Pilotropic mycosis fungoid (PMF) is a rare variant of mycosis fungoides (MF) with distinctive clinicopathological features, accounting for 1 to 5%. It is characterized by a broad spectrum of clinical features and has a more aggressive clinical course than conventional MF [1]. At the onset of its progression, pilotropic mycosis fongoides is sometimes difficult to distinguish from classical mycosis fongoides with follicular involvement. PMF diagnosis is challenging and can mimick other conditions. Dermoscopy can be a valuable clue for the clinical diagnosis and differentiation with other inflammatory conditions. We report a case of follicutropic mycosis fungoid followed up in our department, with its dermoscopic findings, masquerading as chronic eczema.
A 38-year-old patient, working as a poultry farmer, with no relevant medical history, presented to our department with a 5 year history of erythematous plaques located on the head and scalp treated as chronic eczema with topical corticosteroid with good improvement.
Clinical examination revealed the presence of erythematous plaques on the head and scalp, follicular papules on the trunk and the presence of a tumor firm well circumscribed with a size of 7 × 5 cm located on the occipital region.
Dermoscopy showed white and hyperpigmented halo around the follicle, broken hairs, orange pink perifollicular clods and anisotrichia.
The patient was also complaining of chronic pruritus, recurrent abcesses, and folliculitis in the lower limbs over the past 2 years. There was no alopecia and no lymph nodes were found.
A biopsy was performed, showing a lymphocytic infiltrate with perifollicular accentuation. The immunohistochemical analysis was positive for CD3, CD5 and negative for CD7.
The diagnosis of pilotropic mycosis fungoid without mucinosis was made.
Investigations carried out including full blood count, chest X-ray, CT scan, renal and liver function tests were normal. Viral screens for HIV, hepatitis B and C antibodies were also negative. He was diagnosed as early stage disease (stage IIB).
The patient received methotrexate 25 mg per week with good evolution (Figure 1 and Figure 2).
 Figure 1: Erythematous plaques located on the face and occipital area.
View Figure 1
Figure 1: Erythematous plaques located on the face and occipital area.
View Figure 1
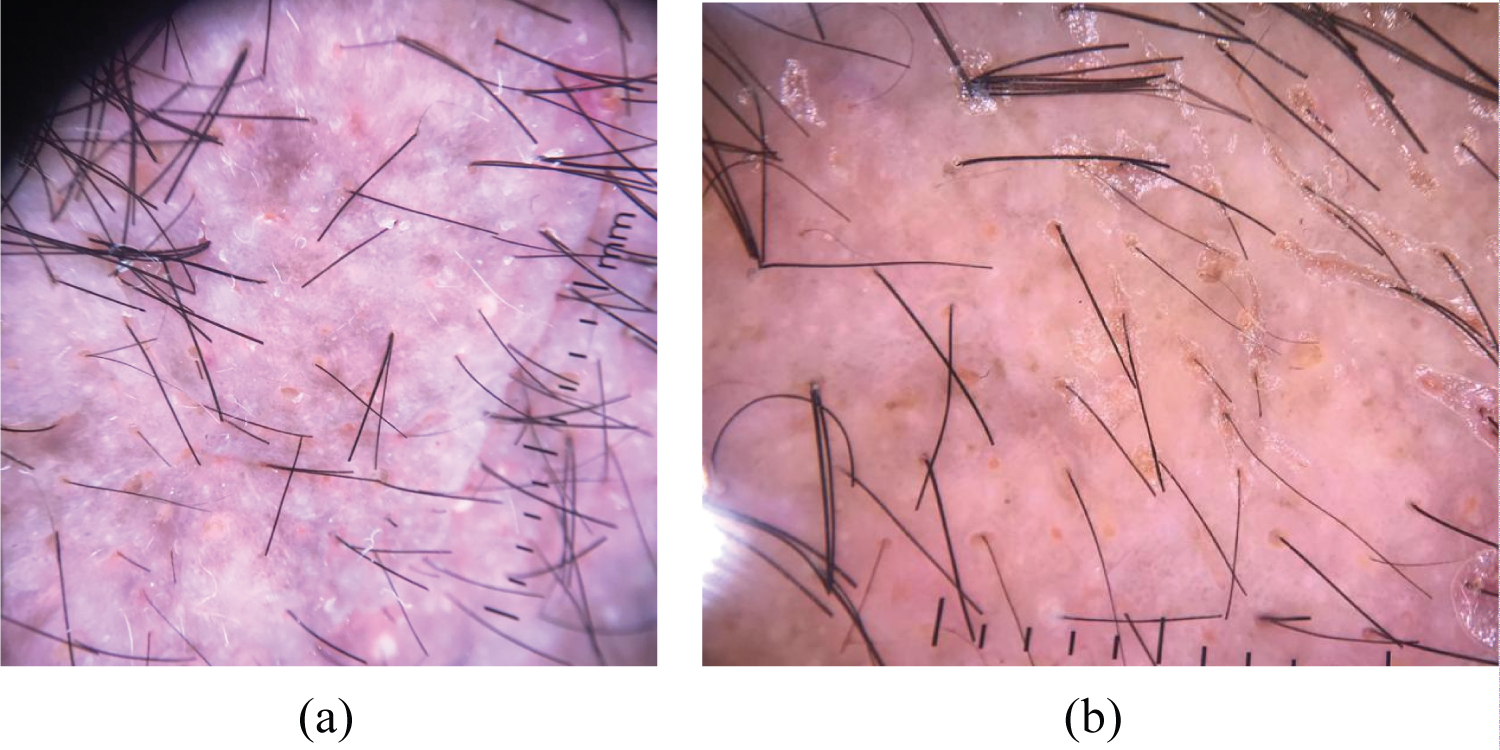 Figure 2: Dermoscopy showed white and hyperpigmented structures (a) with orange halo around the follicle.
View Figure 2
Figure 2: Dermoscopy showed white and hyperpigmented structures (a) with orange halo around the follicle.
View Figure 2
Mycosis fungoid occurred in adulthood; the mean age of onset varies from 46 to 59 years with a male preponderance [1].
The most common clinical findings associated with FMF are patches, plaques, and tumors mainly located on the head and neck as presented in our patient and it rarely affects the tunk and extremities. In adults, pruritus is a common symptom that is often difficult to manage. Comedonal, acneiform, cystic lesions and prurigolike lesions can also be present at the early stage of the disease. FMF lesions can mimic infectious and non-infectious disorders (acne vulgaris, keratosis pilaris) [2-4]. Involvement of the eyebrows with alopecia is also highly characteristic and may present at an early disease manifestation, mimicking alopecia areata [2-6].
Dermoscopic patterns of MF and its variants have been described in a few studies. The dermoscopic features found in patients with FMF are: Perifollicular accentuation seen as a white halo around the follicle, comedo-like openings, white structureless areas, and dotted/fine linear vessels. Milky-white globules and black dots/broken hairs, as well as keratotic cone-shaped spicules, were also reported [7,8]. In our patient, the perifollicular accentuation was suggestive of perifollicular invasion. We performed a biopsy guided by dermoscopy and confirmed the diagnosis of FMF.
Clues to the histopathological diagnosis consisted of a lymphocytic infiltrate with perifollicular accentuation. The interfollicular epidermis is frequently spared. Pautrier's microabscesses are rarely seen. Immunochemistry stained for CD2 and CD3. Antigen loss (for example CD2, CD3, CD4) has been described and may be useful for further diagnostic differentiation. Isolated cases of CD8-positive FMF have also been reported. In addition, there may be variable expression of CD30, which is associated with large-cell transformation in some cases [9,10].
Recent studies distinguished indolent (early-stage FMF) and more aggressive (advanced stage FMP) subgroups. Clinically, patients with early-stage skin-limited FMF present with localized or follicular papules often associated with hair loss, keratosis pilaris-like and acneiform lesions or plaques with histollogically peri and intrafollicular infiltrates. The prognosis is excellent in this group with a 5-year OS of 92-94%. The treatment is based on potent topical steroid, imiquimod in case of limited follicle-based patches (T1), PUVA therapy is indicated in patients with plaques and patches [11].
In patients with advanced stage FMP with widespread thick plaques and/or tumours, prognosis is worse than epidermotropic variants. The treatment should combine a systemic and skin directed therapy. Several options may be considered: PUVA therapy combined with local radiotherapy for most infiltrated lesions and PUVA therapy combined with IFN-a or retinoids (Isotretinoine or bexarotene). In patients with widespread skin lesions we often prefer PUVA with additional low-dose radiotherapy for thick plaques or tumours [11].
Folliculotropic mycosis fungoides is considered as a rare variant of mycosis fungoides with a bad response to therapy and severe prognosis. Physicians should be aware of this 'great imitator' which can mimic inflammatory and infectious disorders. Dermoscopy can be a tool in the diagnosis. A biopsy guided by the dermoscopy should be performed to confirm the diagnosis at an early stage when a FMF is suspected.