With the objective of identifying the best position for performing the lumbar puncture and identifying the distance from the skin to the interspinous space, 16 adult volunteers participating in measuring the distance with ultrasound between the lumbar region and the spinous processes in three positions: lateral decubitus, sitting and leaning forward, and sitting with the feet supported [1]. The study showed that the upright sitting position may offer advantages for performing lumbar puncture.
There are several positions to perform puncture of the subarachnoid space the most common are in sitting and lateral decubitus (Figure 1). However, there are two more important positions to perform other types of spinal anesthesia such as the prone position (Jack-knife position) (Figure 2) and in some patients operated on old orthopedic surgical tables, where there is a space between the back and the buttocks, the puncture can be performed in supine position with the needle inlet under the table (Figure 3).
 Figure 1: Sitting and lateral decubitus position.
View Figure 1
Figure 1: Sitting and lateral decubitus position.
View Figure 1
 Figure 2: Prona Position (Jack Knife Position).
View Figure 2
Figure 2: Prona Position (Jack Knife Position).
View Figure 2
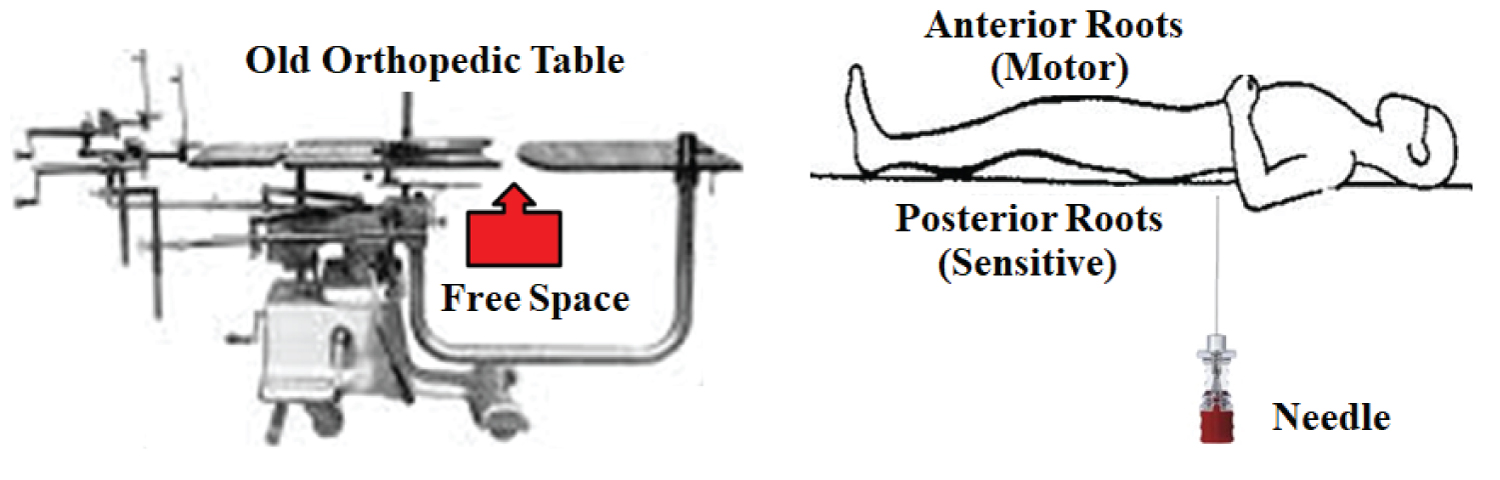 Figure 3: Posterior Puncture (Underneath the Orthopedic Table).
View Figure 3
Figure 3: Posterior Puncture (Underneath the Orthopedic Table).
View Figure 3
Consulting several ultrasound books and several articles teaching the approach to the neuraxis in the lumbar region, practically most of these studies report the performance only in the sitting position. The use of spinal hemianesthesia, which can be unilateral or posterior [2], are forgotten in the teaching of ultrasound use. In order to perform unilateral spinal anesthesia (left or right), it is essential to use hypobaric and hyperbaric solutions of local anesthetics [3], and it is essential to use the lateral position to approach the subarachnoid space and remain in this position long enough for the anesthetic not to pass to the other side. And the other positions, such as Jack-knife position for anorectal surgeries with hypobaric local anesthetics are ignored [4,5]. Likewise, the implantation of gluteal prosthesis under subsequent anesthesia can perfectly replace the use of epidural anesthesia, as well as other indications for plastic, anorectal and orthopedic surgeries [5].
In a meta-analysis published in 2014, they reported an excellent correlation between ultrasound-measured depth and needle insertion depth to the epidural or intrathecal space, showing significant evidence supporting the role of neuraxial ultrasound in improving the precision and efficacy of neuraxial anesthetic techniques [5]. In another systemic review and meta-analysis published in 2020, it was shown that ultrasound guidance for lumbar puncture is an effective technique, decreasing the risk of failure, decreasing the successful attempts and incidences of complications such as headache and back pain [6]. None of these two reviews addressed the different solutions of local anesthetics injected as well as the different puncture positions.
In a recent Editorial, the authors suggest that the evidence-base for ultrasound guidance for lumbar puncture, although growing, may be insufficient as a foundation for a position statement and is certainly insufficient to create a standard of care for hospitalists [7].
Much more important than the use of ultrasound to identify the subarachnoid space, is to understand the behavior of the different solutions of local anesthetics such as hypobaric, isobaric, hyperbaric and to correlate with the different puncture positions such as sitting, lateral decubitus, prone position (posterior spinal anesthesia) and on orthopedic tables with open space, in the dorsal position. During my entire life as a researcher in regional anesthesia, with a predominance of spinal anesthesia, I taught all the possibilities of performing a lumbar puncture. It is obvious that only those who are interested in offering the best to their patients should use these subarachnoid space puncture techniques.
In a recent article published in 2021, our group showed that spinal anesthesia is much more than a single shot of hyperbaric bupivacaine [8]. The question that generated the objectives of publishing this article was: "What is the reason to use spinal anesthesia with hyperbaric bupivacaine most of the time?" Having selected the following fundamental questions: 1) Ignorance of modern anatomy?, 2) Ignorance of the other solutions (isobaric and hypobaric)?, 3) Difficulty performing subarachnoid punctures in lateral decubitus and prone position?, 4) Difficulty changing the acquired habits?, 5) Lack of knowledge of the anterior and posterior roots?, 6) Ignorance of the safety of thoracic puncture?, 7) Unawareness of continuous spinal anesthesia?.
The objectives of this article were to address different forms of spinal anesthesia with other solutions such as hypobaric and isobaric, as well as other indications such as video cholecystectomy, segmental spinal anesthesia, thoracic spinal anesthesia, opioid-sparing spinal anesthesia and continuous thoracic spinal anesthesia [8]. At the conclusion of the article we say that the spinal anesthesia is old, simple, easy and a popular technique. Anatomy, physiology and pharmacology are very important and necessary for its understanding. Nothing is better than the freedom to decide what to do. Only knowledge.
The understanding of the anatomy of the thoracolumbar spine led to the development of thoracic spinal anesthesia, very well described by Jonnesco at the beginning of the 20th century [9], and which now provides several articles on the subject, such as the recent one with 1,406 patients, without any neurological sequelae [10]. The evolution of the understanding of the anatomy of the thoracolumbar spine with MRI [11-13], allowed the use of continuous thoracic spinal anesthesia [14,15].
Ultrasound is used to determine the needle insertion site, and this approach is supported by the largest set of evidence; however, this technique is mainly recommended for complicated punctures. I question: how to use it on difficult and complicated patients if you don't train on the easier ones? Several systems were created to guide the needle allowing the needle path to visualization in the fabric. These systems can potentially accelerating learning curves and increasing success rates in different types of puncture.
And this knowledge must be much greater and more important than the use of technology to identify the space to be punched. The most important thing in spinal anesthesia is the full knowledge of the different solutions, the different lumbar puncture techniques and the use of the different puncture positions. Indeed, the use of ultrasound made possible new and excellent blocks for different types of application, but for use in the neurax is it will be necessary to describe all the other possibilities of puncture.
In a recent Editorial the authors conclude that the evidence-base for ultrasound guidance for lumbar puncture, although growing, may be insufficient as a foundation to a position statement and is certainly insufficient to create a new standard of care for hospitalists [7]. We really shouldn't be against new technologies, but spinal anesthesia is much more than the use of a sitting position, exhaustively studied with ultrasound, we should have the obligation to study all the puncture positions with this new technology, to open up new possibilities of the use of these techniques, which few anesthesiologists are familiar with.
Finally, it is essential that, for ultrasound to be a routine method for performing spinal anesthesia, all puncture positions are exhaustively studied, otherwise only the sitting position will be privileged. Furthermore, ultrasound should be used in all patients and not only in those with a precise indication, as some authors defend. Recently, in an article we showed that spinal anesthesia is much more than the injection of local anesthetic hyperbaric in the sitting position [8], in this way the use of ultrasound for lumbar puncture should be much more than the use in the sitting position. In conclusion, the use of ultrasound would be interesting for the use of thoracic spinal anesthesia by several other anesthesiologists, as recently published in this journal [10,16].