Hyponatremia is observed in children with meningitis, encephalitis, pneumonia, urinary tract infections, and Kawasaki disease. The presence of hyponatremia is associated with increased morbidity and mortality in adults. The clinical significance of hyponatremia in febrile pediatric patients is unknown. The objective of this study was to evaluate the prevalence and prognostic value of hyponatremia in children presenting to the emergency department (ED) with systemic inflammatory response syndrome (SIRS).
This retrospective study included children 1-19 years-old presenting to the ED between January - December 2014 with fever and SIRS. Exclusion criteria included comorbidities affecting sodium levels such as diuretic use, renal insufficiency, hyperglycemia, or immune deficiencies. Hyponatremia was defined as serum sodium of < 132 mEq/L; the primary outcome was hospital admission. Continuous non-normal variables were described as median and interquartile range. Categorical variables were compared using Chi-squared or Fisher's Exact Tests. Spearman correlation was evaluated between nonparametric variables. Level of significance was set at 0.05.
Out of 4,791 patients, 663 met inclusion criteria by having electrolytes collected and by triggering SIRS Best Practice Alerts. Hyponatremia occurred in 19%. Patients with hyponatremia were older (P = 0.04) and had higher maximum body temperature (P < 0.001), white blood cell counts (P = 0.04), and C-reactive protein levels (P = 0.004). Patients with hyponatremia also had higher rates of admission (P = 0.003, OR = 1.9, 95% CI [1.3-2.9]) and bacteremia (P = 0.009).
Hyponatremia is often found among pediatric patients presenting to the ED with febrile SIRS and is associated with increased morbidity.
Hyponatremia, Emergency department, Systemic inflammatory response system
SIRS: Systemic Inflammatory Response Syndrome; ED: Emergency Department; UTI: Urinary Tract Infection; CRP: C-Reactive Protein; AVP: Arginine Vasopressin; ICU: Intensive Care Unit; HER: Electronic Health Record; BPA: Best Practice Alert; IRB: Institutional Review Board; CRH: Corticotropin Releasing Hormone; ACTH: Adrenocorticotropic Hormone; WBC: White Blood Cell Count; PCT: Procalcitonin; IL-1: Interleukin 1; IL-6: Interleukin 6; TNF: Tumor Necrosis Factor; SIADH: Syndrome of Inappropriate Anti-Diuretic Hormone; T1DM: Type-1 Diabetes Mellitus; DKA: Diabetic Ketoacidosis; OR: Odds Ratio; SD: Standard of Deviation; CI: Confidence Interval
Hyponatremia is the most common disorder of electrolytes encountered in clinical practice and is highly prevalent in critically ill children [1-3]. Variable degrees of hyponatremia occur in up to 30% of hospitalized patients [4,5]. In the pediatric population, hyponatremia is often observed in patients with acute inflammatory diseases and infections such as meningitis, pneumonia, bronchiolitis, urinary tract infections, Kawasaki disease, and febrile seizures [6-13]. Most hyponatremic states are characterized by inappropriately elevated plasma levels of arginine vasopressin (AVP) [14], which is released to preserve intravascular volume by promoting free water resorption in the connecting and collecting tubules of the nephron. Systemic inflammatory response syndrome (SIRS), fever, pain, infections, and subclinical volume depletion are among the non-osmotic stimuli of AVP [15-17].
While most hyponatremia is asymptomatic, untreated acute hyponatremia can cause substantial morbidity and mortality as a result of osmotic dysregulation and cerebral edema resulting in seizures, coma, respiratory arrest, and permanent brain damage [18-20]. Brain swelling in the pediatric population is less well tolerated than adults and is associated with significant morbidity and mortality [21]. In hospitalized adult patients, the presence of hyponatremia is frequently associated with increased mortality and worsened outcomes. Hyponatremia is associated with higher rates of mechanical ventilation, intensive care unit (ICU) admission, longer ICU and hospital lengths of stay (LOS), and increased mortality in adults with pneumonia [22-24]. The presence of hyponatremia is also an important predictor for poor outcome in critically-ill adults hospitalized for other infectious and noninfectious etiologies [25,26]. Early detection of hyponatremia is essential for proper fluid management and to avoid potential complications.
Despite the well-established associations of hyponatremia in adult population, its prevalence and clinical significance in pediatric emergency department (ED) patients presenting with SIRS remains incompletely understood. This study is designed to evaluate the prevalence and clinical impact of hyponatremia in children presenting with SIRS to the pediatric emergency department.
The study was approved by the local institutional review board. This retrospective study was conducted by accessing the electronic health record (EHR) (Epic Systems; Verona, WI, USA) and was limited to children between the ages of 1 to 19-years-old presenting to the emergency department of a tertiary free-standing children's hospital located in northeast Ohio. The emergency department has ~100,000 annual encounters. The EHR was interrogated over a 12-month period (January-December 2014). Hyponatremia was defined as serum sodium < 132 mEq/L based on the reference range established by our institution's laboratory (133-145 mEq/L). Using the 2005 pediatric sepsis criteria [27] a series of logic rules were installed into the EHR that triggered a Best Practice Alert (SIRS-BPA) when two out of three criteria (one being abnormal temperature) were satisfied for SIRS. SIRS criteria included: Temperature instability defined as a temperature of > 38.5 ℃ or < 36 ℃. Tachycardia was defined as a mean heart rate > 2 SD above normal for age. Bradycardia was defined as a mean heart rate < 10th percentile for age. Tachypnea was defined as a mean respiratory rate > 2 SD above normal for age. All patients who presented with temperature instability and triggered the SIRS Best Practice Advisory (BPA) were included in the initial cohort. Patients without a basic metabolic panel were excluded.
Patients were excluded if they had an underlying medical condition affecting sodium levels including: Adrenal insufficiency, type- I diabetes mellitus (T1DM) with elevated blood sugar, heart failure, diuretic therapy, kidney failure, or those on chronic steroid therapy. In addition, we elected to exclude patients who were less than one-year-old due to the high frequency of hyponatremia in term and premature neonates [28,29], and the variations in fever management in infants and neonate. Finally, patients with immunosuppression (primary/secondary immune deficiency, receiving a current chemotherapy regimen, or those with sickle cell disease) were also excluded since the presence of immune deficiency is independently associated with higher admission rate. Six hundred and sixty-three patients fulfilled the inclusion criteria and were included in this study (Figure 1). The relationship between hyponatremia, ED disposition, associated metabolic/laboratory derangements and final diagnosis was analyzed. The diagnosis of urinary tract infection, pyelonephritis, or bacteremia was based on final culture results and contaminants were excluded. The diagnosis of pneumonia was done on the basis of chest x-ray findings consistent with pneumonia in addition to clinical signs and symptoms of lower respiratory tract infection. Dehydration was a clinical diagnosis given by the ED provider and was considered in the presence of decreased oral intake, urine output, repeated emesis and/or diarrhea, in addition to clinical signs of dehydration on examination. Patient admission was determined by the ED providers and included observation for less than 24 hours and admission to the acute care ward or PICU. Discharge was defined as a successful discharge to outpatient care without returning to the ED or direct admission within 7 days for similar symptoms or complaint.
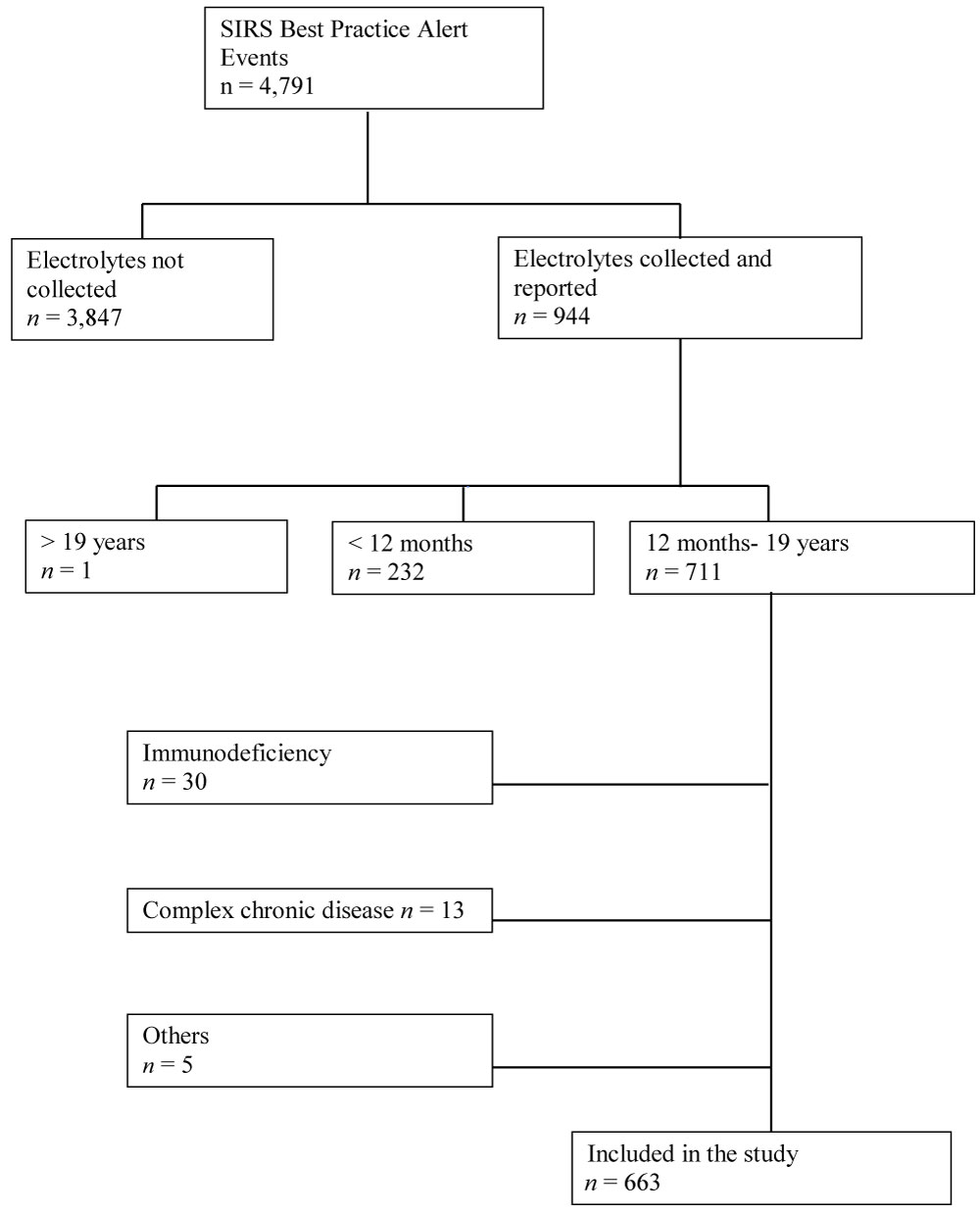 Figure 1: Patient selection for study enrollment. Complex chronic disease included: Cystic fibrosis, T1DM with DKA, renal failure, chronic cardiac disease, and complex non-verbal patients. Others: one patient deceased and records were not accessed. Three patients with false alert and fever was reported or measured, and one patient was transferred to another facility for admission with no known outcome or final diagnosis.
View Figure 1
Figure 1: Patient selection for study enrollment. Complex chronic disease included: Cystic fibrosis, T1DM with DKA, renal failure, chronic cardiac disease, and complex non-verbal patients. Others: one patient deceased and records were not accessed. Three patients with false alert and fever was reported or measured, and one patient was transferred to another facility for admission with no known outcome or final diagnosis.
View Figure 1
Statistical analysis was carried out using SAS (version 9.4; SAS Institute Inc., Cary, NC, USA). Continuous nonparametric variables were described as median and interquartile range. Categorical variables were compared using Chi-squared or Fisher's Exact Tests. The Wilcoxon Rank Sum Test was applied to compare nonparametric variables between groups. Spearman correlation was calculated between nonparametric variables. Level of significance was set at < 0.05.
Six hundred and sixty-three patients with SIRS were included in the study (Figure 1). Table 1 displays the demographic and the clinical characteristics of all patients. The minimum age was one year with the median age of 4 years (IQR: 2-8 years). There were similar numbers of females (51%) and males (49%). The most common primary diagnosis was viral illness (36%), followed by pneumonia (9%). The most common secondary diagnosis was dehydration (26%).
Table 1: Demographic and clinical characteristics of patients presenting at the emergency department with SIRS best practice alert events and with corresponding electrolyte evaluation. View Table 1
Hyponatremia was identified in 19% of patients with SIRS and laboratory testing. Patients with hyponatremia were older (5 vs. 4 years, P = 0.04), and had higher maximum body temperatures in the ED (39 ℃ vs. 38.7 ℃, P < 0.001), higher white blood cell counts (WBC) (13.5 vs. 11, P = 0.04) and higher C-reactive protein (CRP) levels (7.2 vs. 3.5, P < 0.004), Table 2. There was a negative correlation between sodium levels and the recorded maximum temperature in the ED (r = -0.18, P < 0.0001), CRP level (r = -0.24, P = 0.0002), and WBC (r = -0.10, P = 0.017).
Table 2: Demographics, clinical and lab characteristics of hyponatremia groups. View Table 2
Patients with hyponatremia had higher admission rates (71% vs. 56%; P < 0.003, Table 3). Patients with hyponatremia had 1.9 times the odds of hospitalization compared to controls (OR = 1.9, 95% CI [1.3-2.9]). Additionally, patients with hyponatremia had higher rates of bacteremia (8% vs. 2%, P = 0.009). The prevalence of hyponatremia among different diagnoses is shown in Figure 2. Patients with meningitis, bacteremia, urinary tract infections, neck abscesses and streptococcal pharyngitis demonstrated higher prevalence of hyponatremia.
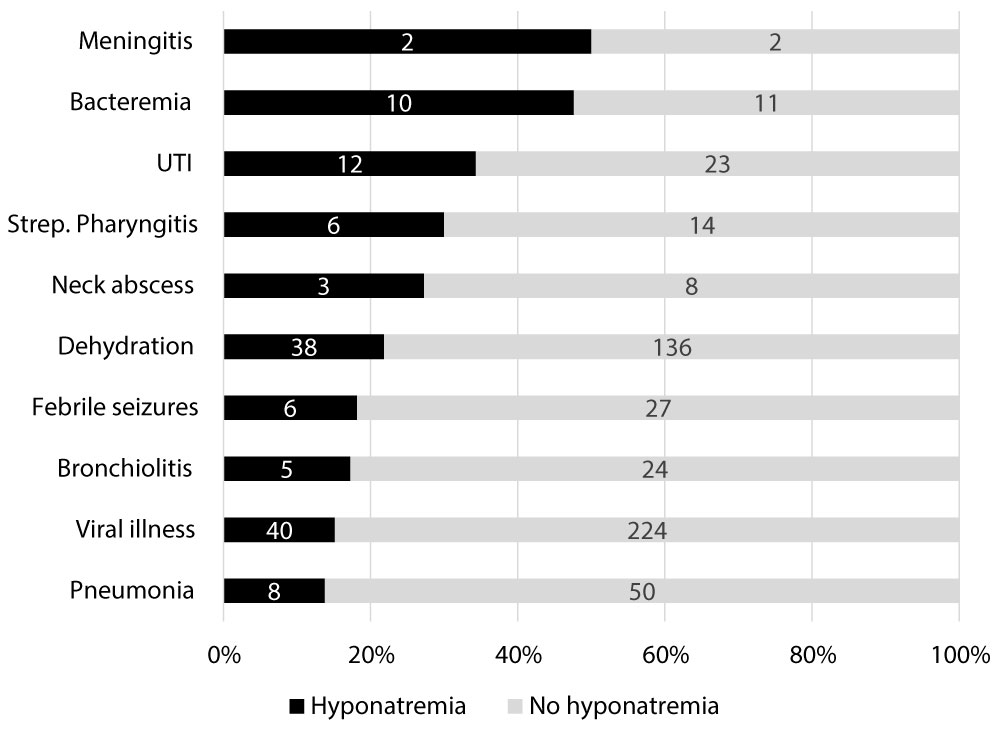 Figure 2: The breakdown of hyponatremia/no hyponatremia by percentages for each diagnosis. Those with meningitis (n = 4) had the most frequent occurrence of hyponatremia followed by bacteremia (n = 21), UTI (n = 35), strep pharyngitis (n = 20). Lowest incidence of hyponatremia occurred in those with viral illnesses (n = 264) and pneumonia (n = 58).
View Figure 2
Figure 2: The breakdown of hyponatremia/no hyponatremia by percentages for each diagnosis. Those with meningitis (n = 4) had the most frequent occurrence of hyponatremia followed by bacteremia (n = 21), UTI (n = 35), strep pharyngitis (n = 20). Lowest incidence of hyponatremia occurred in those with viral illnesses (n = 264) and pneumonia (n = 58).
View Figure 2
The prevalence and the clinical associations of hyponatremia have been established in febrile adult patients. To our knowledge, this is the first report that focused on the prevalence and clinical importance of hyponatremia in pediatric patients presenting with SIRS to the ED. Our study revealed that hyponatremia in this cohort was associated with higher admission rates.
While other studies utilized sodium levels of < 135 mEq/L to define hyponatremia, we elected to utilize a more stringent definition of sodium ≤ 132 mEq/L in our pediatric population. A sodium level > 132 mEq/L is considered by many to be a normal value in infants and young children including our institutional laboratory reference. Despite this approach, we found that the prevalence of hyponatremia among pediatric patients presenting with SIRS to the ED was 19%. This was significantly higher than the prevalence among pediatric (3%) [30] and adult patients (3-4%) [31,32] previously reported, although prior studies included all patients in the ED.
The prevalence of hyponatremia varies widely depending on the etiology and patient population being evaluated. Hyponatremia has been reported in up to 25% of patients admitted to critical care units, [33] and in 6% to 42% of hospitalized patients [34,35]. While hyponatremia in patients presenting to the ED was attributed to hypovolemia and gastroenteritis in up to 65% of patients [26], hyponatremia in hospitalized patients was most frequently associated with normovolemia, regularly attributed to stress response, and ultimately a predictor of poor outcome [2,36,37]. Our study cohort did not represent a random sample of patients presenting to the ED, but rather were among the sickest patients with obvious concerns for infection. All of our patients met SIRS criteria and required intravenous catheter placement for diagnostic laboratory testing, intravenous fluids, or other interventions. Therefore, our study population more closely resembled hospitalized patients than the general ED population. Despite the high concordance of clinical dehydration and SIRS in our study group, the incidence of hyponatremia was not significantly higher in patients with dehydration. Thus, we speculate that the higher incidence of hyponatremia in our study cohort can be attributed to greater illness severity rather than dehydration alone.
To further elucidate the relation between SIRS and hyponatremia, we evaluated the correlation between hyponatremia and the maximum recorded temperature during the ED visit. We found that the presence of hyponatremia was correlated with higher maximum temperature in the ED. This is consistent with Hasegawa, et al. who reported that the prevalence of hyponatremia was significantly higher in febrile versus afebrile children at hospital admission [5]. Hyponatremia in the febrile population is thought to be due to increased arginine vasopressin (AVP) secretion induced by fever to offset insensible losses and thereby maintain body fluid homeostasis and effectively cause the body to retain more water [16,38-40].
This study also found that hyponatremia was correlated with increased CRP and WBC count. Other studies have found hyponatremia to be associated with increased WBC count, elevated CRP, increased PCT levels, and disease severity [4,8,10,35,41]. Hyponatremia was also recently found to be a predictor for complicated gangrenous or perforated appendicitis [42], increased disease severity in children with pneumonia [5], and severity of inflammation in children with febrile UTIs [7]. During acute infections such as these, Eisenhut, et al. postulated that inflammatory mediators such as Interleukin-1 (IL-1) and Tumor Necrosis Factor (TNF) alter expression of ion channels in renal cells, thereby resulting in hyponatremia [7,43]. Other studies have suggested that hyponatremia in SIRS results not only from renal dysfunction but also from increased AVP secretion induced by inflammatory cytokines such as IL-1beta, IL-6, and TNF [7,10,44]. These same cytokines act as endogenous pyrogens [39,45]. This may serve to explain the higher prevalence of hyponatremia among patients with SIRS who have fevers and elevated inflammatory markers.
Our study revealed that patients with bacteremia had a higher prevalence of hyponatremia (Figure 2). In our population, 48% of those with bacteremia were found to have hyponatremia (P = 0.008). This echoes an earlier report by Jensen and colleagues who concluded that hyponatremia was associated with the development of hospital-acquired Staphylococcus aureus bacteremia [46]. The prevalence of hyponatremia was also higher among patients with urinary tract infection, neck abscess, streptococcal pharyngitis, and meningitis. The incidence of meningitis was low in our study cohort (n = 4); nonetheless, fifty percent of patients with meningitis had hyponatremia. Comparable results were found in other studies; one study of adults with group A streptococcus meningitis as 20 out of 35 (58%) had hyponatremia [12,47]. In this study 30% of those with strep pharyngitis, 27% of children with neck abscesses, and 34% of those with UTI developed hyponatremia; by comparison only 15% of those with viral illness developed hyponatremia. These results suggest that presence of hyponatremia is higher in those with more severe bacterial infections as opposed to viral infections. Pneumonia was the second most common presenting diagnosis in our study cohort; however, only 14% of those diagnosed with pneumonia met criteria for hyponatremia. This was lower than the reported prevalence of hyponatremia among children (45%) [41], and adults (28%) with pneumonia [23] in prior studies. Use of a more stringent definition of hyponatremia may have contributed to the lower prevalence of hyponatremia in our pediatric pneumonia patients.
Hyponatremia was significantly associated with higher rates of hospital admission. These results are in agreement with prior adult and pediatric studies which demonstrated that the presence of hyponatremia was associated with greater illness severity, higher admission rates, and longer hospital stay [12,17,20]. The current study showed that 71% of patients with sodium ≤ 132 mEq/L required admission, suggesting that hyponatremia did correspond with increased severity of illness. Unlike the adult population, however, the presence of hyponatremia in our patients was not associated with prolonged hospital stay, neurologic decompensation, or death. This is consistent with previous reports demonstrating that hyponatremia and SIADH in children with febrile illness is rarely symptomatic [6,48]. It is also likely that earlier identification of hyponatremia in the ED resulted in appropriate isotonic rather than hypotonic fluid administration in admitted patients. In the adult population, correction of hyponatremia during hospitalization attenuated the increased risk of mortality associated with hyponatremia [25]. Therefore, early identification and proper management of hyponatremia is critical to reduce its potential complications.
Given the high incidence of hyponatremia (19%) among our pediatric patients with SIRS, caution should be employed when choosing intravenous fluid therapy for patients with infection. Many studies have shown that hypotonic fluids significantly increase the risk of developing hyponatremia [49-51]. Additionally, adverse events including encephalopathy, seizures, stupor, and death was reported to occur in roughly 2% of those receiving hypotonic fluids [49,50]. This is why the newest American Academy of Pediatrics guideline on intravenous fluid management recommends routine use of isotonic fluids [52]. Taken together, identification of hyponatremia and proper fluid management can potentially reduce the risk of poor outcome in pediatric patients with SIRS.
Our study is not without limitations. Only patients with SIRS who were judged by the evaluating clinician to require assessment of electrolytes were included in the study introducing a potential for bias. As a tertiary children's hospital many patients are referred from community hospitals. This study did not account for labs obtained at the referring hospital or during inter-facility transport, though the impact of that in either over or underestimation of hyponatremia cannot be predicted. Additionally, the mechanism of hyponatremia could not be elucidated as total body water and serum osmolality were not systematically assessed. Regardless, the current study demonstrates that hyponatremia is an electrolyte abnormality in pediatric patients with SIRS that is associated with higher rates of admission and bacteremia. Further studies are needed to elucidate the mechanism of hyponatremia in this population.
Hyponatremia is identified in pediatric patients presenting with SIRS to the ED. It is correlated with higher admission rates, higher temperatures, elevations in WBC count and CRP. Among a variety of infectious etiologies, the incidence of hyponatremia was significantly higher in patients with bacteremia. Hyponatremia should be considered in patients presenting with SIRS, and may guide appropriate fluid management.
We would like to give a special thanks to the Rebecca D. Considine Research Institute. The authors declare no conflict of interest.
There is no external funding for this manuscript.
Dr. El-Assal conceptualized and designed the study, coordinated and supervised data collection, and drafted the initial manuscript, and reviewed and revised the manuscript. Dr. Marzec, Dr. Forbes, Dr. Bigham, Dr. Solomon, and Dr. Reichert, and Ms. Brown, participated in data collection, analysis or interpretation and reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.