The objective of this study is to evaluate the analgesic efficacy and patient recovery characteristics when utilizing opioid- free anesthesia (OFA) as part of a multimodal enhanced recovery after surgery pathway (ERAS) for bariatric surgery.
Retrospective cohort study. Data was collected from medical records from June 2018 to September 2019 for consecutive patients aged 18 and older undergoing elective laparoscopic sleeve gastrectomy for obesity. A standardized ERAS pathway for bariatric surgery was utilized in all study patients. For anesthetic maintenance, the OFA group (n = 46) received propofol combined with dexmedetomidine, lidocaine, and/or ketamine by intravenous infusion. In the opioid-based anesthesia (OBA) group (n = 160), a volatile agent or propofol infusion and opioid were used. Analysis of outcome variables was conducted using STATA software, version 16.1. Time to first postoperative opioid (min), amount of opioid administered postoperatively, pain intensity scores, time to PACU discharge readiness, hospital length of stay, and incidence of postoperative nausea and vomiting (PONV).
OFA was not associated with an increased rate of opioid use (hazard ratio [HR] 1.23, 95% CI (0.85-1.79), p = 0.26) in comparison to the OBA group. There was no difference in median time to first postoperative opioid rescue between the two groups (p = 0.57). The incidence of PONV in the first 6 postoperative hours was similar in both groups (p = 0.39), as were time to discharge readiness (p = 0.11) and hospital length of stay (LOS) > 1 day (p = 0.77). There was no statistical difference in opioid consumption in the first 6 hours (p = 0.82) and 6 to 24 hours (p = 0.79) postoperatively between the two groups.
In this study, patients who received OFA during bariatric surgery had similar recovery characteristics when compared to patients who received OBA.
Opioid-free anesthesia, Enhanced recovery after surgery, Anesthetic adjuncts, Sleeve gastrectomy, Bariatric surgery
OFA: Opioid Free Anesthesia; ERAS: Enhanced Recovery after Surgery Pathway; OBA: Opioid Based Anesthesia; PONV: Postoperative Nausea and Vomiting; LOS: Length of Stay; OSA: Obstructive Sleep Apnea; HTN: Hypertension; DT2: Diabetes Mellitus Type 2; GERD: Gastroesophageal Reflux Disease; OME: Oral Morphine Equivalents; NRS: Pain Intensity Scores
Obesity is a serious global public health problem. The prevalence of obesity in adults in the United States (US) is almost 40% [1]. Associated comorbid conditions such as obstructive sleep apnea (OSA), hypertension (HTN), and diabetes mellitus type 2 (DT2) significantly decrease quality of life and increase mortality in this population [2,3]. The prevalence of OSA in obese adults is nearly double that in normal weight adults and is present in 71% of patients being evaluated for weight loss procedures [4,5]. Bariatric surgery is the most effective treatment for sustained weight loss [6]. An estimated 228,000 bariatric procedures were performed in the US in 2017, and this number is expected to increase [7]. Obesity is a known risk factor for opioid-induced respiratory depression, and bariatric surgery patients are at increased risk for thromboembolism [8,9]. Therefore, utilizing anesthetic techniques that promote rapid emergence, minimal postoperative sedation and early ambulation are desirable.
Opioids are widely used to supplement general anesthesia for bariatric surgery and are commonly used for the treatment of acute post-surgical pain [10]. In addition to respiratory depression, opioids exacerbate OSA, increasing the risk of critical respiratory events (CREs) during recovery from surgery [11]. Their use may also increase PONV and its severity, requiring the administration of rescue medications that can cause significant sedation and delay early mobilization [12,13]. Paradoxically, opioid use may also lead to opioid-induced hyperalgesia, which can influence postoperative pain, opioid dose escalation and associated complications [14].
Utilization of OFA is a growing trend to counter the risks of opioid-related adverse drug events. Opioid free techniques typically employ a combination of non-opioid adjuncts to provide sedation, analgesia, and sympatholysis [15,16].
A review of evidence to date in bariatric surgery reveals that while opioid sparing techniques are effective in reducing pain scores, postoperative opioid consumption and PONV, the impact of OFA on these and other important outcome measures in bariatric patients is less clear [15,17-19]. Although OFA is considered a viable alternative to opioid-based methods, additional evidence on clinically meaningful benefits is needed.
The objective of this study is to evaluate OFA as part of a multimodal ERAS pathway for bariatric surgery with respect to analgesic efficacy and patient recovery characteristics. We hypothesize that the use of OFA will lead to reduced postoperative opioid use in the first 6 and 24 hours, reduced incidence of PONV and an earlier achievement of postoperative recovery milestones.
Following Northwell Health Institutional Review Board approval, a retrospective cohort study was conducted with a full waiver of informed consent. Data was collected from medical records from June 2018 to September 2019 for consecutive patients aged 18 and older undergoing elective laparoscopic sleeve gastrectomy. All operative procedures included in the study were performed by two surgeons. Patients converted to open procedures, undergoing gastric band placement or removal, Roux-en-Y gastric bypass or patients with surgical complications necessitating reoperation were excluded. The decision to use OFA or opioid-based anesthesia (OBA) was made according to the preference and expertise of the anesthesiologist. All patients were managed within the guidelines of our departmental ERAS pathway for bariatric surgery.
Standard ASA monitors were utilized in the operating room, including Bispectral Index® (BIS® Aspect Medical Systems, Newton, MA). After adequate preoxygenation, all patients were induced with propofol (1.5-2 mg/kg), lidocaine (1.5 mg/kg), and succinylcholine (1-1.5 mg/kg) or rocuronium (0.5-1 mg/kg) to facilitate endotracheal intubation. Fentanyl (50-100 μg) bolus doses were added in patients receiving OBA. Port sites were infiltrated with liposomal bupivacaine (Exparel®) by the surgeon in both groups. In patients receiving OBA, general anesthesia was maintained with sevoflurane in oxygen and air or an infusion of propofol (90-200 μg kg-1 min-1). Intermittent fentanyl boluses or remifentanil by continuous infusion (0.05-0.3 μg kg-1 min-1) were administered at the anesthesiologist's discretion. Patients in the OFA group received an infusion of propofol (90-200 μg kg-1 min-1) and one or more of the following adjunct infusions: Dexmedetomidine (0.2-0.6 μg kg-1 h-1), ketamine (5 μg kg-1 min-1), and lidocaine (0.5-2 mg kg-1 h-1). When ketamine was used, a 0.5 mg/kg bolus was administered after endotracheal intubation. Additional ketamine boluses were given at the anesthesiologist's discretion. In both groups, muscle relaxation was maintained with rocuronium and anesthetic agents were titrated to maintain the BIS® value between 40-60. Persistent hypertension with a BIS value < 40 was treated with esmolol or labetolol. Patients were extubated in the operating room after reversal with sugammadex (2-4 mg/kg) or neostigmine (5 mg maximum dose) and glycopyrrolate (0.2-0.8 mg). All patients received IV acetaminophen (1000 mg) before incision and dexamethasone (4-8 mg), ondansetron (4 mg), ketorolac (30 mg) intraoperatively. Standard postoperative orders included IV ketorolac (30 mg), acetaminophen (1000 mg) and ondansetron (4 mg) every 6 hours until hospital discharge. Fentanyl, hydromorphone, and oxycodone were administered for breakthrough pain. Pain scores were recorded using a 10-point numeric rating scale (NRS). Breakthrough PONV was treated with IV haloperidol (1 mg) and diphenhydramine (25 mg).
The primary exposure variable was defined as anesthesia type with OFA defined as the complete elimination of intraoperative opioid administration by any route during intraoperative anesthesia care.
The primary outcome was time (in minutes) to administration of first postoperative opioid rescue dose. Secondary outcomes included the amount of opioid administered postoperatively at timed intervals (oral morphine equivalent dosage in mg), pain intensity scores (from 0-10 verbal NRS scales) at timed intervals, time to PACU discharge readiness (defined as time to Aldrete 10 in minutes), hospital length of stay (LOS; in days) and incidence of PONV (defined as administration of any antiemetic supplemental to usual care ondansetron administration every 6 hours for breakthrough nausea or vomiting). Additional data collected from electronic medical records included patient age, sex, race, ethnicity, body mass index (BMI), American Society of Anesthesiologists Physical Status (ASA PS) and any clinically relevant comorbidities such as gastroesophageal reflux disease (GERD), OSA, HTN, DT2 as well as a history of chronic pain, anxiety or depression.
Statistical analysis was conducted using STATA software, version 16.1 (StataCorp LLC, College Station, Texas). We conducted statistical analysis for the outcome variables: time to first postoperative opioid rescue event, postoperative opioid consumption at timed intervals converted to oral morphine equivalents (OME), time to PACU discharge readiness (minutes), LOS (days), pain intensity scores (NRS) and the incidence of PONV in the first 6 hours during postoperative recovery. Continuous data were assessed for normality graphically and using the Shapiro-Wilks normality test. Descriptive statistics such as means (95% confidence intervals; CI), medians (interquartile range; IQR) and percentages with frequencies were used to describe the outcomes. For univariate analyses conducted to compare patient characteristics and outcomes for OFA and OBA groups normally distributed, continuous variables were compared using student t test while non-parametric continuous data were analyzed using appropriate non-parametric tests. Categorical data were analyzed using the chi square or Fisher exact test. The timing of first opioid analgesic event after surgery was used as a measure of analgesic efficacy. The Kaplan-Meier method was used for time-to-event, specifically time to first rescue opioid event analysis in the first 6 postoperative hours. Median time to event in minutes with 95% CI was estimated and the Log-rank test was used to evaluate the difference in time-to-event endpoint between OFA and OBA groups. Univariate Cox proportional hazards models were fitted to evaluate the effect of OFA and patient demographic and clinical characteristic variables on the time-to-event outcomes. A multivariate Cox proportional hazard models was used to adjust for age, gender and covariates with p < 0.2 from univariate analysis. Statistical software STATA version 16.0 was used for all the analyses. A p-value < 0.05 was considered statistically significant.
From June 2018 to September 2019, 206 adult patients underwent laparoscopic sleeve gastrectomy for weight loss (Figure 1). The median age (IQR) of the study cohort was 41 (32-52) years and median BMI was 42.85 (39.60-46.50) kg/m2. One hundred and sixty seven patients (81.1%) were female and 38.1% (n = 78) were African American. Almost 23% (n = 46) of our cohort underwent surgery with OFA. Patient demographics were similar in both OFA and OBA groups (Table 1), as were BMI, ASA status (percentage of patients with ASA PS ≥ 3), prevalence of type II diabetes (DT2), GERD and surgical duration. While a trend for a higher prevalence of HTN (50.0% versus 35.0%) and OSA (69.6% versus 55.6%) was observed in patients in the OFA group, these differences were not statistically significant at the p < 0.05 significance level (Table 2).
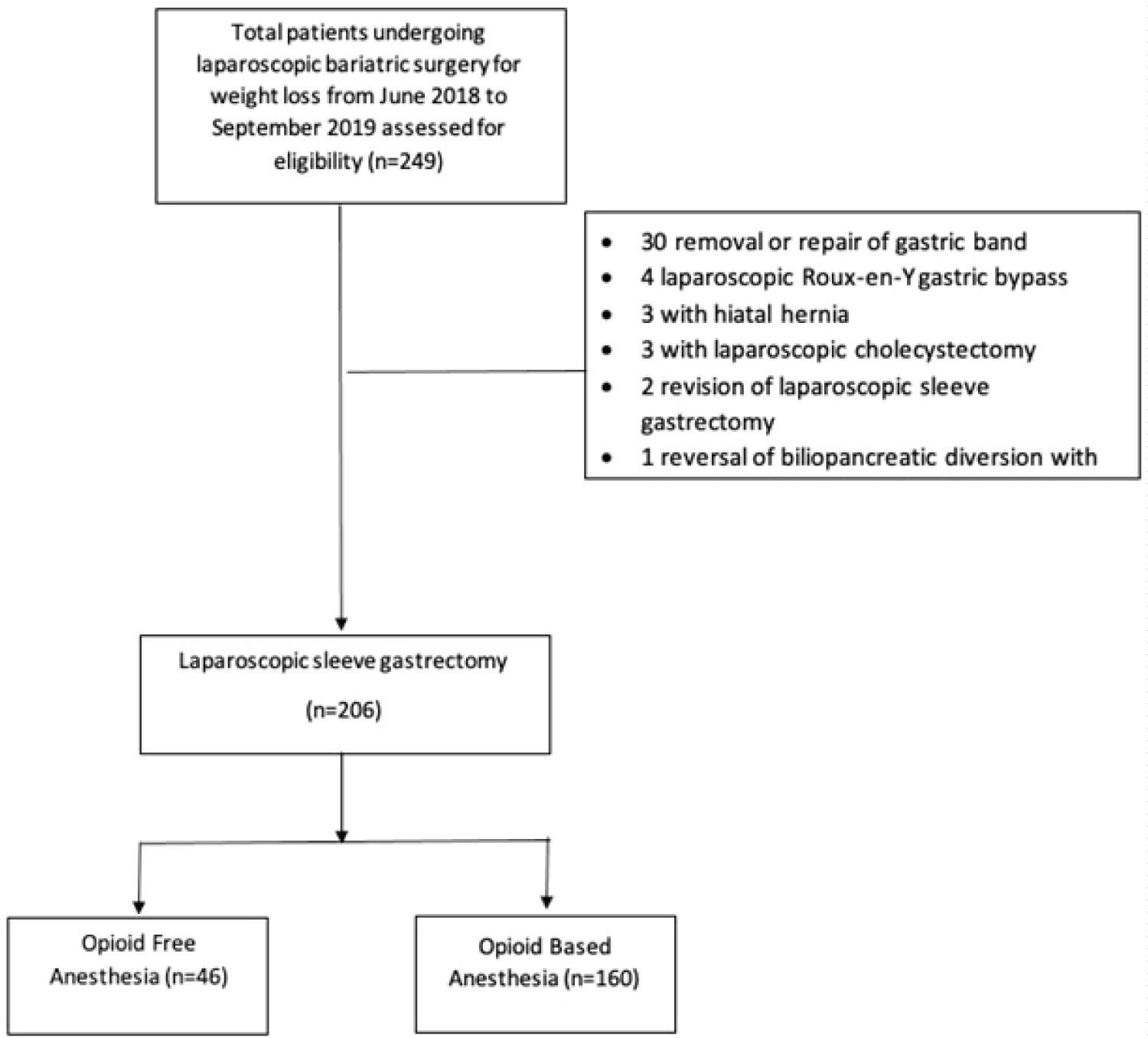 Figure 1: Flow diagram for subject selection.
View Figure 1
Figure 1: Flow diagram for subject selection.
View Figure 1
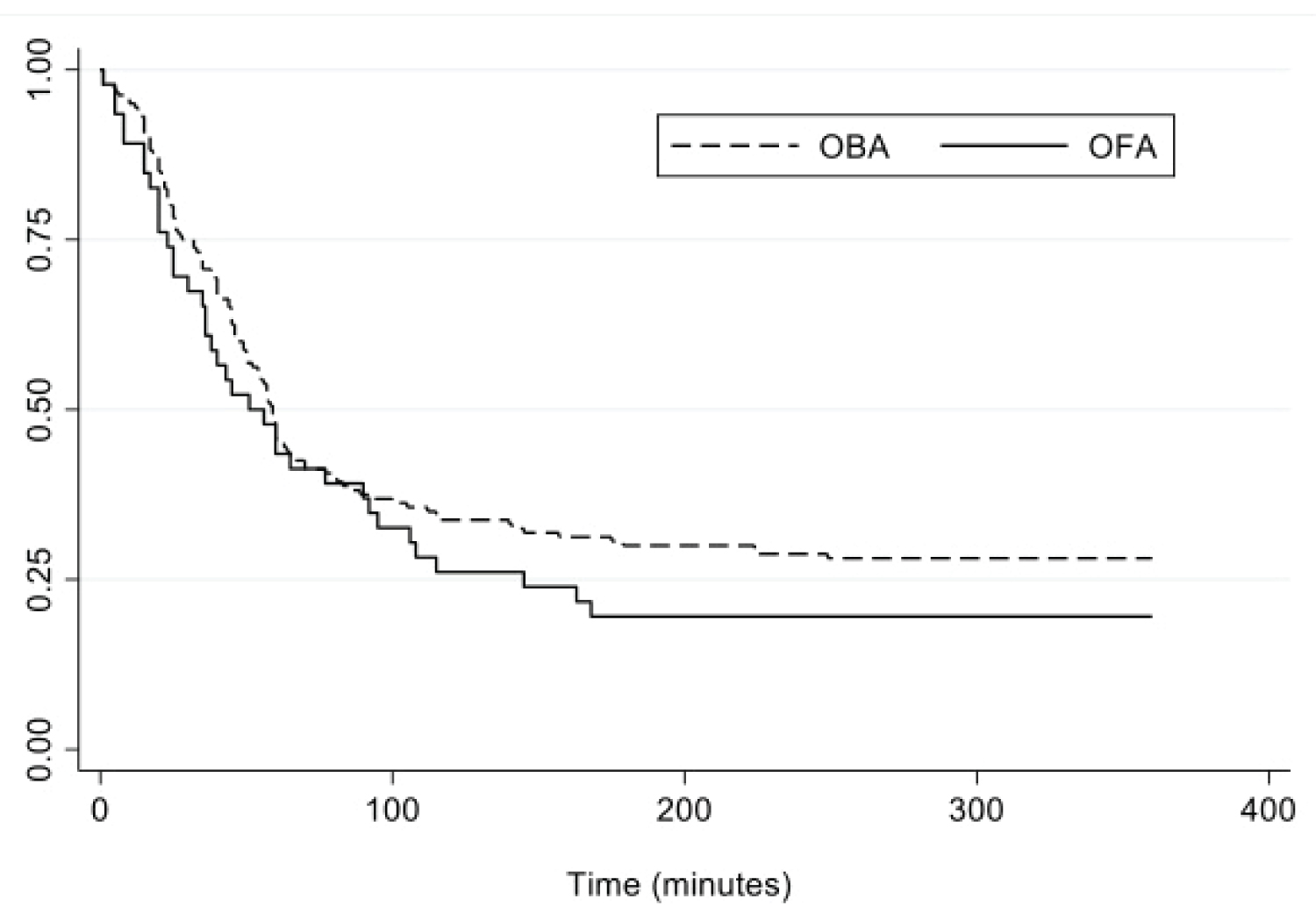 Figure 2: Kaplan-Meier survival estimates for OFA and OBA groups showing the durations of the first 6 hours of the postoperative period without rescue opioid medication.
Figure 2: Kaplan-Meier survival estimates for OFA and OBA groups showing the durations of the first 6 hours of the postoperative period without rescue opioid medication.
X-axis: Proportion of patients without opioid rescue in first 6-hour postoperative period.
View Figure 2
Table 1: Univariate analysis of patient demographics for OFA versus OBA group. View Table 1
Table 2: Univariate analysis of patient clinical characteristics for OFA versus OBA group. View Table 2
OFA and OBA groups were similar with respect to median pain intensities for the first 6 and the following 6 to 24 postoperative hour time intervals (Table 3). Similarly, the incidence of PONV in the first 6 postoperative hours was similar for both groups. No significant difference was observed between groups with respect to hospital LOS of greater than 1 night. While patients in the OFA group appeared to have increased time to PACU discharge readiness (median time in minutes [IQR]; 215 (100-275) versus 153.5 (60-260)), this result was not statistically significant at the p < 0.05 significance level (p = 0.11). OFA and OBA groups had similar opioid consumption in both the first 6 hours (median OME [IQR]; 11.25 (6.00-16.25) versus 10.0 (0-18.75), p = 0.82), and the following 6 to 24 hours (0 (0-5) versus 0 (0-5), p = 0.79). The percentage of patients that were opioid-free in the postoperative period was also similar for both groups (Table 4). There was no difference in median time to first postoperative opioid rescue between the two groups (median time in minutes [IQR]; OFA versus OBA: 39.0 (20.0-90.0) versus 46.0 (23.5-70.0), p = 0.57). Kaplan-Meier survival analyses performed using the log-rank test showed that the time to first opioid use during the first postoperative 6 hour period was similar for both groups (p = 0.25; Figure 2).
Table 3: Univariate analysis of patient recovery outcomes for OFA versus OBA group. View Table 3
Table 4: Univariate descriptive characteristics for postoperative OME (oral morphine equivalent dose) use. View Table 4
Univariate Cox proportional hazards model demonstrated OFA was not associated with an increased rate of opioid use (hazard ratio [HR] 1.23, 95% CI (0.85-1.79), p = 0.26) in comparison to the OBA group. OFA was also not significantly associated with increased rate of opioid use in a multivariate model following adjustment for age, race and ASA PS ([HR] 1.33, 95% CI (0.91-1.93), p = 0.14; (Table 5).
Table 5: Univariate association between OFA and time to first opioid rescue in postoperative period. View Table 5
In our study cohort, patients who received OFA during bariatric surgery had similar recovery characteristics, including rate and amount of opioid use, in comparison to patients who received OBA. Furthermore, recovery characteristics related to opioid use including incidence of PONV, pain intensities, time to PACU discharge readiness and length of stay were similar for both groups. Although unexpected, our outcomes could have been influenced by the absence of any standardized opioid free regime in our OFA group.
Anesthetic techniques for ERAS pathways are developed with the goal of providing optimal operating conditions with rapid postoperative recovery. Perioperative opioid administration, while an important mainstay of balanced anesthesia can be associated with adverse effects such as respiratory depression, hyperalgesia, PONV and sedation [20,21]. These opioid related effects and the current opioid epidemic have contributed to a shift towards implementation of ERAS guidelines that promote opioid-free and opioid-sparing multimodal analgesia [22,23]. Furthermore, the growing number of bariatric surgical procedures performed in the obese and morbidly obese has increased the need to explore suitable anesthetic and analgesic techniques in a population that are particularly susceptible to opioid-induced complications [24,25]. Multimodal analgesia has been shown to decrease postoperative opioid requirements and is considered an essential element in a successful ERAS pathway [26,27]. Although the ERAS Society published their guidelines for bariatric surgery in 2016, there was insufficient evidence to recommend specific intraoperative anesthetic agents or techniques at that time [26].
The opioid-free approach capitalizes on the synergistic effects of multiple analgesic adjuncts with different mechanisms of action. Typically, a combination of non-steroidal anti-inflammatory drugs, acetaminophen, lidocaine, ketamine, magnesium, gabapentinoids, and alpha-2 adrenoreceptor agonists are employed in lieu of intraoperative opioids with the ultimate goal of circumventing undesirable adverse effects that can lead to increased health care costs and decreased quality of recovery. When used as an adjunct to opioids, these agents have been shown to decrease perioperative opioid consumption and PONV [28-31].
OFA has been utilized in a variety of surgeries, attesting to its feasibility. Hontoir, et al. compared OFA using clonidine, ketamine, and lidocaine with a remifentanil anesthetic in patients undergoing breast surgery. PACU opioid consumption was similar in both groups, and higher after 24 hours in the remifentanil group. OFA patients were shown to be more sedated in the PACU, but PACU length of stay was similar for both groups [32]. Soffin, et al. compared OFA with a standard opioid technique in patients managed within an ERAS pathway for minimally invasive spine surgery. They found no statistically significant difference in opioid consumption and pain scores. PACU and hospital length of stay was similar between both groups [33]. When dexmedetomidine with lidocaine were compared to a remifentanil anesthetic for laparoscopic cholecystectomy, fentanyl requirements were reduced 2 hours after extubation, but were equivalent at 4 and 6 hours postoperatively. PACU discharge was delayed in the opioid-free group [34]. A meta-analysis of randomized trials comparing opioid-based to opioid-free anesthetic techniques found evidence that opioid-based anesthesia did not reduce postoperative pain and was associated with increased PONV compared with OFA techniques. However, none of the 23 randomized trials comprising 1304 patients selected were in the bariatric surgery population [35].
Despite increasing numbers of anesthesia providers practicing opioid-free techniques for bariatric surgery, the available evidence for anesthetic best practices is limited to observational studies, case series, and small randomized trials. Ziemann-Gimmel, et al. found that OFA reduced the risk of PONV in bariatric surgery patients compared to standard volatile opioid-based techniques. However, PONV was only assessed at one time point and postoperative pain intensities, while similar between groups, were only assessed upon arrival in PACU without follow-up assessments [36]. Tufanogullari, et al. compared varying doses of intraoperative dexmedetomidine with desflurane on early and late recovery parameters in laparoscopic bariatric surgery patients. Although immediate postoperative fentanyl requirements were higher in the placebo group, morphine consumption was the same in all study groups during the first 2 postoperative days. Although dexmedetomidine patients required less antiemetic rescue medication, hospital length of stay was not affected [37]. When combined with sevoflurane anesthesia, intraoperative dexmedetomidine was associated with less postoperative opioid consumption and PONV when compared to remifentanil, although emergence from anesthesia was significantly prolonged in the dexmedetomidine group [38]. A retrospective analysis of 9246 bariatric surgery cases found reduced postoperative complications in patients with OFA. This was partially attributed to a combination of less pain, less PONV, faster recovery, and improved mobilization. However, the observational, non-randomized nature of this study limited the conclusions [5,39].
OFA would appear to be an attractive alternative in bariatric surgery patients, particularly for those with sleep disordered breathing. Over 70% of obese patients evaluated for bariatric surgery have obstructive sleep apnea (OSA), which can be aggravated by the administration of opioids or other sedatives. OSA may lead to postoperative adverse events, including cardiac events and respiratory failure [40,41]. Yet, OSA has not been shown to be an independent risk factor for postoperative hypoxemia in bariatric surgery patients [8]. CPAP is considered the mainstay of treatment for OSA and its application may mitigate postoperative complications in bariatric surgery patients independent of anesthetic technique used [42]. Similarly, bariatric surgery patients are at high risk for PONV due to the nature of the surgery and patient characteristics (young, female, non-smoking). PONV is distressing to patients, may delay hospital discharge and increase postoperative emergency department visits [43]. Our results did not show a difference in the incidence of PONV between OFA and OBA groups. This may have been influenced by our lack of a standardized OFA regime. Interestingly, propofol, a known antiemetic, was consistently administered by infusion in our OFA cohort without discernable benefit.
There are several limitations to this study. First, to reduce the impact of confounders our study cohort was restricted to patients of two surgeons undergoing laparoscopic sleeve gastrectomy at a single hospital center. While restriction of our cohort reduced the effects of confounding, it also limited the generalizability of our study findings. Furthermore, the observational nature of this study and the use of medical records limited our ability to control for unmeasured confounders and collect information on variables such as previous opioid use and baseline pain scores. The non-random assignment of patients to groups based on anesthesiologist preference could introduce selection bias, a point reinforced by clinical characteristics of OFA versus OBA groups. While it is unknown if patient risk factors such as OSA influence the rate or amount of postoperative opioid use, it is worth noting that there is a trend in the OFA group for a higher prevalence of HTN and OSA. Although this is not statistically significant at the p < 0.05 level, it could point to potential bias in the assignment of patients on the basis of these risk factors. It is also unknown, given the retrospective nature of this study, if certain patients expressed a preference to avoid opioid therapy that resulted in the use of OFA. Finally, given the observational nature of this study we cannot infer any causation, merely association, of OFA with similar patient recovery characteristics including rate of opioid use, incidence of PONV and LOS.
Although OFA techniques are increasingly described in the literature there is still no consensus on the ideal combination of agents or dosing regimens necessary to measurably improve patient quality of recovery, decrease hospital LOS, reduce hospital costs or favorably influence postoperative opioid misuse. Additionally, diluting and preparing multiple agents for administration via drug infusion devices adds a layer of complexity and preparation time that can become burdensome in high volume, rapid turnover practices. More high quality randomized clinical trials are needed to determine the cost effectiveness, utility and safety of OFA in improving clinically meaningful outcomes in bariatric surgery patients.
The authors declare no conflicts of interest, no associations, no consultancies.
The authors have no sources of funding to declare for this manuscript.
All authors contributed equally to this manuscript.