Mycosis fungoides and its variants account for almost 50% of all cutaneous lymphomas and around 65% of cutaneous T-cell lymphomas. We report the clinical case of a patient with a tumoral nodule, with progressive evolution and rapid transformation. Our patient was undergoing chemotherapy. After mycosis fungoides, CD30+ cutaneous lymphoproliferations are the most frequent pathologies among cutaneous T-cell lymphomas, accounting for 20% of this group.
Mycosis fungoides, Cutaneous lymphomas, Tumoral nodule, Chemotherapy
Primary cutaneous lymphomas are malignant lymphocytic proliferations strictly localized to the skin, without initial extracutaneous extension. They include cutaneous lymphomas such as mycosis fungoides and Sézary syndrome, and other mostly non-epidermotropic lymphomas of T or B lymphocytic origin. Epidermotropic cutaneous T lymphomas of the mycosis fungoides/Sezary syndrome type account for over half of all primary cutaneous lymphomas, ahead of the group of CD30+ cutaneous T lymphoproliferations. Transformation is defined histologically by the presence of more than 25% large cells in the cutaneous infiltrate, and often (but not always) coincides with clinical disease progression and the appearance of tumour lesions or erythroderma. Diagnosis is clinical, confirmed by histology, lymphocyte immunophenotyping and molecular biology.
67-year-old female patient with a history of dysthyroid on Levothyrox. She presented to our department with a tumor-like nodule. The onset was 05 months ago, with the appearance of a small red nodule on the right supraclavicular area, progressively evolving and pruritic. Dermatological examination revealed the presence, in a healthy woman, of an erythematous squamous plaque measuring 07 cm in diameter, centred by a painless 3.5 cm red nodule, on the right supra-clavicular area, and another erythematous squamous plaque measuring 04 cm in diameter, centred by a 1 cm nodule, on the right calf. Biological investigations were carried out, and showed no renal, hepatic or carbohydrate metabolism disturbances. The blood count with smear showed the presence of Sézary cells < 3%. Histological study of a skin biopsy showed cutaneous T lymphoproliferation, and the immunohistochemical profile showed that the dermal and epidermal infiltrate is of T phenotype, strongly expressing CD3 with the presence of epidermotropism in the dermis. There is a higher proportion of CD4+ cells than CD8+ cells. CD30 is expressed only by large cells in the vicinity of the ulceration. Histological study of skin biopsy and immunohistochemistry led to the diagnosis of mycosis fungoides transformed into CD30+ large-cell T lymphoma. The patient was put on chemotherapy after an extension workup, which revealed right axillary lymph node localization on PET scan [1-4] (Figure 1, Figure 2, Figure 3, Figure 4, Figure 5, Figure 6, Figure 7 and Figure 8).
 Figure 1: Erythematous squamous plaque 07 cm in diameter centered by a red budding nodule on the right supra-clavicular area.
View Figure 1
Figure 1: Erythematous squamous plaque 07 cm in diameter centered by a red budding nodule on the right supra-clavicular area.
View Figure 1
 Figure 2: Erythematous squamous plaque measuring 04 cm in diameter, centred by a 1 cm nodule, on the right calf.
View Figure 2
Figure 2: Erythematous squamous plaque measuring 04 cm in diameter, centred by a 1 cm nodule, on the right calf.
View Figure 2
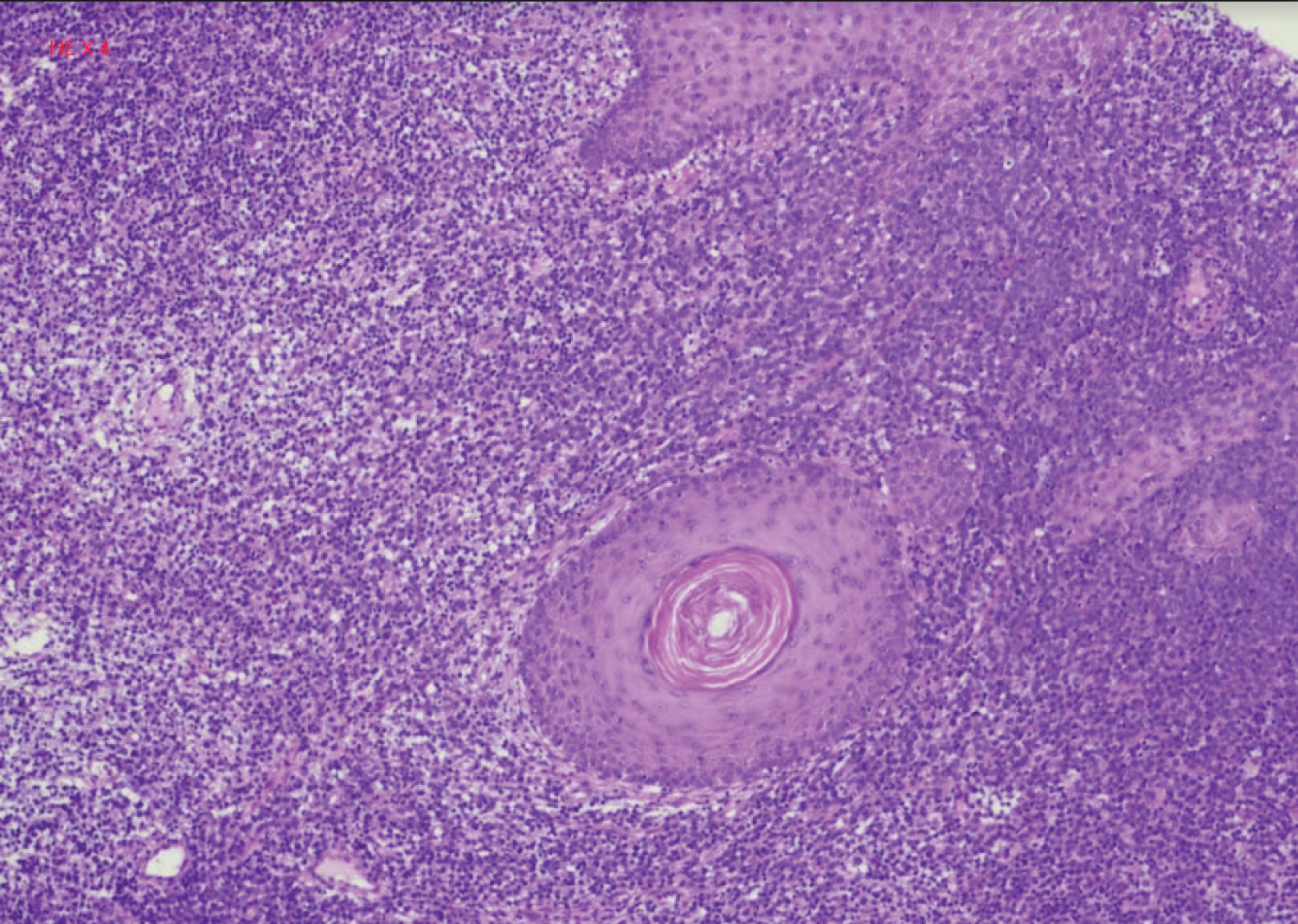 Figure 3: HE x4 cutaneous T lymphoproliferation.
View Figure 3
Figure 3: HE x4 cutaneous T lymphoproliferation.
View Figure 3
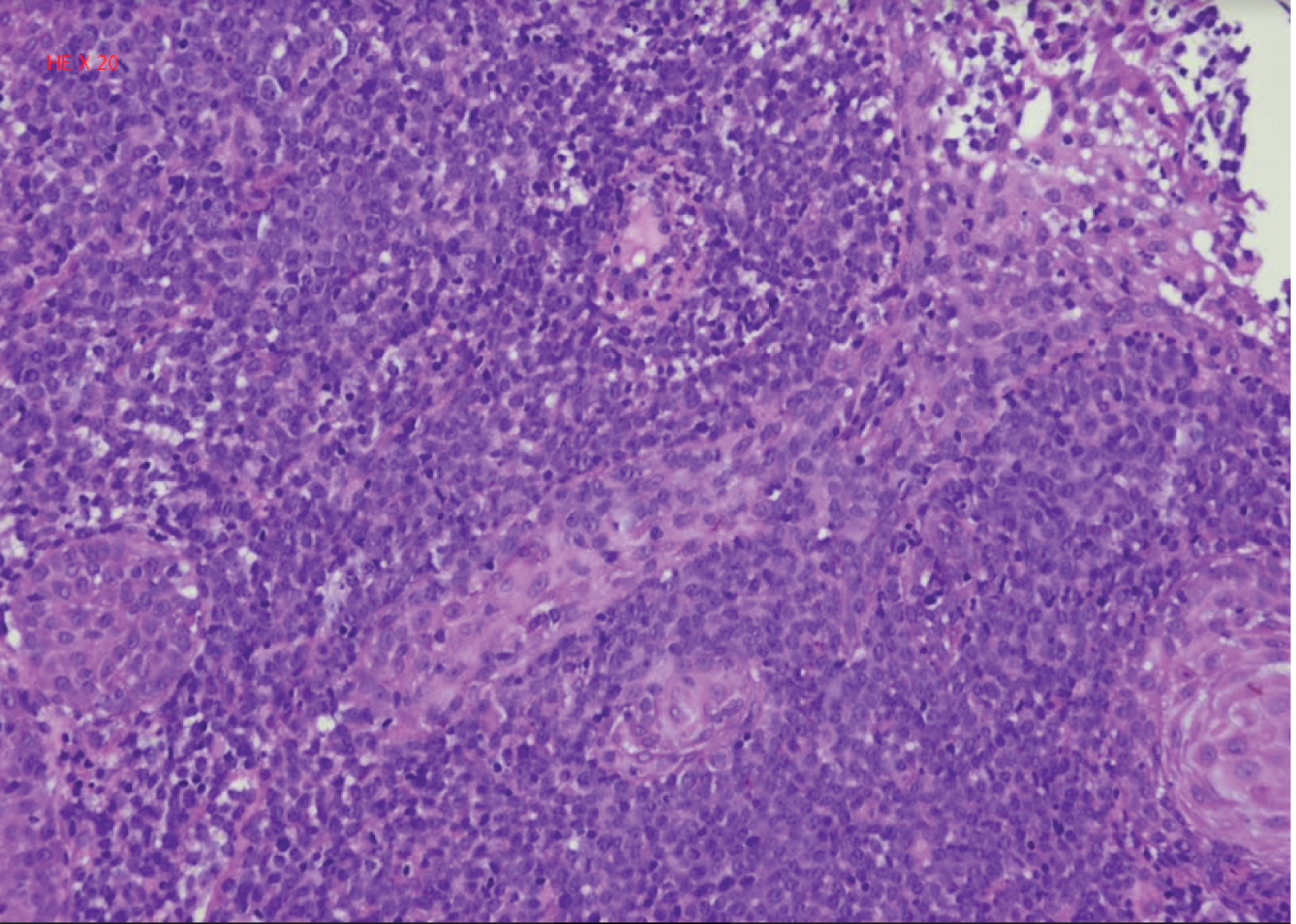 Figure 4: HE x20 cutaneous T lymphoproliferation.
View Figure 4
Figure 4: HE x20 cutaneous T lymphoproliferation.
View Figure 4
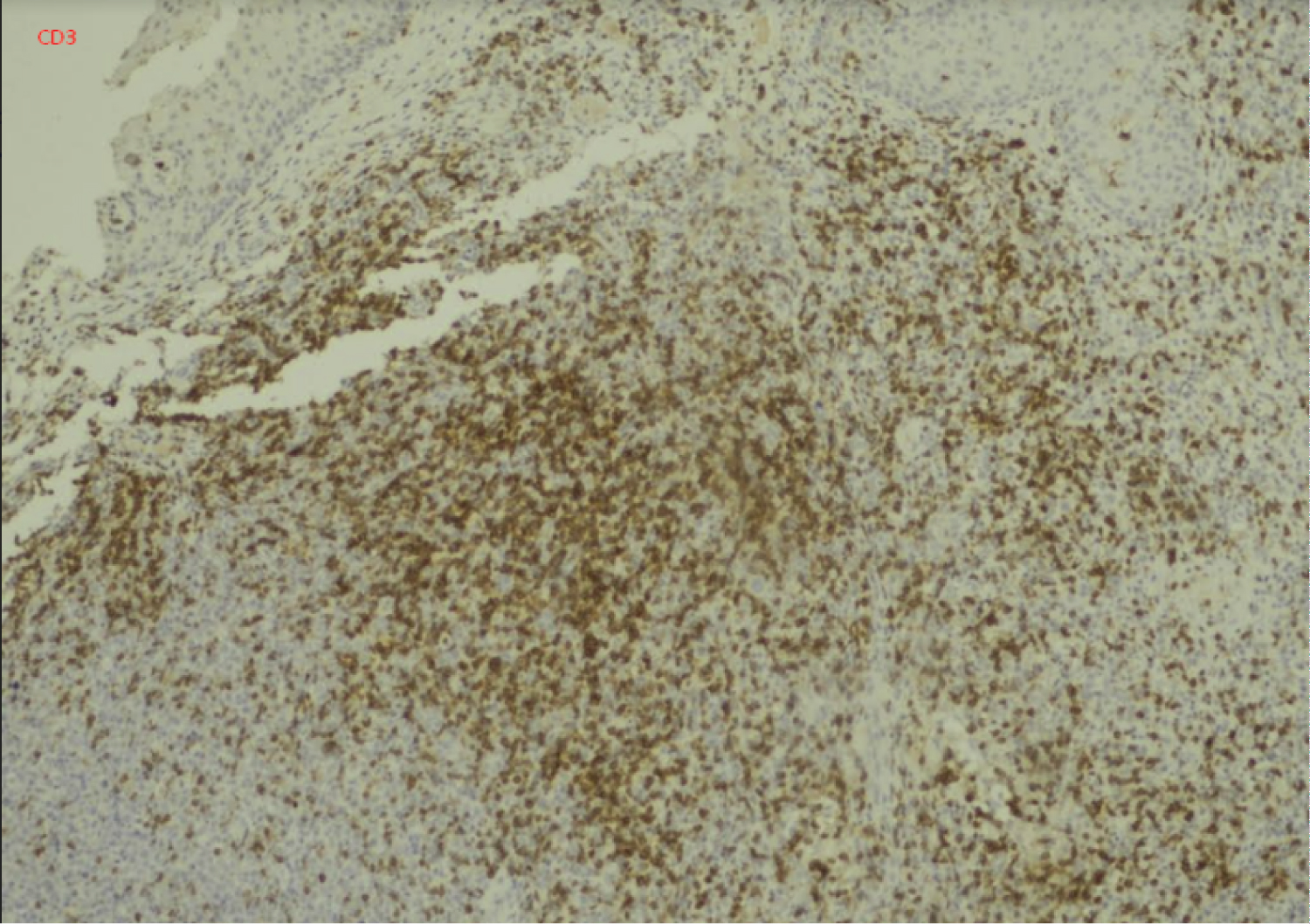 Figure 5: CD3.
View Figure 5
Figure 5: CD3.
View Figure 5
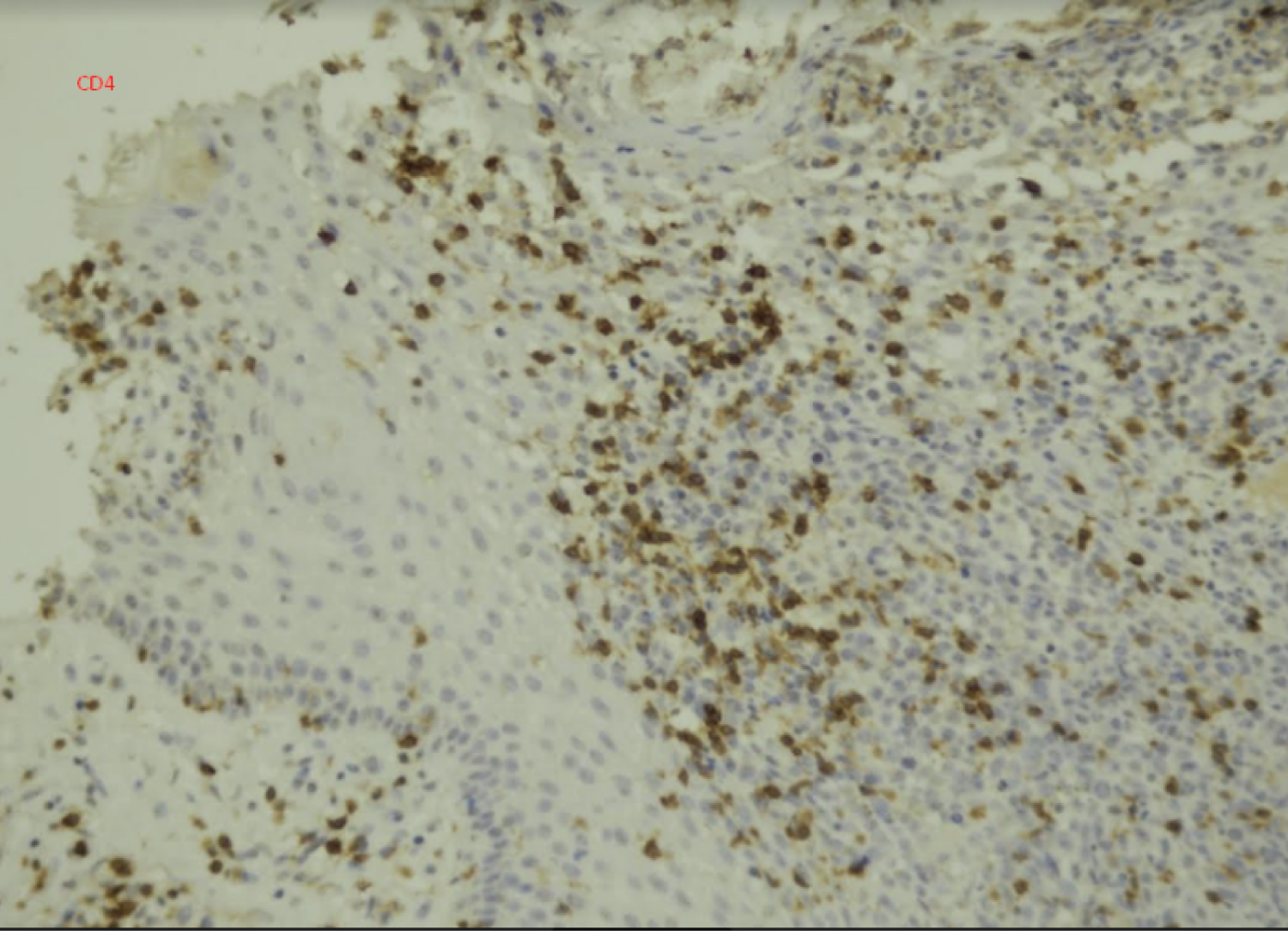 Figure 6: CD4.
View Figure 6
Figure 6: CD4.
View Figure 6
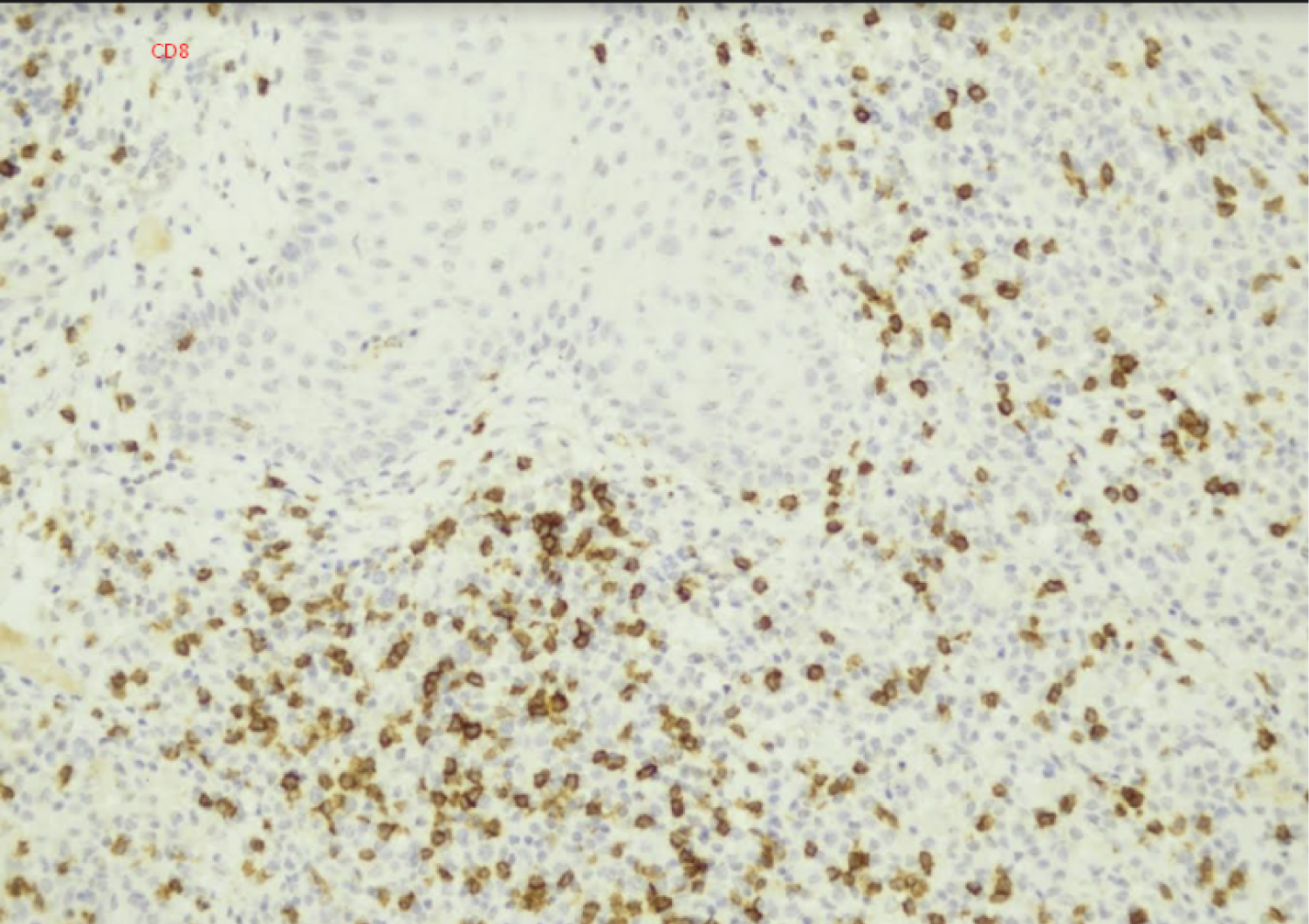 Figure 7: CD8.
View Figure 7
Figure 7: CD8.
View Figure 7
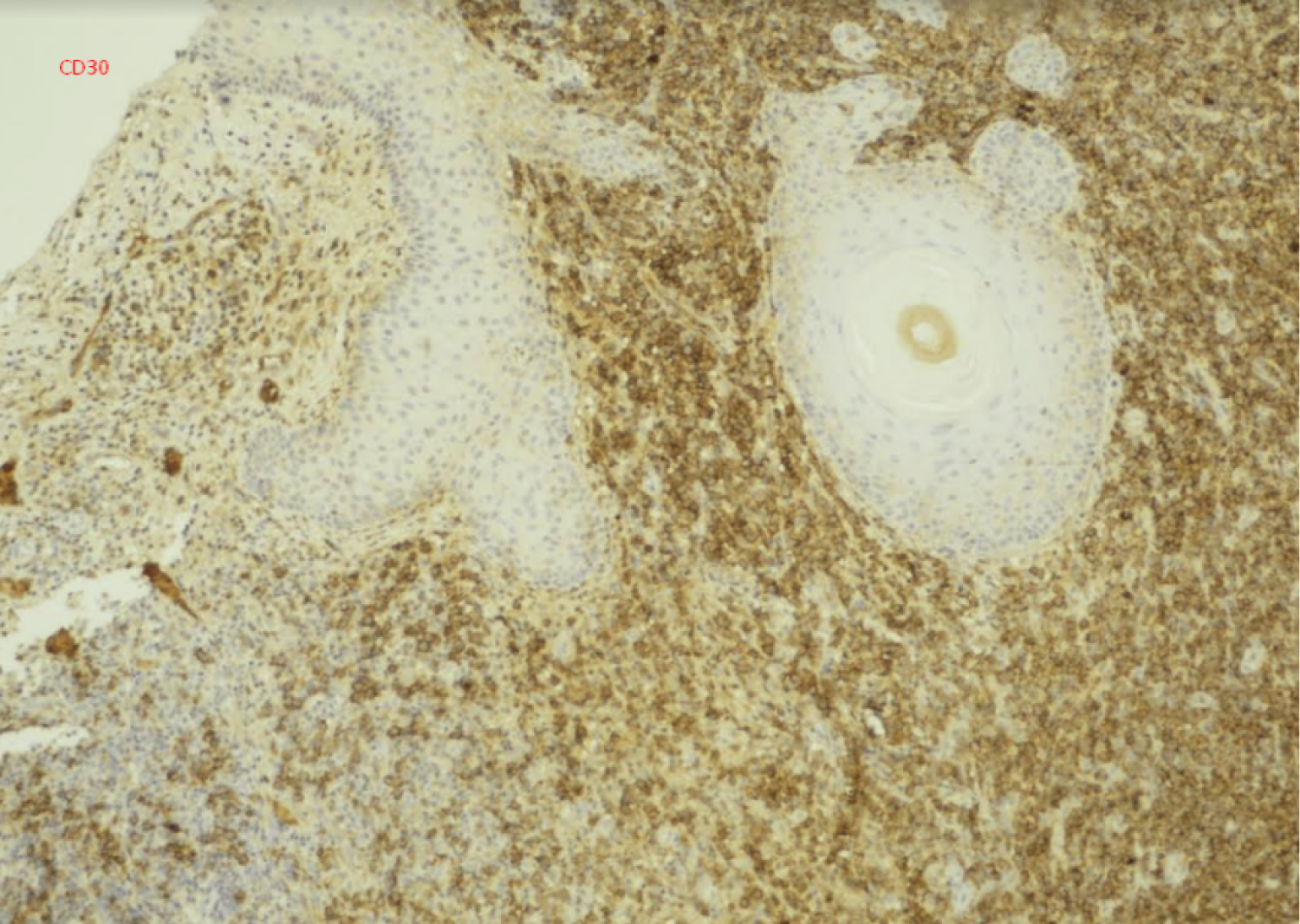 Figure 8: CD30.
View Figure 8
Figure 8: CD30.
View Figure 8
Mycosis fungoides and Sézary syndrome are clearly recognized cutaneous primary T lymphomas and identified within the lymphoma group in the WHO-EORTEC 2019 classification. The diagnosis is clinically evoked in the vast majority of cases, and skin biopsy confirms the diagnosis. The stage of the lymphoma is defined by the TNMB classification to guide treatment and prognosis. Transformation occurs on average five years after the onset of mycosis fungoides, with a median survival of 22 months, indicating a severe worsening of prognosis. This was not the case for our patient, who underwent transformation in less than six months.
The presence of large cells expressing CD30 could be considered a marker of transformation in mycosis fungoides. Nevertheless, they can also be observed in many inflammatory or infectious skin diseases, hence the interest of anatomic-clinical comparisons.