Toxic epidermal necrolysis (TEN) is a life-threatening drug reaction that requires immediate medical treatment. Mortality due to TEN cases is quite high until now and the main cause reported is multiple organ dysfunction syndrome. A 7-year-old child, was diagnosed TEN with 86% blistered skin, after receiving Metampiron. Given 20% albumin 50 ml from the first day treated until 20 days, also fluid resucitation, steroids, antibiotics, vitamin C, neurobion, paracetamol, antihistamines, oral hygiene, steroid and antibiotic ointment for body, eye ointment, woundcare, and high nutritions.
The other case, 33-year-old woman, was diagnosed TEN with 100% blister skin, due to Phenytoin. Given 25% albumin 100 ml from the first day to 20 days. Both patients recover without complications. In TEN, hypoalbumin often occurs due to eroded skin. Hypoalbumin can reduce organ function and drug effectiveness. Drugs that are usually bound to protein become free in plasma and metabolism in hepatic become more rapid. Immidiate albumin therapy can prevent this and reduce patient mortality. The albumin also plays a role to accelerate skin regeneration.
Immediate albumin therapy, Mortality, TEN
TEN (Toxic Epidermal Necrolysis) is an acute life-threatening drug reaction and is characterized by involvement of the mucous membrane and skin, where extensive necrosis can occur and erode the epidermis layer [1-3]. Most causes of this disease are due to drugs. This disease is a rare case, there are about 5-6 cases per year with a high mortality rate around more than 50% [1]. Severe TEN cases can be accompanied by systemic complications resulting in organ failure and death [3]. Herrmann, et al. [4] reported that increased length of stay and mortality at hospital associated with low albumin levels obtained within 48 hours of admission, because albumin levels may decrease early in severe illness and even lower after 48 hours admission [4]. Albumin can maintain organ function, increase drug effectiveness, reduce mortality and accelerate skin regeneration [5-7].
A 7-year-old girl, with the complaints of appearing red spots all over the body, blistered mouth, peeled, fever, red eyes, and itching for one day after took a mixed drug of paracetamol, methampiron, cold and cough medicine. This complaint was felt for the first time. History of systemic disease, drugs or food allergy is denied. She had a complete immunization history.
In generalized status, the patient was compos mentis and looked seriously ill. Weight about 34 pounds. Vital signs, pulse 175 times a minute, breathing 30 times a minute, and temperature 39.1 ℃. Normal physical examination. Dermatological status, facial, anterior and posterior thorax, abdominal, bilateral brachial, bilateral antebracial, perineum, bilateral femoral, there are erythematous macules, well-defined, multiple numular-plaque sizes, and also bullae, purpura, erosion, and epidermolysis; orbital: bilateral conjunctival hyperemia; labium oris: Erosion and black crust; genital: Erosion (total 86% blistered skin). Laboratory tests show, hemoglobin 14.2 g/dL, leukocytes 10.400/uL, platelets 403.000/mm3, Albumin 3.6 g/dL, ureum 48 mg/dL, creatinine 0.7 mg/dL, sodium 133 mEq/L, potassium 4.6 mEq/L, chloride 101 mEq/L.
Albumin 20% intravenous 50 ml once a day for twenty days was given, as well as Ringer's Lactate solution 1500 cc in 24 hours, systemic drugs such as Metylpredisolone 62.5 mg twice a day, Gentamicin 60 mg once a day, Amikacin 250 mg once a day, Vitamin C 500 mg, Neurobion, Paracetamol 175 mg, Loratadine 5 mg twice a day. For lips, Mometason ointment and Kenalog®, Kloderma 50 grams + Mupirocin ointment 50 grams for body area, and Cendo Xitrol® eye ointment. Also closed gauze wounds, aspirated bullae, and given high calories and high proteins nutrition.
The other case, a 49-year-old woman, with complaints of full body blisters for 5 days, arose suddenly after taking phenytoin drug. This complaint was felt for the first time. History of systemic disease, drugs or food allergy is denied. She got the drug when she was first diagnosed with epilepsy three weeks ago.
The patient was compos mentis and looked seriously ill. Vital signs, tension 110/70 mmHg, pulse 88 times a minute, breathing 20 times a minute, and temperature 38.1 ℃. Normal physical examination. Dermatological status, facial, anterior and posterior thorax, abdominal, bilateral brachial, bilateral antebracial, perineum, bilateral femoralis, bilateral cruris, there are erythematous macules, well-demarcated, multiple numular-plaque, and also bullae, purpura, erosion, crust, and epidermolysis; orbital: bilateral conjunctival hyperemia; labium oris: erosion and black crust; genital: erosion (total 86% blistered skin). Laboratory tests show, hemoglobin 12.8 g/dL, leukocytes 8.100/uL, platelets 237.000/mm3, Albumin 2.2 g/dL, ureum 25 mg/dL, creatinine 1.0 mg/dL, sodium 127 mEq/L, potassium 4.6 mEq/L, chloride 91 mEq/L.
Patient was treated with Albumin 25% intravenous 100 ml once a day for twenty days, as well as Ringer's Acetat solution 2000 cc in 24 hours, systemic drug such as Metylprednisolone 125 mg twice a day, Ceftriaxone 2 gr once a day, Gentamicin 80 mg once a day, Vitamin C 500 mg, Neurobion, Paracetamol, oral medication Loratadine 10 mg twice a day, Tantum Verde® for mouth rinses, Kloderma® 50 grams + Mupirocin ointment 50 grams for body area. For eye, and Cendo Xitrol® eye ointment. Also closed gauze wounds, aspirated bullae, and given high calories and high proteins nutrition.
Both patients recovered without complications and were discharged from the hospital (Figure 1, Figure 2, Figure 3, Figure 4, Figure 5 and Figure 6).
 Figure 1: Early treatment period.
View Figure 1
Figure 1: Early treatment period.
View Figure 1
 Figure 2: Skin and mucosal conditions in healing phase.
View Figure 2
Figure 2: Skin and mucosal conditions in healing phase.
View Figure 2
 Figure 3: Patient condition after 1 week discharge from the hospital.
View Figure 3
Figure 3: Patient condition after 1 week discharge from the hospital.
View Figure 3
 Figure 4: Early treatment period.
View Figure 4
Figure 4: Early treatment period.
View Figure 4
 Figure 5: Skin and mucosal conditions in healing phase.
View Figure 5
Figure 5: Skin and mucosal conditions in healing phase.
View Figure 5
 Figure 6: Patient condition after 1 week discharge from the hospital.
View Figure 6
Figure 6: Patient condition after 1 week discharge from the hospital.
View Figure 6
TEN is characterized by eroded epidermis skin and mucositis [1,2]. The cause of TEN in both cases due to drugs is based on a history of previous drug consumption and after the drug stop, the skin lesions begin to heal.
The massive loss of fluid, albumin, and protein can occur in extensive skin loss, besides the open dermis skin layer will release serum so that it bleeds easily, leakage of albumin happens, and easily get infected [2,3,8]. Various complications can occur in TEN such as dehydration, sepsis, pneumonia, and also multiorgan dysfunction such as ulceration and gastrointestinal perforation, acute renal failure, thromboembolism, and DIC (Disseminated Intravascular Coagulopathy) [3,9,10]. In both of these patients fluid, albumin and protein loss occurred. In the case of children, albumin at admission is 3.6 mg/dL, but after treatment albumin levels tend to fluctuate, until the lowest albumin level obtained 2.4 mg/dL on day-14 of treatment. In adult case, albumin at admission is 2.2 mg/dL, during treatment albumin levels also tend to fluctuate, but have never been found lower than initial results. In this patient, complete skin healing occurs at 3 weeks after treatment. When healed, the hypo- and hyperpigmented parts of skin are visible Graphic 1.
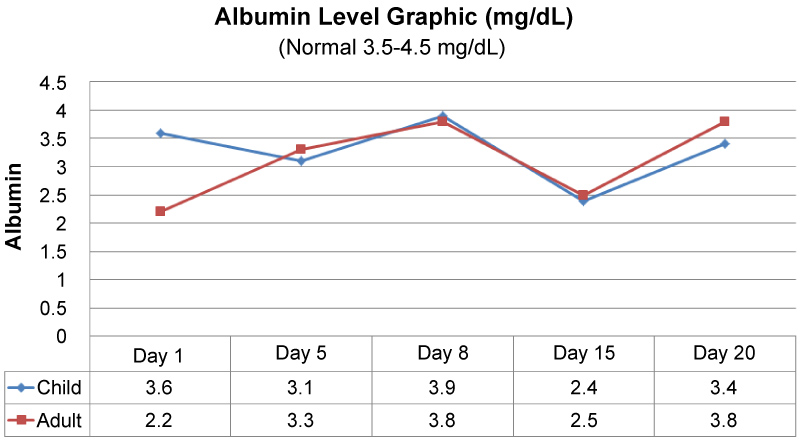 Graphic 1: Albumin level progress.
View Graphic 1
Graphic 1: Albumin level progress.
View Graphic 1
There are not many journals that discuss the importance of using intravenous albumin in patients with NET, maybe because of the albumin level are seen to be normal at early hospital admission. Albumin is the largest plasma protein and is synthesized in the liver. Albumin production is inhibited by proinflammatory mediators namely interleukin-1 (IL-1), interleukin-6 (IL-6), and TNF (Tumor Necrosis Factor). Albumin is important to maintain oncotic pressure (80%) which can prevent vascular leakage from intracellular to extracellular where it can be at risk of edema [5,11]. Albumin also functions to transport various substances, namely fatty acids, metals, hormones, iron, bilirubin, and drugs medicine. When hypoalbumin occurs, drugs that bind to proteins become free circulating in the blood, so the levels of drugs in the blood increase and increase hepatic metabolism [11].
Hypoalbumin often occurs in critical patients, in care, and elderly, which may occur due to decreased production and/or lost through the kidneys, skin, gastrointestinal, or increased catabolism or extravascular. [5] Amit Akirov, et al. [6], states that administration of albumin can increase life up to 34%, compared to administration of crystalloid fluids alone. Albumin also prevents acute kidney injury (AKI), hypotension, and general edema [5,7]. Albumin also plays a role in accelerating wound healing [12]. In both patients 20% (child) or 25% (adult) albumin was applied, once a day from the first day to 20 days of treatment. Although initial albumin levels are still within normal limits, this is to avoid albumin leakage that occurs within a few days due to epidermolysis. Albumin can also make the performance of the drugs given work better and speed up the recovery and healing of patient's wounds. Moreover, it can reduce the excessive use of crystalloid fluids and also prevent acute kidney damage due to dehydration. As a result both patients recovered without complications.
Two cases of toxic epidemal necrolysis in 7-year-old children and 49-year-old women have been reported. Diagnosis is based on anamnesia, physical examination and laboratorium examination. Giving albumin for 20 days from the beginning of treatment can maintain organ function, increase drug effectiveness, reduce mortality and accelerate skin regeneration.