Background: Cartiva® Synthetic Cartilage Implant (SCI) was introduced in our department in 2016 as an alternative treatment for advanced degenerative disease of the hallux metatarsophalangeal joint requiring fusion but would rather prefer to maintain joint movement.
Method: A prospective audit was commenced to monitor clinical results limiting selection criteria to young patients with advanced disease with no hallux deformity and no inflammatory arthritis. Outcome measures include patient-reported outcome using the Manchester-Oxford Foot Questionnaire and total range of movement.
Results: Between 2016 and 2019, we performed Cartiva® SCI in 19 toes in 16 patients. Thirteen toes were grade 4 and 6 were grade 3. Outcome data were collected at 3, 6, 12 and 24 months. We have complete follow-up data for 19 of 19 cases at 3 and 6 months, 14 of 19 at 1 year and 7 of 19 at 24 months.
Results show significant improvement in MOx-FQ scores compared to preoperative scores with peak improvement at 6 months, followed by slight decline but stayed significantly better compared to preoperative scores. This was observed in all components of the MOx-FQ except for social interaction which showed continuous improvement up to 2 years.
The total range of movement showed steady improvement from mean preoperative baseline of 31 degrees to 55 degrees at 3 months (p=< 0.001), 63 degrees at 6 moths(p=< 0.00), 59 degrees at 12 months (p=< 0.003) and 80 degrees at 24 months (p=< 0.043).
Two patient required further procedures for continuing pain and stiffness. One was converted to fusion after 2 years. One patient had manipulation and steroid injection.
One patient developed a "squeegee" sensation when walking and moving the toe which spontaneously resolved after 6 months.
Conclusion: Our results indicate good short-term result in 17 of 19 patients with Cartiva® SCI based on patient-reported outcome and total range of joint movement.
Cartiva; Hallux rigidus; PROM; MOx-Fq; Interposition arthroplasty
Hallux rigidus is a common degenerative condition which affects approximately 2.5% of patients over 50 years. It is a progressive disorder and is associated with pain and loss of joint movement.
Management is dependent on severity of clinical symptoms and radiographic appearance. In advanced stages, operative management becomes necessary for pain relief. Fusion of the joint remains the most popular operative option. It is reliable in relieving pain but requires sacrifice of joint movement which is not acceptable for many patients.
Historical operative options have included resection arthroplasty [1] and Moberg osteotomy [2]. In recent decades, joint replacement type surgeries have been developed with varying results. These include Moje joint replacement [3], Townley metallic hemiarthoplasty [4], hemiCAP® hemiarthroplasty [5] and silicon replacement [6].
The Cartiva® Synthetic Cartilage Implant (SCI) is promoted as a joint preserving alternative to fusion and is equally effective in relieving pain [7]. SCI comprises an organic hydrogel polymer composed of polyvinyl alcohol and saline. It has a high-water content, and its elastic and compressive mechanical properties are similar to articular cartilage. It is a cylindrical implant and is placed into the metatarsal head via press-fit implantation [8].
The operative technique is simple, requires minimal instrumentation and leads to minimal bone loss and thus, postoperative recovery is faster than fusion [8]. Owing to the minimal bone loss during the primary procedure, salvaging a failed SCI with fusion has been shown to produce similar outcomes to primary arthrodesis [9].
Results from other series show positive midterm results. SCI has demonstrated high survivorship at two [8] and five years [10] and has produced similar pain relief and functional outcomes to fusion with a preserved range of motion [10,11]. However, there remains a paucity of studies evaluating SCI with most publications in the field derived from a single randomised controlled trial [8].
We introduced Cartiva® Synthetic Cartilage Implant (SCI) in our department in 2016, hence a mandatory audit was undertaken as a requirement for clinical governance when introducing a new procedure.
This study aims to assess the clinical outcome of patients with advanced hallux metatarso-phalangeal joint osteoarthritis treated with Cartiva® Synthetic Cartilage Implant based on patient-reported outcomes measure scores and total range of motion of the joint.
Data were prospectively recorded for all patients who underwent SCI for advanced hallux MTPJ arthritis performed by a single surgeon at a district general hospital from 2016 to 2019. The procedure was selectively offered to young patients with advanced disease which required fusion but would rather preserve joint movement. Patients with significant hallux deformity and inflammatory arthritis were not offered this treatment.
Disease severity was assessed clinically and radiographically by the senior author and classified using the Coughlin and Shurnas (C&S) grading system.
The primary outcome was Manchester-Oxford foot questionnaire (MOx-FQ) score. The MOx-FQ is a validated patient reported questionnaire which assesses outcomes following foot and ankle corrective surgery [12]. It comprises 16 items which examine three domains: walking/standing; pain; and social interaction. Each section is scored from 0 to 4 indicating increasing severity. Scores are summed generating total scores for each domain and for the entire questionnaire. Total scores are then converted to metric scores for increased sensitivity, as per user instructions.
Secondary outcome was range of motion (ROM) of the hallux. This was assessed by the senior author using a handheld goniometer. Dorsiflexion was assigned a (+) value, and plantar flexion a (-) value. Range of movement was calculated as the difference between dorsiflexion and plantarflexion.
Outcome data were recorded preoperatively, and then at three, six, 12 and 24 months postoperatively.
The procedure was performed under general or spinal anaesthetic with patient supine. Prophylactic antibiotics were given, and a thigh tourniquet was used. The metatarsophalangeal joint was approached dorsally. The extensor hallucis tendon was retracted and peripheral osteophytes were removed. The collateral ligaments were preserved.
The SCI kit comes with a metallic placer, a 2-mm guidewire, a cannulated reamer, and an introducer. The placer is either 8- or 10-mm diameter and corresponds to the size of the implant chosen. The 10mm implant was used in all cases in this series.
The placer was used to guide wire insertion ensuring perpendicular placement to the joint surface. The wire was applied centrally but adjusted to cover for the worn area with at least 2 mm margin of bone around the rim. Reaming over the guidewire was done to create the cavity in the metatarsal head making sure not to rim all the way but leave a 2 mm gap between the surface and reamer stopper.
The implant was inserted and pressed into the cavity using the introducer leaving it 2 mm proud. The joint was reduced and smooth gliding over of the surfaces was confirmed.
The capsule was repaired without tension with a no. 2.0 Vicryl suture, and the skin was closed using interrupted nylon sutures. Wound dressing was applied, and the foot was strapped with wool and crepe.
Patients were allowed to full weight-bear as tolerated and were advised to elevate their foot. The foot strap was removed after 24 to 48 hours. Active movement of the joint was encouraged as soon as pain allowed. Range of motion exercises were performed by patients themselves and no formal physiotherapy was employed. A single postoperative X-Ray was taken at the first follow up appointment at which time the sutures were also removed.
MOx-FQ scores were analysed as total scores, and as three subcategories: walking/standing; pain; and social interaction. Raw scores were converted to metric scores for each of the analyses to increase sensitivity as instructed by the user manual. MOx-FQ scores preoperatively were compared with those at 3, 6, 12 and 24 months and the distribution of differences was analysed using the Wilcoxon signed-rank test.
 Figure 1: Cartiva® implant. View Figure 1
Figure 1: Cartiva® implant. View Figure 1
ROM was calculated by summing values for dorsiflexion and plantarflexion. Preoperative ROM was compared with ROM at follow up and the mean difference was analysed using a paired T-test. Limited data were available for ROM at 24 months and Wilcoxon signed-rank test was utilised for this analysis.
A P‐value of < 0.05 was considered to be statistically significant. Data were stored using Microsoft Excel and SPSS version 25.0 for Windows was used for analysis.
A total of 19 SCI operations were conducted over the study period, 9 right toes and 10 left toes. These were from 16 patients, 11 female and 5 male, who had a mean age of 53 years (range 37 - 64). Thirteen toes were classified as (C&S) grade 4 and 6 were classed grade 3. See Figure 2 for a typical preoperative and postoperative radiograph.
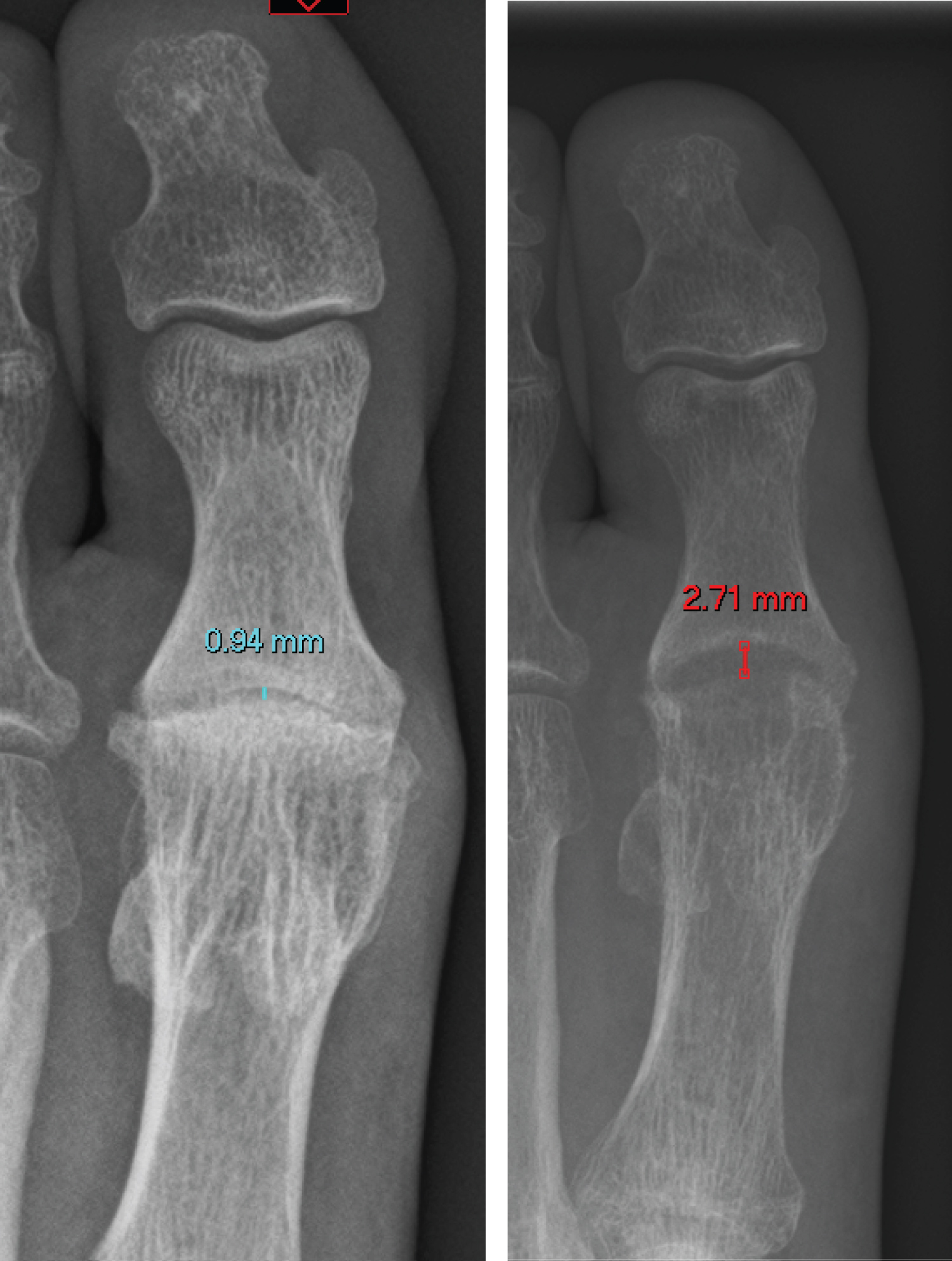 Figure 2: preoperative and postoperative radiograph demonstrating increased joint space. The cavity in the metatarsal head housing the implant is also visible on plain films. View Figure 2
Figure 2: preoperative and postoperative radiograph demonstrating increased joint space. The cavity in the metatarsal head housing the implant is also visible on plain films. View Figure 2
Complete MOx-FQ data were collected at 3 and 6 months follow up for all patients. At 12 months follow up, complete data were collected for 14 of 19 cases and there were complete data for seven patients at 24 months postop. Median metric scores for the MOx-FQ total and sub-scores at baseline and follow up are displayed in Table 1.
Table 1: Median MOx-FQ total score and subgroup scores pre-operatively and at follow-up. p values from Wilcoxon Signed-Rank test. View Table 1
Median total MOx-FQ score for each interval is displayed in Figure 3. The median metric MOx-FQ score preoperatively for the series was 53.13. Three months postoperatively this improved to 32.81 and this further improved to 17.19 at 6 months. Median metric total MOx-FQ score at 12 months was 17.97 for the available patients and this was 29.69 at 24 months. Improvements in scores were statistically significant at all points of follow up when compared with preoperative scores.
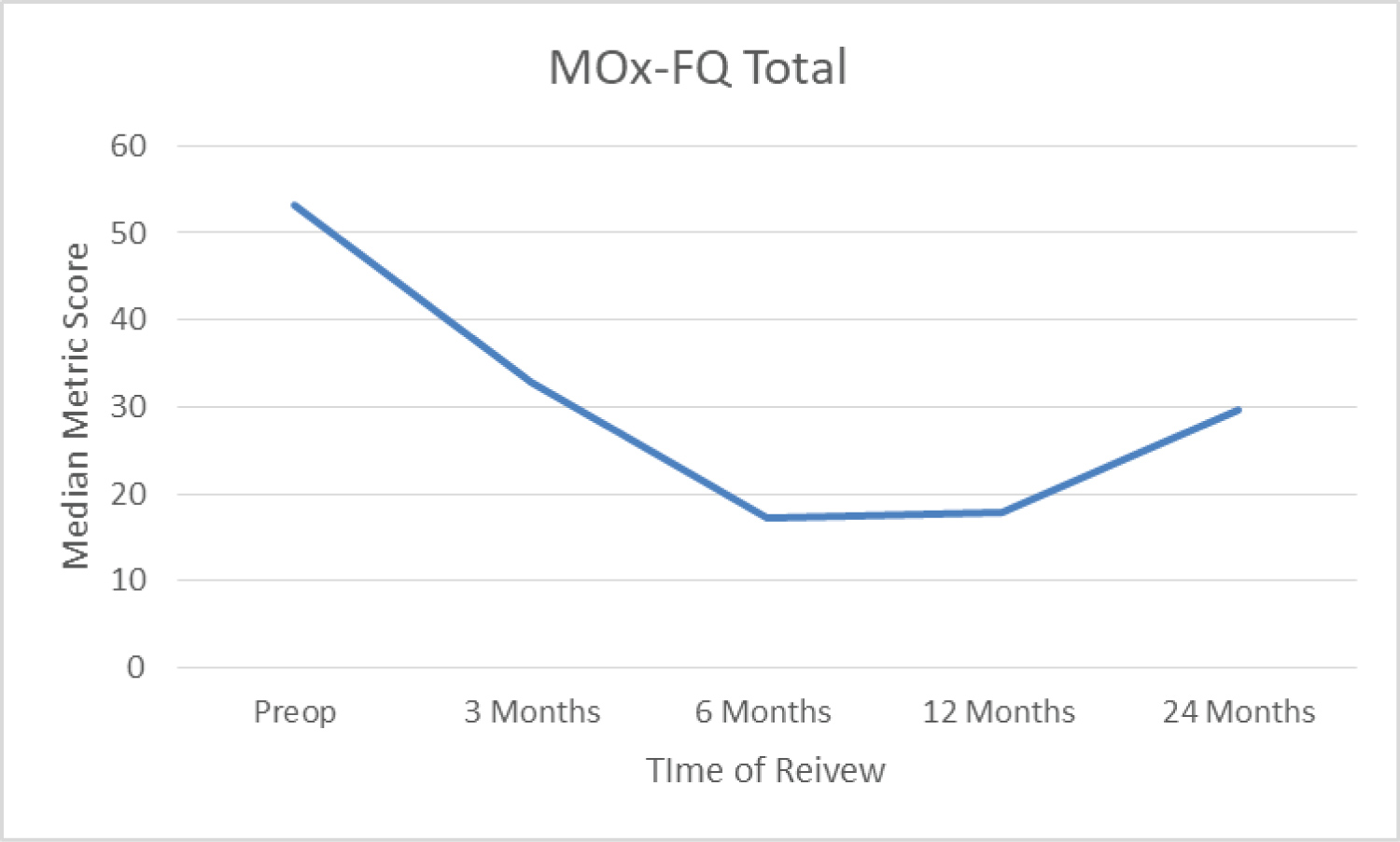 Figure 3: median total MOx-FQ score. View Figure 3
Figure 3: median total MOx-FQ score. View Figure 3
Walking/standing scores are graphically displayed in figure 4. The median metric score improved from 53.57 preoperatively to 39.29 at 3 months follow-up. This improved again at 6 months to 17.86 and again to 10.71 at 12 months. The scores appeared to increase as 24 months with a median metric score of 28.57. Significant improvement in scores were seen at all point of follow up when compared with those at baseline.
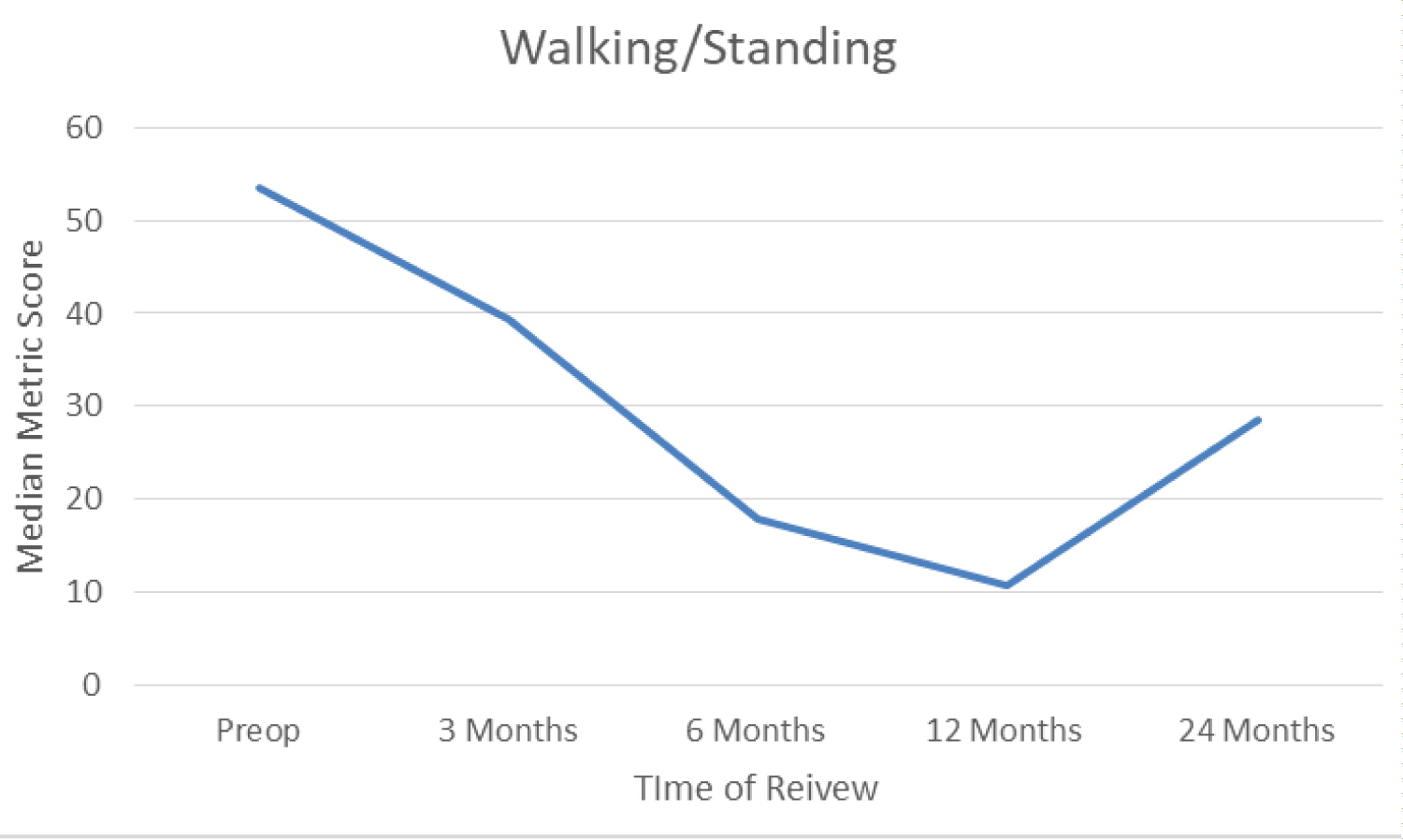 Figure 4: median walking/standing score. View Figure 4
Figure 4: median walking/standing score. View Figure 4
Pain data are displayed in Figure 5. Median score improved from 65 preoperatively to 30 at three months. This again improved to 20 at six months. Scores increased to 30 at 12 months and were 35 at 24 months. Pain had significantly improved at all points of follow up when compared with baseline score.
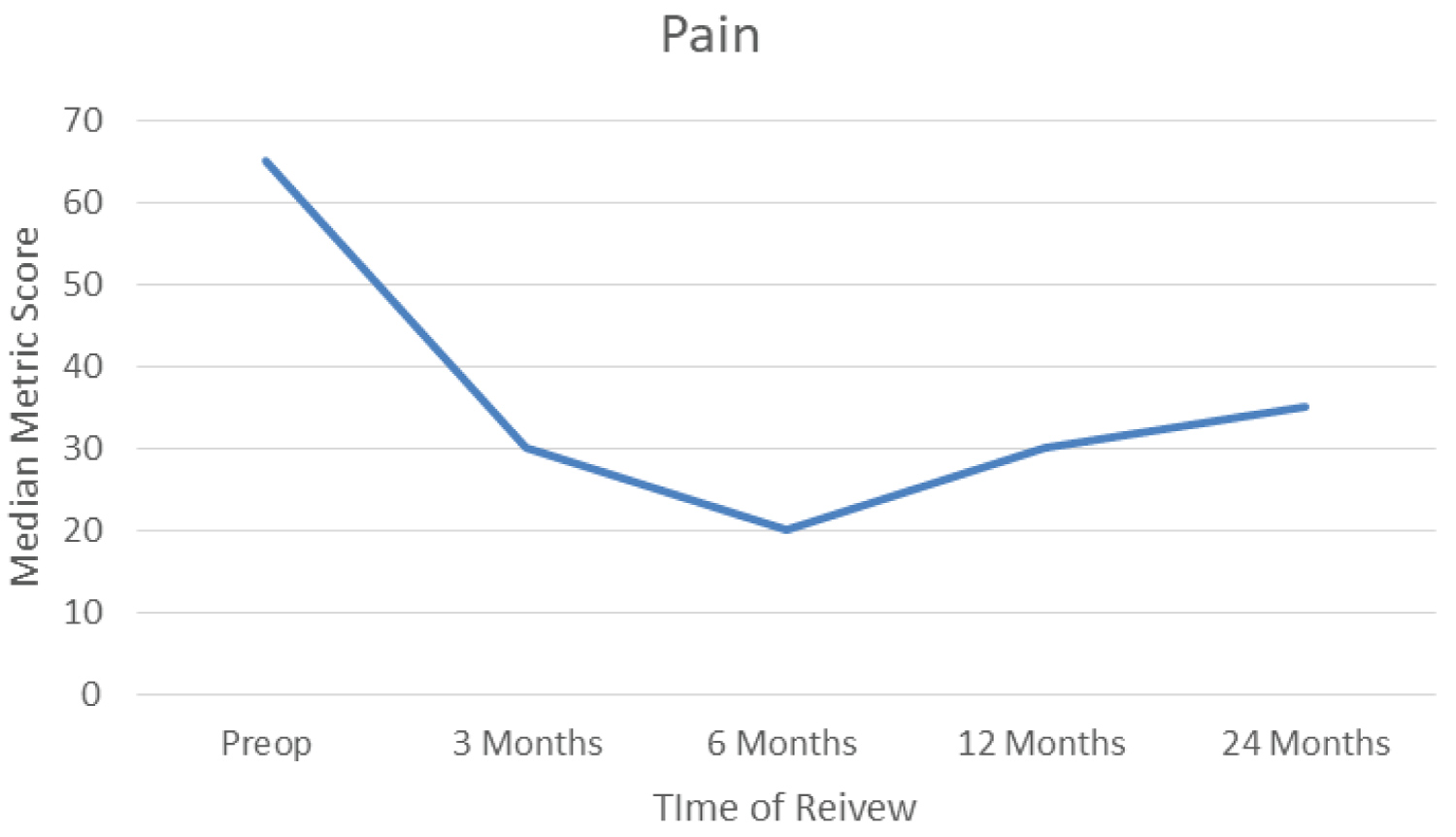 Figure 5: Median pain score. View Figure 5
Figure 5: Median pain score. View Figure 5
Median social interaction score was 43.75 preoperatively. This improved to 18.75 at 3 months and to 12.50 at 6 months. Median metric score was 12.5 at 12 months and median score was 0.00 at 24 months follow up. Again, significant improvements were seen at all points of follow up when compared with baselines scores.
ROM data for the series are reported in table 2. Complete data were collected for all 19 toes pre-operatively and at 3 months postoperatively. Data were collected for 18 of 19 toes at 6 months, 13 of 19 at 12 months and 5 of 19 toes at 24 months.
Table 2: Range of movement in degrees preoperatively and at each point of follow up. P values reported from paired t tests comparing total ROM to pre-op except a which is from a Wilcoxon Signed-Rank test. View Table 2
Mean ROM preoperatively was 31.84 degrees. This improved to 55.00 and further to 63.24 degrees at 3 and 6 months follow up respectively. This dropped slightly to 59.29 degrees at 12 months. ROM had significantly improved at all points of follow up when compared with baseline. Median 24-month ROM was 80.00 and this was marginally significantly higher than baseline (p=0.043).
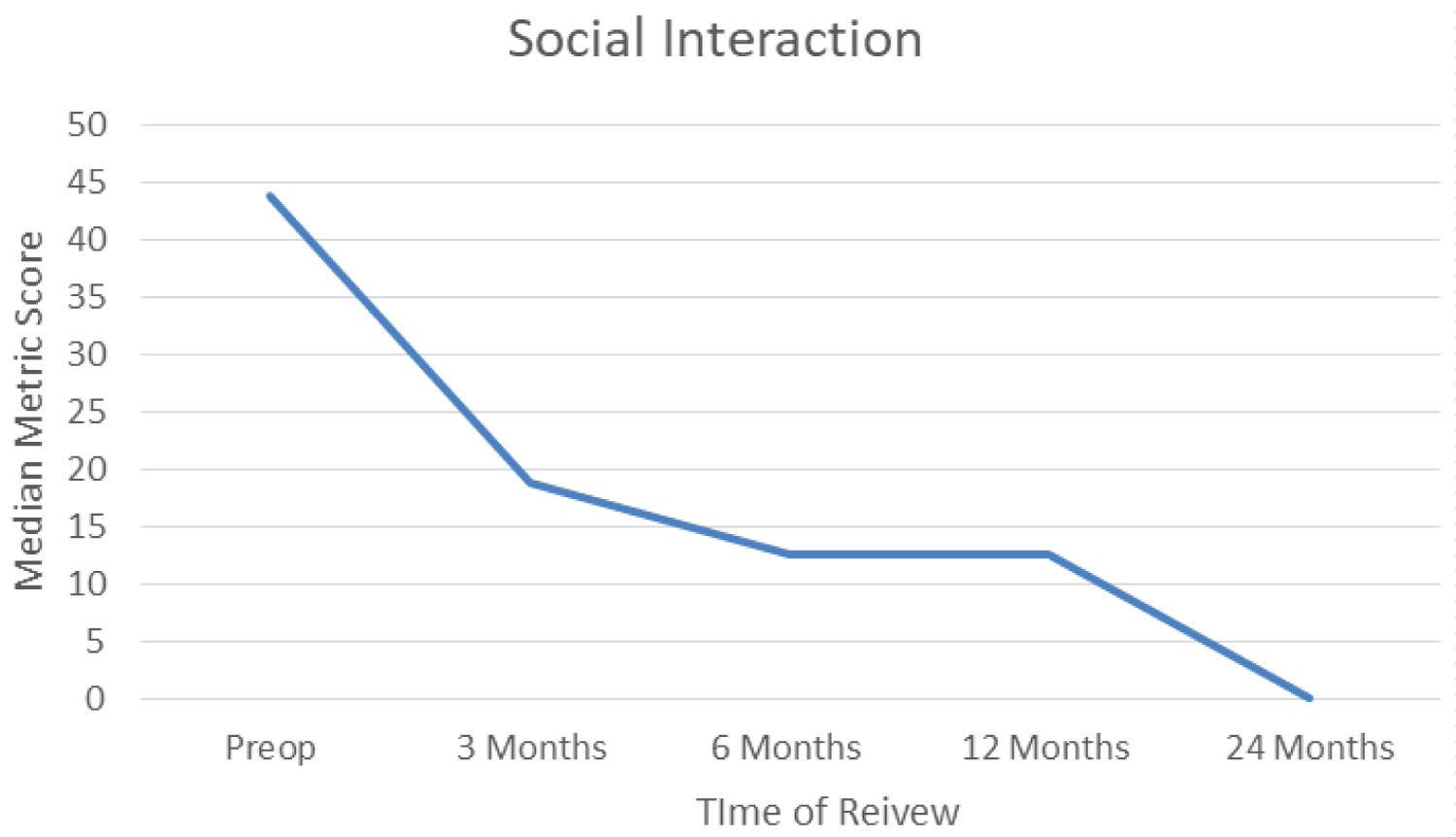 Figure 6: Median social interaction score. View Figure 6
Figure 6: Median social interaction score. View Figure 6
These data are displayed graphically in Figure 7 except for ROM at 24 months.
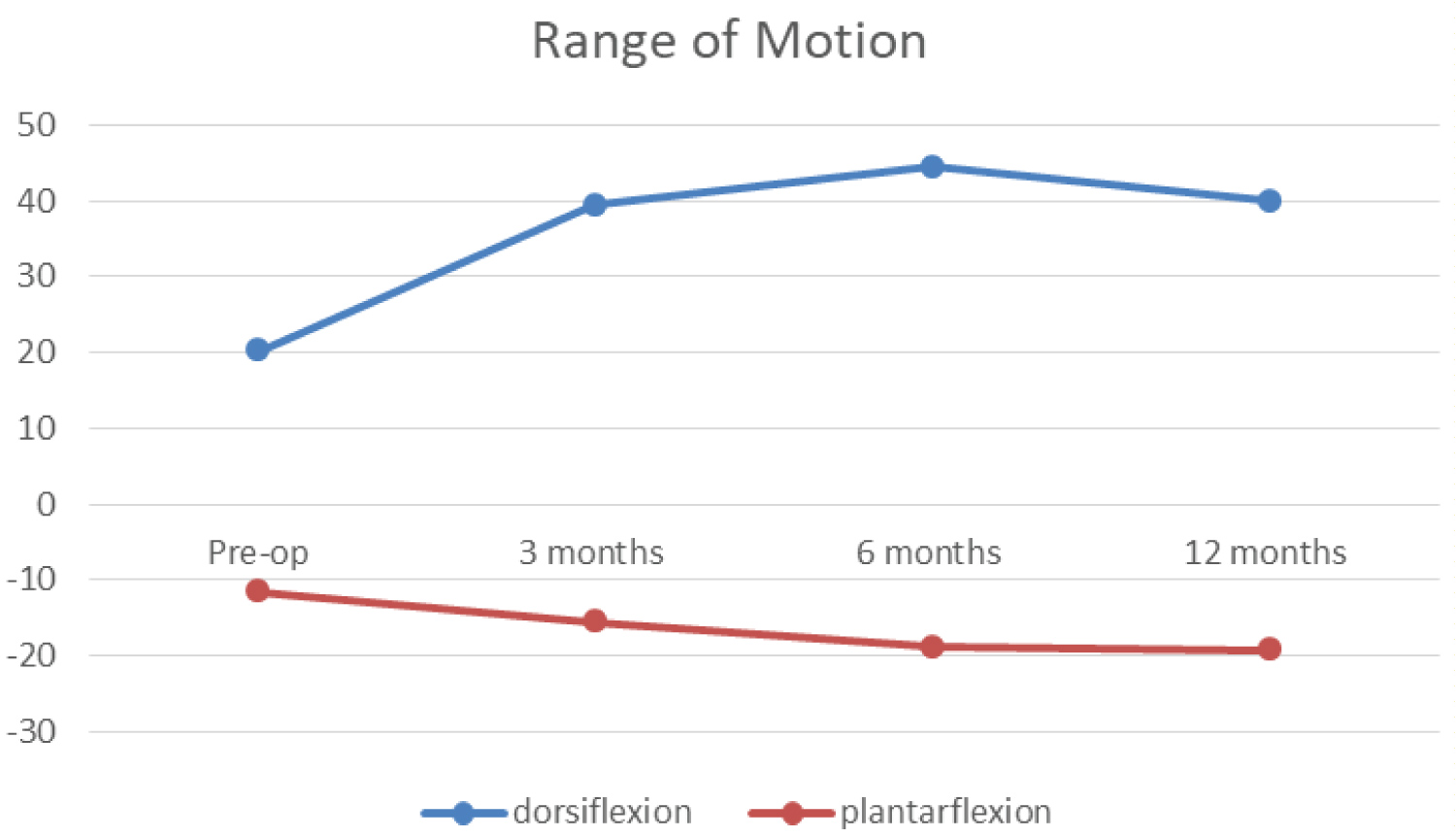 Figure 7: Mean dorsiflexion and plantarflexion in degrees. The area under the curves represents total arc of motion. View Figure 7
Figure 7: Mean dorsiflexion and plantarflexion in degrees. The area under the curves represents total arc of motion. View Figure 7
Two patients had persistent pain and stiffness after SCI. One patient responded well to cortisone injections and manipulation under anaesthesia and remains under review at the time of writing. The second patient underwent 1st MTPJ fusion. This decision was made at 24 months after the primary operation at which time the patient had a metric MOx-FQ score of 71.9. Of note, this patient had two failed temporo-mandibular joint replacement surgeries prior to SCI which left her with an extremely limited mouth opening. She is suspected to have an undiagnosed inflammatory arthritis, and in hindsight, the authors feel that this may have been a case of poor patient selection. Although not considered a significant complication, it is worth mentioning that one patient reported a faint sensation resembling rubber against mirror surface when moving her toe. This "squeegee" sensation, which was appreciable on clinical examination, was not associated with pain or any other symptoms and had resolved spontaneously at the 6-month review. Thereafter, patient went on to undergo SCI replacement on the other big toe. This issue was not highlighted in the reviewed literature and it is possible that this was a result of a proud implant, which settled with time.
Our audit shows good outcomes of SCI replacement for advanced hallux rigidus in a young series of patients without hallux deformity. Patients had significant improvements in self- reported pain, mobility and social function. Our series also indicate preservation and improvement of range of motion up to 2 years postoperatively.
The findings of this audit are consistent with other series in the literature, demonstrating positive short-term outcomes. Randomised controlled trial data for 106 patients demonstrated significant improvements in pain scores and function up to 5 years postoperatively and reported high levels of patient satisfaction [10].
Our data demonstrate peak results at 6 months followed by declining trend in the MOx-FQ scores except social interaction, although all scores remain significantly better those preoperative scores all throughout the study period. Other studies showed consistent improvements in outcomes up to 5 years follow up [11]. All patients in our series had a routine follow up of 6 months and data was collected after this period opportunistically with data available for 14 of 19 and 7 of 19 patients at 12 and 24 months respectively. To explain the trend, we speculate that patients returning after 6 months are the ones who are having a relatively poorer outcome.
Cartiva® SCI is shown to have a survivability similar to arthrodesis with around 10% of cases requiring a secondary procedure [8]. The current series shows a revision rate of 5% (1 of 19 cases). One series reports that nearly a third of their cases require manipulation under anaesthesia for stiffness [13]. Only one patient (5%) in the current series required manipulation. The patient remains under review and it is anticipated he will require fusion in the near future.
Owing to the minimal dissection and bone stock preservation with SCI, the authors found that, in the singular case that needed revision, conversion to arthrodesis was straightforward. This is consistent with reports from other studies [9]. However, in the case in the current series, the implant cavity needed filling with a small amount of bone chips during the fusion procedure.
This study had several limitations. The follow up period was limited by local policy and hence long-term symptom change and integrity of the implant could not be assessed. This also resulted in little data available at 12 and 24 months. Additionally, the small sample size and selection of young patients limits the generalisability of these results.
Cartiva® SCI replacement has a good short-term patient-reported outcome. It relieves pain and it preserves and improves joint movement at the same time.
It is a sound alternative to fusion for young patients with advance hallux metatarsophalangeal joint osteoarthritis and no hallux deformity.
However, a long-term study is required to determine if the currently favourable outcomes are maintained and to determine the long-term survivorship of the implant.
What is already known:
• Cartiva® provides similar pain relief to 1st metatarsophalangeal joint fusion in advanced hallux rigidus without deformity.
• Good short-term to mid-term results.
• Operative method is simple, with shorter post-op recovery compared to fusion.
What this study adds:
• Our study provided pre op and post op ROM, most studies only report post op movement.
• The procedure does not require specialised set up and can be done in small DGH setting.
• Revision to fusion, although technically easy, requires the use of bone chips to fill up the implant cavity.
None
We declare no conflict of interest.
None of the authors have received grants or financial support of any kind from the manufacturer of Cartiva® SCI during the conduct of this study.