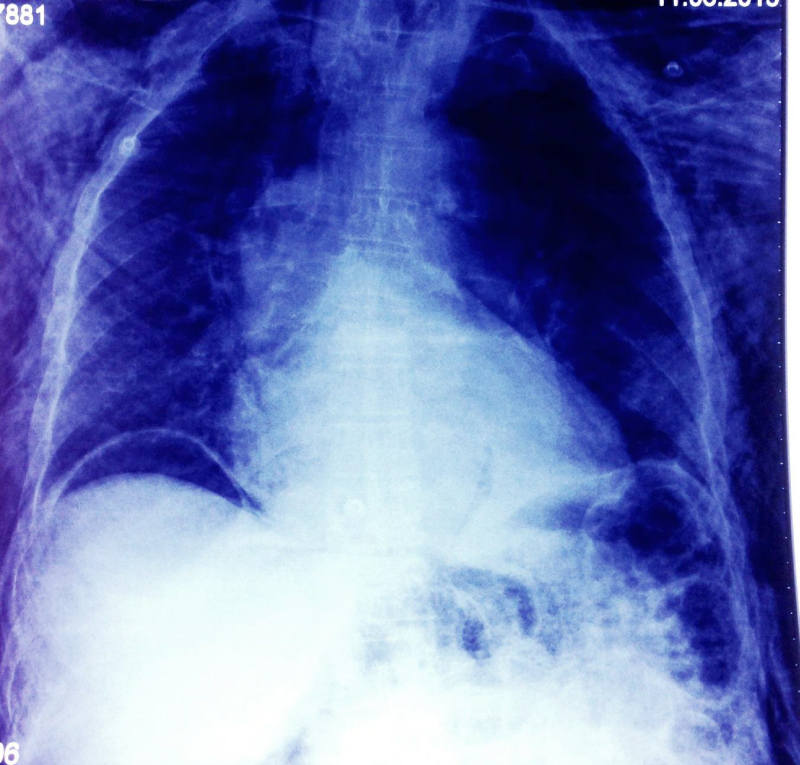 Figure 1: Showing free gas under the diaphragm. View Figure 1
Figure 1: Showing free gas under the diaphragm. View Figure 1
Day 1: Mechanical ventilation using pressure support ventilation was used. Repeat chest x-ray showed free gas under the diaphragm but there was no sign of guarding or rigidity. Subcutaneous emphysema was still present (Figure 2).
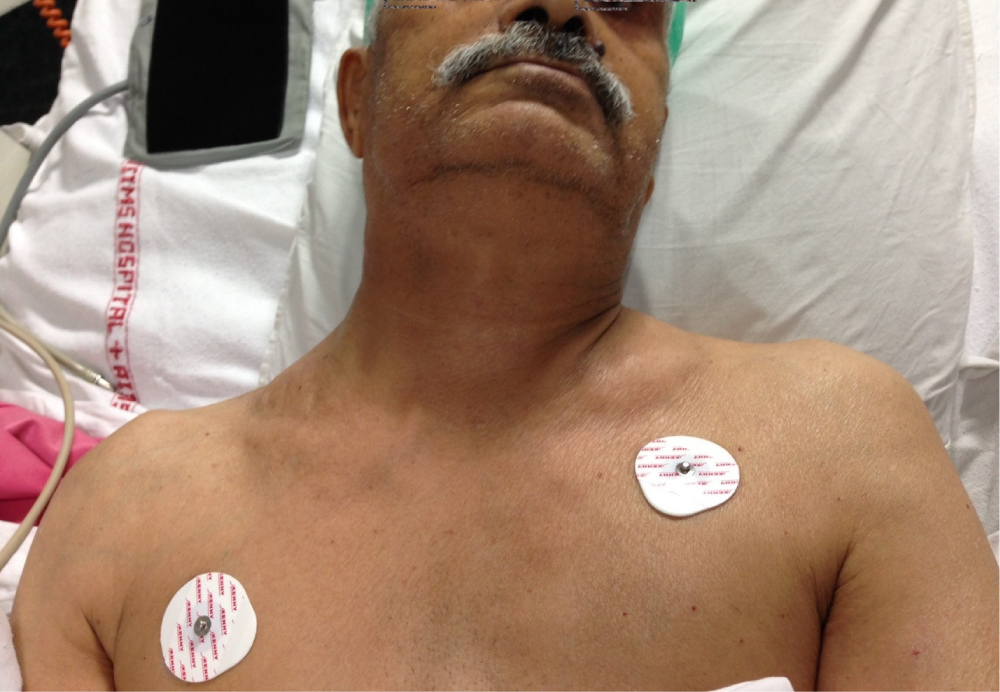 Figure 2: Showing subcutaneous emphysema.
Figure 2: Showing subcutaneous emphysema.
RA: Right Atrium; RV: Right Ventricle; LA: Left Atrium; LV: Left Ventricle View Figure 2
Day 2: Patient was extubated in the evening and subcutaneous emphysema started resolving.
Day 3: Subcutaneous emphysema resolved up to 90%.
Day 4 and Day 5: Patient was comfortable, taking orally, passed stool and flatus.
Day 6: The patient was transferred to ward care.
Day 7: Patient was discharged and asked to follow up as outpatient in surgical outpatient department.
Chest x ray and arterial blood gas analysis was done twice daily so that any deterioration in the clinical condition of the patient can be diagnosed promptly.
The subcutaneous emphysema resolved on day 5 and patient was discharged on day 7 with stool softener, antibiotics and proton pump inhibitor.
Patient was asked to continue taking phenytoin and metoprolol as advised before.
Routine investigation on subsequent visit showed no sign of residual tumor and now patient is on regular follow up.
This case describes the effect of intraoperative hypercarbia and subcutaneous emphysema during TEMS leading to delayed extubation and extended stay in the ICU. It is a well-known fact that we should increase minute ventilation in order to maintain normocapnia during laparoscopic surgery but no such recommendation is available for TEM surgery. It has been reported that intraperitoneal insufflation of CO2 leads to subcutaneous emphysema in 3% of the cases during laparoscopy [5].
TEMS though reduces morbidity and mortality associated with APR and permanent stoma but still it is associated with various complication. Some are due to patient positioning while others are due to prolonged surgery. Some rare complications are also associated with it like development of massive subcutaneous emphysema and hypercapnia leading to ventilator failure.
However, the incidence of subcutaneous emphysema with TEM is extremely low [6]. Mechanism are raised insufflation pressure, duration of insufflation, extra peritoneal approach and extent of tissue dissection. The development of subcutaneous emphysema is likely due to tracking of gas under tension along the surgically opened tissue planes. A gas flow of at least 6 liters/minute has been recommended to maintain intra rectal pressure of 12-15 mm of Hg. We recommend the clinicians to monitor insufflation flow and intrarectal pressure continuously. The lithotomy position along with spread of carbon dioxide to loin, groin, anterior abdominal wall and thigh hindered detection of surgical emphysema in our patient. We suggest detailed examination of patients at unusual site for surgical emphysema if very high level of EtCO2 or PaCO2 are noted during TEMS.
Blair showed that insufflation of carbon dioxide into subcutaneous fat of anterior abdominal wall of anesthetized pigs having fixed minute ventilation resulted in increased arterial carbon dioxide concentration and fall in blood pH for long duration [7]. He suggested that patient with similar condition should undergo repeated testing of arterial carbon dioxide and remain in the recovery room for longer time. Our case demonstrate the life threatening complication post TEMS by a mechanism similar to Blair's model.
The potential differential diagnoses can be Spontaneous pneumothorax, acute respiratory failure, pulmonary embolus and intraperitoneal perforation. Various methods of prevention and differential diagnoses are mentioned in Table 1.
"Kerr and Mills" in 2001 reported a case of intraoperative and postoperative hypercapnia leading to delayed respiratory failure secondary to TEMS with moderate degree of subcutaneous emphysema. They told that a patient with arterial hypercapnia and subcutaneous emphysema should be observed for prolonged period with regular blood gas analysis to allow timely intervention [8].
Franken, et al. in 2012 described 2 cases of free intra-abdominal air without perforation after TEMS. In both cases diagnostic laparoscopy showed no peritoneal breech and both patient were managed conservatively. However they suggested that close monitoring of patient is necessary, so that conservative management can be replaced by surgery if the patient's condition deteriorates [9].
Aninda Chandra, et al. in 2014 reported the first case of massive subcutaneous emphysema with hypercarbia leading to ventilator difficulty. Their patient had complete resolution of emphysema at 24 hour and was discharged on day two. They followed conservative treatment without any surgical intervention post complication [10].
With increasing popularity of TEMS for rectal lesion, we expect these kind of complication to occur more frequently. After ruling out rectal perforation by abdominal CT-scan, first conservative management should be done consisting of advanced hemodynamic monitoring and regular follow-up of symptoms & signs of intestinal perforation and peritonitis so that conservative treatment can be replaced by surgery once the patient deteriorates.
Dr. Kaushal has meticulously followed this patient in the ICU and provided us the follow-up detail.