Psoriasis is a chronic, recurrent inflammatory skin disease characterized by abnormal keratinocyte proliferation and vascular hyperplasia. Apatinib is a tyrosine kinase inhibitor which has been reported to be effective in some tumors thought to be associated with inhibition of the proliferation of endothelial cells by selectively inhibiting vascular endothelial growth factor receptor-2 (VEGFR-2). We present a 54-year-old patient with a 30-year history of psoriasis, who did not respond well to oral treatment with acitretin in combination with topical corticosteroids. The patient was diagnosed with rectal cancer and was treated with oral apatinib 250 mg once daily. To our surprise, all the psoriasis lesions were completely resolved after a 53-days course of treatment. Although apatinib and its variants have been extensively used as an anticancer drug, there is no report of their use in psoriasis. As with other antitumor treatments, we speculate that apatinib is effective for psoriasis owing to an inhibition of endothelial cell growth in psoriasis lesions. This observation suggests that apatinib may be a useful drug to treat psoriasis in the future and deserves further investigation in its own right.
Apatinib, Psoriasis, Vascular endothelial growth factor (VEGF), Vascular endothelial growth factor receptor-2 (VEGFR-2)
Apatinib is a tyrosine kinase inhibitor, which has been reported to be effective against some tumors. Its activity against cancer is based upon its antiangiogenic roles by selectively inhibiting vascular endothelial growth factor receptor-2 (VEGFR-2).
Psoriasis is a chronic skin disease characterized by the hyperproliferation of abnormal keratinocytes. In the pathogenesis of psoriasis, activated keratinocytes in lesions produce a number of pro-angiogenic cytokines, including vascular endothelial growth factor (VEGF). The binding between VEGF and VEGFR promotes cell proliferation and angiogenesis [1].
Here, we present a case of patient with rectal carcinoma whose psoriasis lesions were resolved dramatically during treatment with apatinib. We speculate that the remission of psoriasis was also led by VEGFR-2 inhibition of apatinib. With currently available treatment, the clinical response of psoriasis is not always satisfactory. Our case provides a clue that targeted VEGFR-2 by a small molecule inhibitor may be a new therapeutic avenue for psoriasis therapy.
A 54-year-old woman suffering from rectal cancer stage IV presented with severe and chronic psoriasis and underwent an unexpected remission of lesions after treatment with apatinib, an inhibitor of VEGR-2. She began suffering from chronic to have psoriatic plaques about 30 years ago, and the plaques were changed into pustule psoriasis around 10 years ago. One and half years ago she had been treated with oral acitretin 10 mg twice daily for 6 months in combination with topical corticosteroids, which resulted in only partial regression of skin lesions. One year ago, the patient was diagnosed with rectal cancer and stopped taking acitretin and topical corticosteroids; then she underwent surgical treatment, followed with anticancer drugs. She received oxaliplatin 200 mg once in combination with oral capecitabine 1.5 g for 14 days; then 2 months later, she was treated with pulse therapy of 14 d/month with S-1 150 mg twice daily during four months. The treatment with the kinase inhibitor lapatinib (250 mg once daily) was subsequently initiated. At the beginning of treatment with Apatinib, the patient had multiple, large, coalescing erythematosquamous plaques on the upper arms, abdomen, back, and lower legs, covering approximately 10% of the body surface area. There was no nail or joint involvement. After 13-days treatment with apatinib, the skin condition improved satisfactorily (Figure 1); 53-days after starting apatinib, almost all psoriatic plaques had regressed completely, with only a few erythematous papules remaining on the upper arms. During treatment with apatinib, the patient stopped receiving acitretin and topical corticosteroids. The patient was followed up for one month without recurrence of skin lesions.
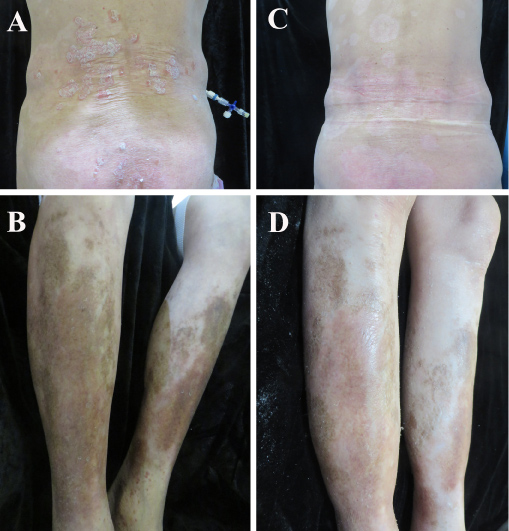 Figure 1: Three days after treatment with apatinib. View Figure 1
Figure 1: Three days after treatment with apatinib. View Figure 1
Aberrant keratin expression in psoriasis plays a crucial role in keratinocyte dysfunction and disease development. In patients with psoriasis, pro-angiogenic cytokines (VEGFRs) are significantly elevated in keratinocytes, which suggests that the keratin dysregulation may be due to these VEGFs. The effectiveness of VEGFR inhibitors on psoriasis have been previously reported with sorafenib, an inhibitor of multiple kinase including VEGFR, which could effectively treat psoriasis lesions [2-4]. In another study, two patients were reported to have clearance of psoriasis skin lesion after treatment with anti-VEGF antibody bevacizumab [5]. In addition, the psoriatic lesions were dramatically resolved in two patients (one patient with renal cell carcinoma, another patient with metastatic renal carcinoma) during treatment with sunitinib, an inhibitor of VEGFR-2 [6-8]. These case reports suggested that targeted inhibition of VEGFR or/and VEGF may be a new therapeutic avenue for psoriasis therapy.
Acitretin is a second-generation retinoid. It is taken orally and is typically used for psoriasis. After six months of daily treatment with 30 mg of acitretin, the plasma steady-state concentration of acitretin was 85.5 ng/mL with an elimination half-life of 47.1 hours (about 2 days) [9]. If etretinate was not formed, 98% of acitretin would be completely removed within two months. Topical glucocorticoids are used alone or in combination with other drugs to treat psoriasis. The washout time of glucocorticoids range from 2 days to 4 weeks. In our patient, the patient had stopped taking acitretin and topical corticosteroids for more than one year before he was treated with apatinib. The post-treatment of both two drugs on psoriasis were excluded. The link between antiangiogenic drugs and keratinocyte proliferation in psoriasis has been tested in Kuang, et al. study, in which they found that topical sunitinib ointment alleviates psoriasis-like inflammation by inhibiting the proliferation and apoptosis of keratinocytes [6]. We assume that inhibition of VEGFR-2, and possibly other kinases, is responsible for apatinib's therapeutic efficacy.
While some researchers assumed that inhibition of EGFR, VEGF or VEGFR would represent a new therapeutic approach for psoriasis [10], some disagreements occurred.
Two patients treated with sorafenib who had no history of psoriasis developed a psoriasis-like eruption [11,12]. In one patient with chronic plaque psoriasis, a pustular eruption appeared during treatment with sorafenib even through the authors explained it as a possibly a pustular drug reaction [13]. Therefore, the beneficial effects of VEGF, VEGFR and EGFR inhibition on psoriasis need to be clarified with a larger number of the case studies before the introduction of apatinib, sorafenib, vemurafenib, and/or other tyrosine kinase inhibitors as a new therapeutic approach to psoriasis.
The authors have no conflict of interests in connection with this study.
This work was supported by grants from the national natural science foundation of China (NM. 81773337 and 81401653) and funded by the Shandong Traditional Chinese Medicine Science and Technology Development Plans, China (NM) 2017-415), the Medical and Health Science Technology Project of Shandong Province, China (NM 2017WS345), and the Natural Science Foundation of Shandong Province, China (NM. ZR2015HL127).