Background: Calcification of the pericardium due to recurrent inflammation is a rare condition which can lead to severe restrictive cardiomyopathy. This case demonstrates severe circumferential pericardial calcification leading to cardiogenic shock and death. It is proposed that the patient's history of repeat cardiac interventions, including cardiac ablation, and open valve repair procedures precipitated this.
Case Presentation: 78-year-old Caucasian man presented for syncope, dyspnea on exertion, and chest pain. Past medical history significant for atrial fibrillation, requiring cardiac ablation procedures, along with severe mitral regurgitation requiring open valve replacement, He was found to have severe restrictive cardiomyopathy in the setting of a circumferentially calcified pericardium discovered on chest imaging. The patient was transferred to the cardiovascular intensive care unit in cardiogenic shock. Cardiothoracic surgery was consulted, and pericardial stripping procedure was performed. Despite this intervention, the patient developed septic shock and passed away.
Conclusions: This case highlights the importance of early identification in patients with risk factors for pericardial calcification, namely, multiple prior cardiac interventions such as open valve replacements, and cardiac ablations. Early diagnosis with radiographic imaging can impact outcomes for patients with this condition.
Calcified Pericardium, Constrictive Cardiomyopathy, Cardiac Ablation, Cardiogenic Shock
Our case proposes that prior cardiac surgeries, including cardiac ablation procedures for atrial fibrillation, and open valve repairs, can precipitate recurrent inflammation and subsequent pericardial calcification. The risk of cardiac inflammation and pericarditis following such procedures has been well described in the literature. The aim of this case report is to highlight the clinical considerations and differential diagnoses that should be included in the evaluation of patients with such risk factors.
A 78-year-old man presented to the emergency room of an outside hospital for burning chest pain, generalized weakness, severe dyspnea on exertion, and syncopal episodes over three days. The initial physical exam revealed coarse breath sounds and pitting edema in bilateral lower extremities. Initial laboratory workup was significant for elevated pro-BNP, leukocytosis, acute kidney injury, and elevated transaminases. Imaging with CT of the chest, abdomen, and pelvis was significant for bilateral pleural effusions and extensive pericardial calcification with small pericardial effusion. [Figure 1 and Figure 2] There was also evidence of cardiac liver cirrhosis and ascites. Patient was transferred to a tertiary care center (Mercy, St. Louis) for cardiothoracic intervention. He underwent sternotomy with pericardial stripping for cardiogenic shock secondary to constrictive pericarditis. Despite successful operation, he unfortunately expired several days later from refractory cardiogenic and septic shock leading to multi-organ failure.
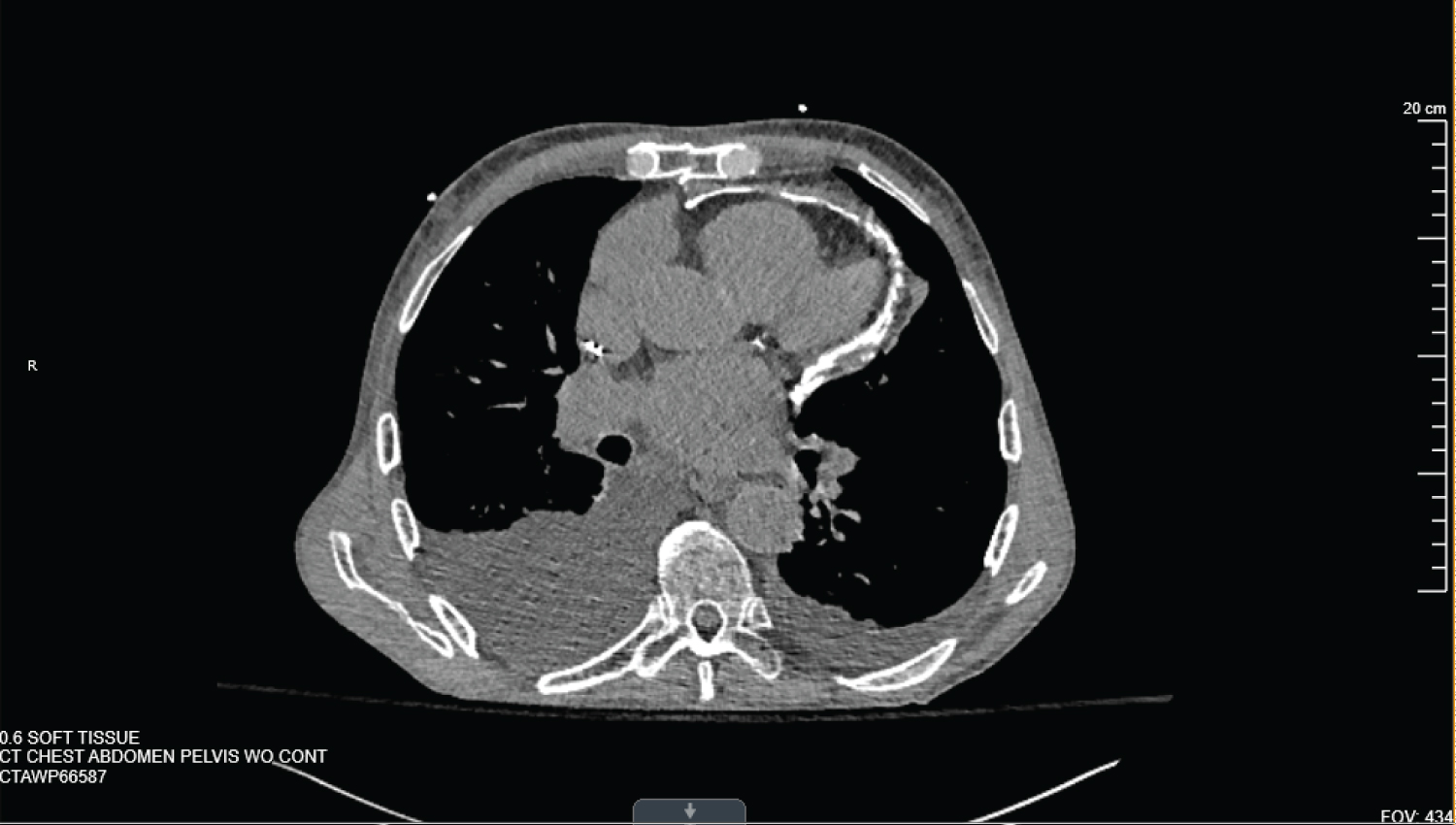 Figure 1: CT scan of the Chest, Axial view. Showing calcified pericardium, along with pleural effusion. View Figure 1
Figure 1: CT scan of the Chest, Axial view. Showing calcified pericardium, along with pleural effusion. View Figure 1
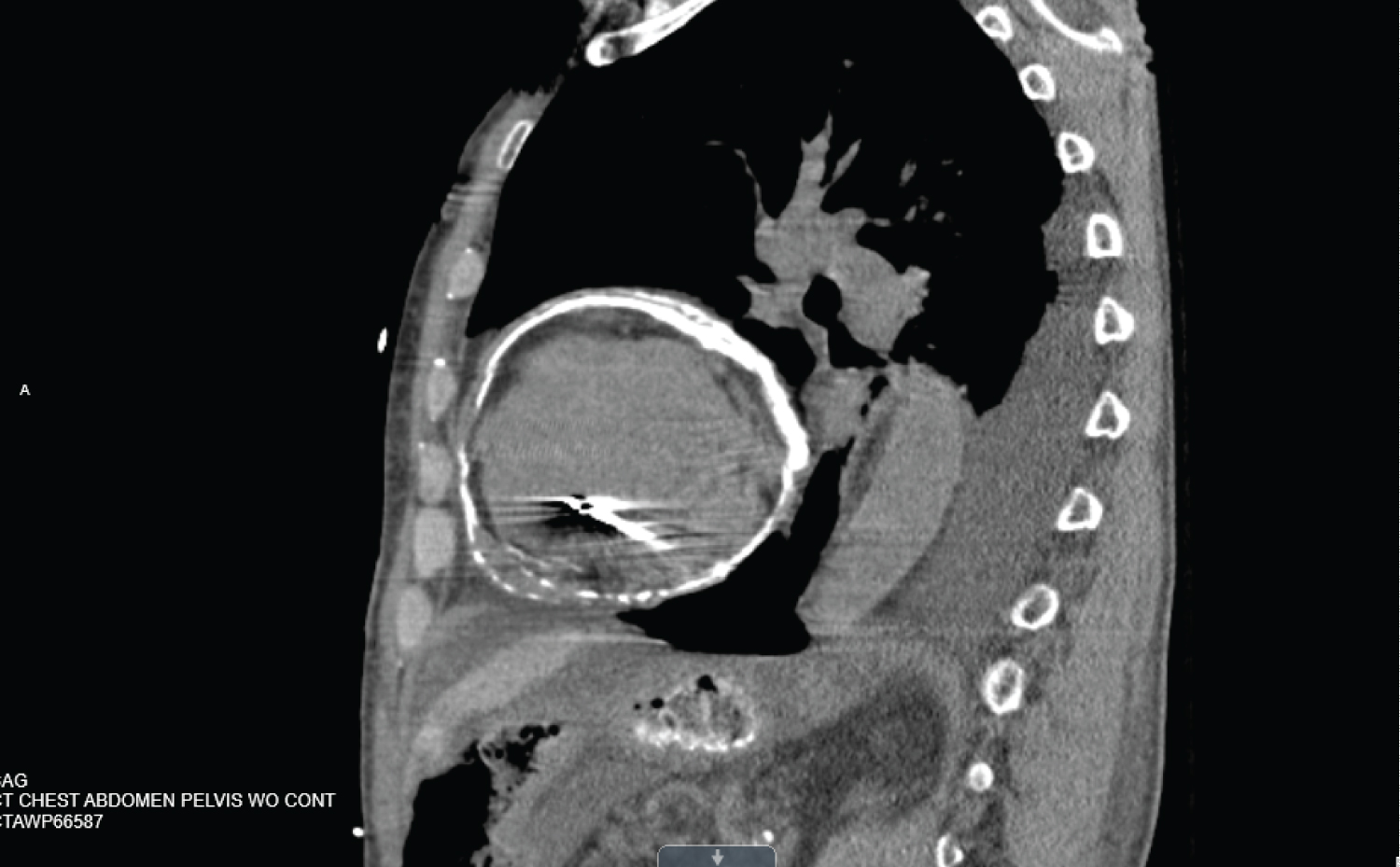 Figure 2: CT scan of the chest showing circumferential pericardial calcification. View Figure 2
Figure 2: CT scan of the chest showing circumferential pericardial calcification. View Figure 2
The pericardium is a thin outer layer of the heart that is comprised of fibrous tissue that anchors, lubricates movement, and prevents overdistention of the cardiac chambers, thereby allowing optimal filling during diastole [1] The pericardium is further subdivided into two separate layers (visceral and parietal layers), which are separated by a potential space (the pericardial space). Under normal conditions, this structure lacks calcification, however, under certain conditions, calcium can be deposited, forming a rigid shell which can compromise cardiac function if it becomes severe [2].
Calcification of the pericardium does not occur in healthy individuals [3]. It is most commonly the result of prolonged inflammation of the pericardium secondary to blunt trauma, previous cardiac surgery, viral or bacterial infection, chronic pericarditis, radiation exposure, or malignancy [1,2,4]. In the developing world, the most common cause of pericardial calcification is believed to be tuberculosis. Evidence for this is found in up to 3% of autopsied cases [5]. Most cases of pericardial calcification are asymptomatic found incidentally on CT imaging of the chest [1]. Unfortunately, as shown in the case of our patient, the sequalae can certainly be life-threatening. Our patient had a notable medical history of atrial fibrillation and severe mitral regurgitation, for which he underwent a cardiac ablation and maze procedure in 2006 along with open mitral valve repair. A maze procedure is when a cardiac surgeon creates small areas of scar tissue in a maze pattern along the atria of the heart to prevent atrial fibrillation. These procedures have been associated with pericardial inflammation and pericarditis [4,5]. In addition, due to recurrent atrial fibrillation, he underwent additional cardiac ablation one year prior to this admission, in 2021. Cardiac ablation carries a known risk factor of post-procedural pericarditis and its implication in the development of constrictive pericarditis has been described in several case studies [1,6-8]. In one study, 10.2% of patients were suspected of having acute pericarditis following atrial fibrillation ablation procedure [1]. In conclusion, prior cardiac surgeries, including mitral valve replacement and maze procedure for atrial fibrillation, along with additional cardiac ablation for recurrent atrial fibrillation resulted in persistent and recurrent inflammation of the pericardium. Subsequent extensive calcium deposition within the pericardium led to constrictive cardiomyopathy, which ultimately resulted in significantly reduced cardiac output and cardiogenic shock.
In conclusion, constrictive cardiomyopathy secondary to pericardial calcification should be considered a differential diagnosis when evaluating a patient with significant risk factors. This includes a history of multiple prior cardiac procedures.
Ethics Approval and Consent to Participate:
Not applicable.
Consent For Publication: Full consent for publication has been obtained from the patient or family. This consent form can be requested if necessary.
Availability of Data and Materials: Data and materials which were collected from the electronic medical record are protected in this case to preserve patient anonymity and per HIPPA guidelines.
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Competing Interests: The authors declare that they have no competing interests.
Funding: No funding was provided for this case report.
Authors' Contributions:
Connor Shaw was a major contributor to reviewing relevant literature, and writing this manuscript.
Vinaya Sermadevi assisted in editing the manuscript.
All authors read and approved the final manuscript.
Not Applicable.
Vinaya Sermadevi, M.D. is a Critical Care Medicine Specialist at Mercy Hospital in St. Louis, Missouri.
Connor S. Shaw, D.O. is a second-year Internal Medicine resident at Mercy Hospital in St. Louis, Missouri.