Shock is a pathological condition characterized by imbalance between oxygen demand and supply. Irrespective of the cause, shock leads to a state of energy failure due to a decrease in adenosine triphosphate (ATP) production, creation of lactic acidosis, and as a consequence, multiple organ dysfunction [1].
Lactic acidosis is an ominous finding in critically ill patients. The severity and increased duration of lactic acidosis are associated with increased mortality [2]. Lactic acidosis can result from hypoperfusion and hypoxia (Type A lactic acidosis) or decreased utilization of oxygen by the tissues (Type B Lactic Acidosis) [3].
As a part of ATP production, glucose is metabolized to pyruvate during glycolysis. Pyruvate is then metabolized by pyruvate dehydrogenase (PDH), which connects glycolysis to the Krebs cycle. Within the Krebs cycle, the α-ketoglutarate dehydrogenase (α-KGDH) complex, a key rate-limiting enzyme involved in mitochondrial energy metabolism, requires the presence of oxygen as well as functional enzymes to generate adequate ATP [4]. In the setting of hypoxia or dysfunctional enzymes, pyruvate is channeled into the Cori cycle which results in lactic acidosis. Thiamine or Vitamin B1 is a water-soluble vitamin that plays an essential role in carbohydrate, protein, lipid, and neurotransmitter metabolism. After conversion into thiamine pyrophosphate, it serves as a cofactor for both the PDH and the α-KGDH complex. Thiamine deficiency results in dysfunctional PDH and α-KGDH complexes, resulting in an inability to enter the Krebs cycle and subsequent activation of the Cori cycle, resulting in lactic acidosis, energy failure that can lead to multiorgan dysfunction and death [5].
Thiamine deficiency can result in a variety of distinct clinical presentations. In its more widely known form, Beriberi disease, it can present as a "wet" cardiac form or a "dry" neurologic form [6]. Thiamine deficiency can cause a more rapid/severe presentation known as Shoshin beriberi, resulting in acute cardiovascular collapse and severe lactic acidosis [7] as well as acute pulmonary hypertension [8].
We report- the case of a 2-year-old boy who received bone marrow transplant as a treatment for stage IV neuroblastoma. He was transferred to the pediatric intensive care unit (PICU) with progressive vasodilatory shock and lactic acidosis despite aggressive cardiopulmonary support, improving within hours, following one dose of intravenous thiamine.
A 2-year-old boy with stage IV neuroblastoma was admitted to the hospital for his first planned autologous stem cell rescue following high dose chemotherapy. Two weeks prior to transplant he was diagnosed with pneumatosis intestinalis, which led to the cessation of all enteral feeds and subsequent initiation of total parenteral nutrition (TPN) as his sole source of nutrition. Shortly after TPN was initiated, he was noted to have an allergic reaction with hives and wheezing which was attributed to multivitamins in the TPN, so they were removed from his ongoing nutrition. He underwent autologous stem cell rescue after high-dose chemotherapy consisting of thiotepa (10 mg/kg per day × 3 days) and cyclophosphamide (50 mg/kg per day × 4 days). He tolerated it well and engrafted by day +12. He was progressing very well and ready for discharge. Day +19 post-transplant, he was noted to have tachycardia, developed acute hypoxemia and hypotension despite appearing clinically well. He was immediately worked up for sepsis and was started on Cefepime and Vancomycin. He was found to have metabolic acidosis and a lactate of 10.8 requiring transfer to the PICU.
Upon arrival to PICU, he remained hemodynamically unstable requiring aggressive fluid resuscitation as well as vasopressor and inotropic support including norepinephrine, epinephrine, and vasopressin. His diastolic blood pressures were disproportionately low with wide pulse pressures. His blood gas demonstrated an uncompensated metabolic acidosis (pH = 7.20, pCO2 = 44 mmHg, pO2 = 381 mmHg, HCO3 = 17 mEq/L, Base Deficit = -9.3 mEq/L, SaO2 = 100%). Interestingly his ScvO2 remained 76% despite high lactate of 11.5 mmol/L. He was electively intubated due to hemodynamic instability, shock, and rising lactate to reduce metabolic demands. Initial differential diagnosis included septic shock or ischemic bowel, with his history of pneumatosis pre-transplant. A computed topography (CT) abdomen and pelvis was obtained, which demonstrated enteritis involving small bowel, distal colon to rectum with no concern for bowel necrosis. His abdominal examination revealed no acute pain and surgery didn't feel his abdomen was the source. CT head showed a mild hypodensity in the posterior white matter and cerebellum. A follow-up MRI later showed Artery of Percheron infarction and bilateral thalamic infarcts. Antibiotics were optimized to include meropenem and vancomycin for presumed sepsis in the setting of neutropenia, enteritis, and shock. His echocardiogram showed more than half systemic right ventricular systolic pressure along with left ventricular diastolic dysfunction. His biventricular systolic function was normal. He was started on inhaled nitric oxide which resulted in a transient improvement in his hemodynamics. His inflammatory markers (CRP and Procalcitonin) were not significantly elevated and both urine and blood cultures showed no growth.
Despite this management, there was persistent severe metabolic acidosis with progressive rise in lactate over the next 24 hours. He developed significant polyuria with urine output exceeding 40 ml/kg/hour which was replaced continuously. His urine studies were suggestive renal tubular dysfunction with a combined loss of water and electrolytes (Serum Osmolality = 276 mOsm/Kg, Serum Na = 130 mEq/L, Urine Osmolality = 307 mOsm/Kg, Urine Sodium 136, Urine Calcium = 9.3 mg/dL). Sodium bicarbonate and calcium gluconate infusions were initiated to buffer the metabolic acidosis and to treat the persistently low ionized calcium.
Despite his hemodynamic instability and lactic acidosis, he had brisk capillary refill and his central venous saturation consistently remained above 70%. His shock remained refractory to all treatments and ECMO was discussed multiple times.
With his unique clinical picture, a very careful review of other potential contributors in his history was done. We found that although he was on TPN prior to PICU admission, multivitamins had been excluded from the TPN for about 5 weeks due to concerns allergy to a component in the multivitamin formulation. Blood levels for vitamins were drawn and a dose of Thiamine 50 mg intravenous was immediately administered. Following the single dose of thiamine, the patient had dramatic improvement in hemodynamics, lactic acidosis (Figure 1), and urine output. The vasopressors and inotropes were weaned off quickly, within eight hours of the thiamine administration. He was extubated within 24 hrs and transferred back to the oncology floor within 48 hrs of vitamin administration. He was discharged home five days later, with clinic follow up and is doing extremely well.
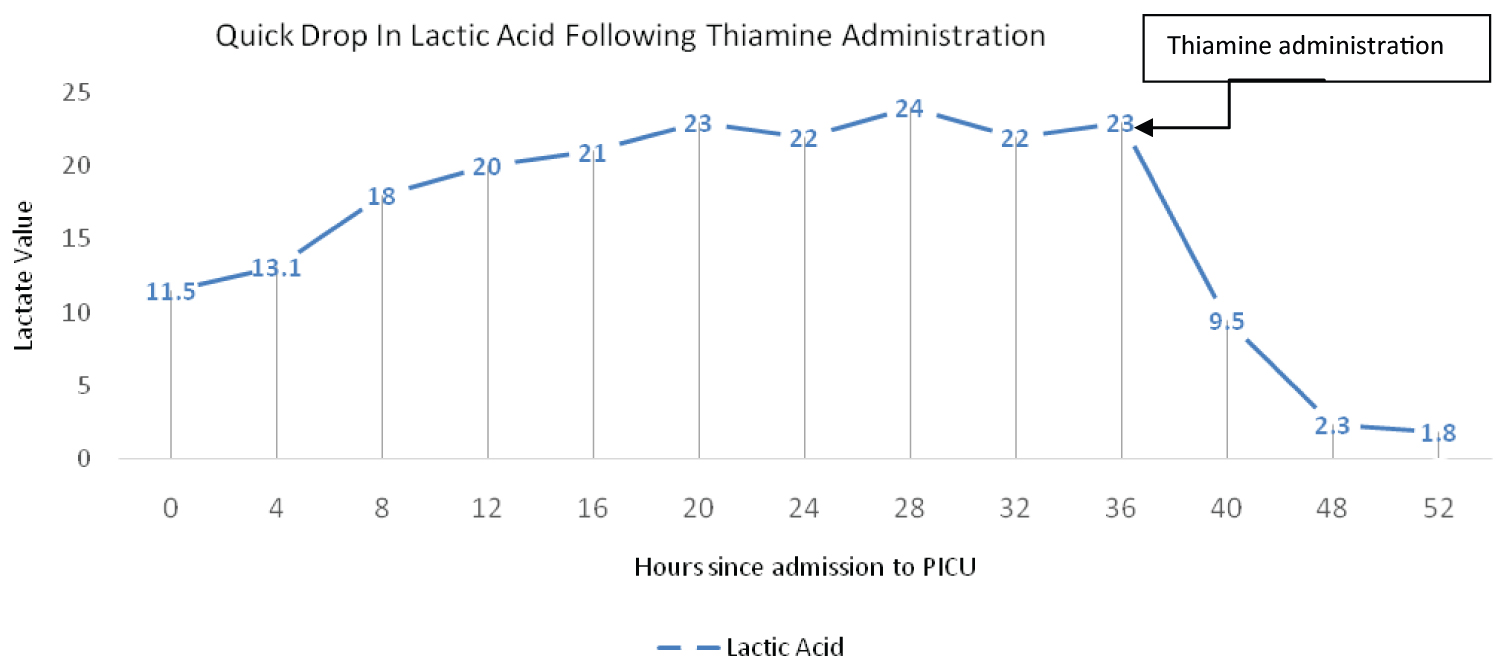 Figure 1: Lactate trend after admission to PICU.
View Figure 1
Figure 1: Lactate trend after admission to PICU.
View Figure 1
Results of his vitamins levels, prior to thiamine administration resulted several days later and were notable for a Thiamine (B1) level of 44 nmol/L (normal 70-180), Riboflavin (B2) level of 1 nmol/L (normal 5-50), Pyridoxine (B6) level of < 5 nmol/L (20-125), Ascorbic Acid (C) level of < 5 Microgram/L (normal 23-114), and Folic Acid level of 1.3 ng/mL (normal > 5.9).
Thiamine deficiency is the only plausible explanation of this patient's presentation, with such dramatic improvement following thiamine administration. He continues on multivitamin supplementation since discharge.
For clinicians taking care of critically ill children, lactic acidosis is reflective of inadequate oxygen delivery caused by low cardiac output or low arterial oxygen content. Patients are tachycardiac, have poor peripheral perfusion, low central venous saturations, and oliguria. If sepsis is ruled out, other causes of lactic acidosis should be investigated.
Thiamine plays an important role in cellular and mitochondrial energy production. It is a cofactor for the PDH needed for the conversion of pyruvate into acetyl-CoA and subsequent entry into the Krebs cycle for ATP production. Thiamine deficiency will lead to pyruvate excess which is alternatively metabolized via the Cori cycle and lactate dehydrogenase into lactate with resultant lactic acidosis [9]. Metabolism of glucose in glycolysis alone produces net two molecules of ATP compared to its complete oxidation which produces almost 30 molecules [10]. This leads to an ATP deficient, and therefore energy deficient state with resultant multiorgan dysfunction.
Traditionally, thiamine deficiency was almost exclusively attributed to alcohol consumption. Thiamine deficiency has also been seen in other conditions associated with malnourishment such as bariatric surgery, Crohn's disease, and prolonged TPN with inadequate support of thiamine or among children whose diets were identified as being deficient in thiamine [11]. Recent evidence suggests that septic patients admitted to the intensive care unit have a higher mortality if they also have thiamine deficiency [12].
Hematopoietic stem cell transplant (HSCT) patients are especially vulnerable to thiamine deficiency through multiple cancer and treatment mediated mechanisms. For example, treatment related anorexia and vomiting limits absorption of thiamine from dietary sources. Chemotherapies and calcineurin inhibitors, typically administered during hospitalization for HSCT, also impair thiamine conversion to its biologically active form [13].
Thiamine deficiency is a rare but possible presentation, even in developed countries, especially in vulnerable populations, due to medical errors, or manufacturing issues. Fattal-Valevski, et al. reported 9 infants from Israel with thiamine deficiency with lactic acidosis due to administration of infant formula that was deficient in thiamine [14]. Ramsi M, et al. reported a 16-year-old with severe lactic acidosis with multiorgan dysfunction with thiamine deficiency due to thiamine deficient TPN during national multivitamin shortage [15]. Finally there was another report of thiamine deficiency a result of a medical error where multivitamins were not added to parenteral nutrition in a vulnerable patient as reported by Clémence Didisheim, et al. [16]. Irrespective of the cause, a high degree of suspicion is required when a patient with risk factors presents with signs and symptoms that are compatible with thiamine deficiency and are not responsive to conventional treatment.
Our patient presented with shock associated with brisk capillary refill, low diastolic blood pressures likely due to vasoplegia, pulmonary hypertension (PH), left ventricular diastolic dysfunction, and normal biventricular systolic function which is a presentation that has been previously reported in literature [8,17]. Moderate to severe PH is common in thiamine deficient patients. Usha M K Sastry, et al. reported 250 thiamine deficient infants who had PH due to dietary deficiencies, 231 infants responded to thiamine administration with complete resolution of their PH within 24-48 hours and no recurrence of PH at 60 months follow up [18]. In our patient we tried inhaled nitric oxide in the acute setting with some improvement in hemodynamics however, repeat echocardiography days after administration of thiamine showed resolution of pulmonary hypertension.
Rapid resolution of lactic acidosis following thiamine administration is reported by various authors [7,16,17,19]. Our patient's lactic acidosis resolved within twelve hours of thiamine administration, and he was weaned off all the three inotropes and vasopressors.
Interestingly, our patient had significant polyuria (40 ml/kg/hour) along with hypocalcemia, a presentation that likely represents renal tubular dysfunction in the setting of energy deficient state. Additionally, the MRI findings were typical for an infarction in the territory of the artery of Percheron (AOP), which is a posterior cerebral circulation variant characterized by a single trunk which supplies blood to the paramedian thalami and the rostral midbrain bilaterally. This infarction is rare and presents with features termed as paramedian thalamic syndrome. The differential diagnosis for the AOP infarction is Wernicke encephalopathy (WE) [20], however our patient did not have the neurological examination consistent with WE.
Thiamine deficiency and resultant life-threatening complications are likely under-realized and under-diagnosed. Thiamine deficiency must be in the differential diagnosis of shock, lactic acidosis and multiorgan dysfunction especially if the patient's clinical trajectory is unusual and clinical risk factors for thiamine deficiency are present. Treatment with thiamine is safe, response is rapid, and failure to recognize and treat this condition has tragic consequences. This review reminds clinicians of the importance of routine thiamine supplementation and assessment.
Further prospective studies are needed to identify target populations where empiric administration of thiamine should be considered earlier during presentations consistent with refractory shock.