Introduction: Synovial chondromatosis (SC) is a rare benign condition which involves synovial metaplasia and proliferation resulting in formation of multiple cartilaginous nodules in the synovium of the joints. It most commonly involves large joints such as hips and knee and is less frequently present in smaller joints. While it is a benign condition, primary synovial chondromatosis (PSC) can undergo malignant transformation into synovial chondrosarcoma. Their clinical and radiological features are very similar, and this may pose a problem for diagnosis. We have a described a case of Synovial Chrondromatosis where unusual histopathology was reported, and there were concerns regarding malignancy.
Case summary: A 49-year-old male originally presented with a history of severe intermittent pain and swelling in his left ankle joint. He is an extremely active builder and has been playing football for decades. Radiographs revealed an unusual appearance that was consistent with Synovial Chrondromatosis. After the clinical and radiological assessment, the lesion was excised along with cartilage and bony tissue. Histopathological study confirmed the findings of Synovial Chrondromatosis and showed the presence of a concerning degree of spindling and atypia of the cells.
Conclusion: This case highlights the potential issues that can arise when trying to distinguish primary synovial chrondromatosis from a malignant synovial chondrosarcoma based on histopathology. When such concerns arise, it is advisable to completely excise the lesion to remove a possible malignant tumour and for symptomatic relief for patients.
Synovial chondromatosis (SC) is a rare benign condition that involves the synovial lining of joints, synovial sheaths and bursae [1]. Metaplastic transformation takes place in the synovium producing intra-articular cartilaginous nodules [1]. These nodules break away forming loose bodies in the joint and may undergo secondary calcification thereafter [2]. SC typically presents in the fourth to fifth decade of life [3] with large joints such as hips and knees being mainly involved [4]. Patients usually present with pain, swelling and restriction of movements [5]. While SC is benign, one possible complication is malignant transformation to a synovial chondrosarcoma. Multiple reports estimated that the incidence of a synovial chondrosarcoma developing from SC range between 1%-6% [6,7]. The aim of this case report is to present a case of SC where there was an unusual finding on histopathology and multiple reviews and further surgery was required because of concerning malignant features.
A 49-year-old male presented initially with a chronic history of pain and swelling in his ankle. He lived a very active lifestyle working as a builder and playing football regularly. These symptoms started at the age of 27 when he sustained a significant inversion injury to his left ankle. He would experience intermittent episodes of severe pain and swelling in his ankle followed by these manifestations settling. MRI perfomed in 2005 confirmed Synovial Chrondromatosis. His symptoms settled with non-operative treatment, but he presented again 16 years later with complaints of recurrence of pain and instability in his ankles.
On examination, there was normal gait and alignment. There was swelling around the lateral malleolus and a bony prominence anterior to the fibula. Tenderness over the lateral ligament complex was present. The subtalar range of motion was significantly reduced by up to 50% and there was reduced plantar flexion as well. These examination findings suggest mechanical impingement.
Radiographs revealed an unusual appearance which was reported as being consistent with SC in the ankle. It showed multiple small, calcified bodies surrounding the left ankle joint, there was also a calcified mass noted in the anterior aspect of the distal fibula. A CT Scan was performed, looking at the extent of infiltration of the lesion (Figure 1).
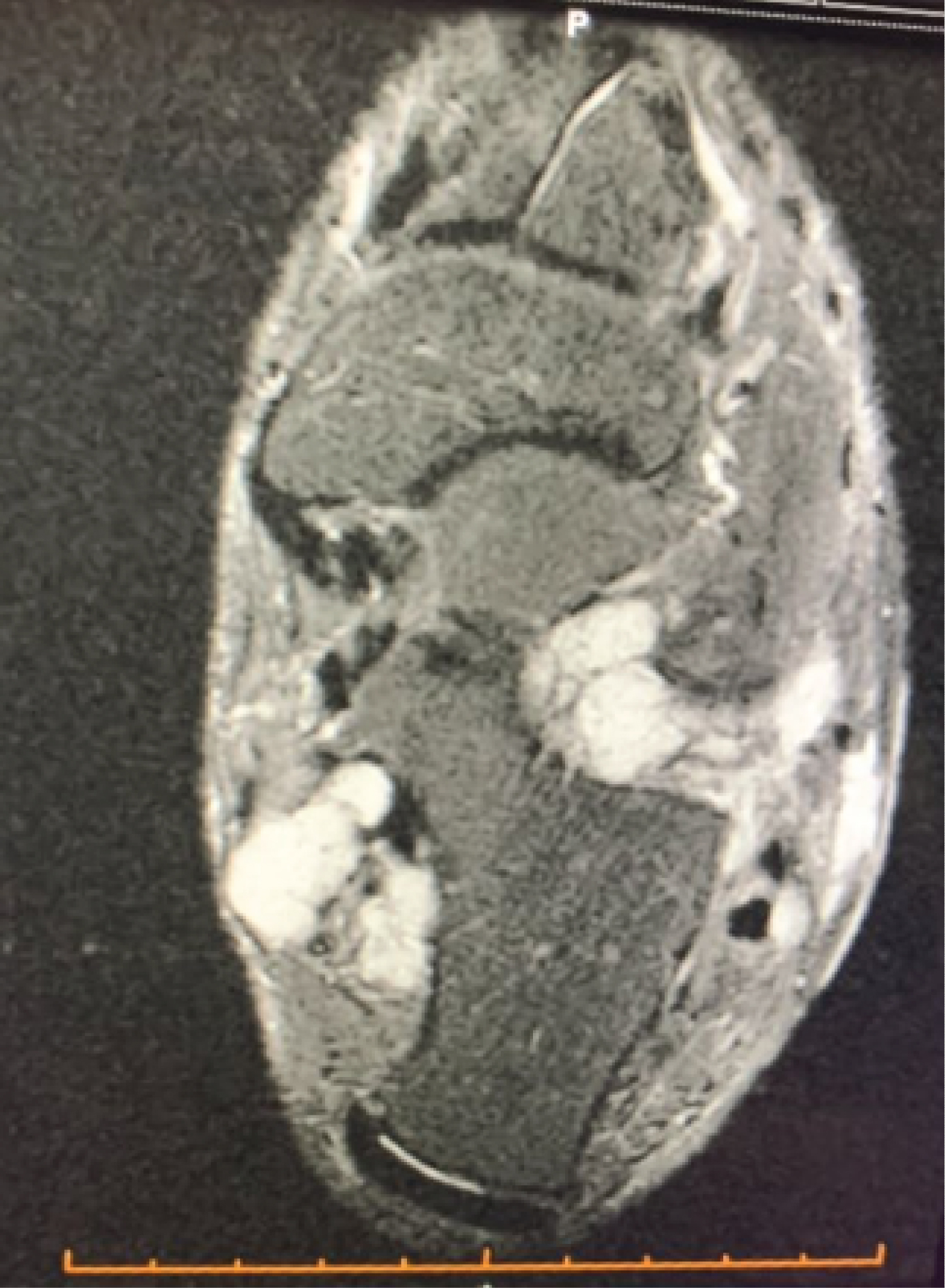 Figure 1: CT scan showing a cartilaginous lesion growing around the ankle joint. View Figure 1
Figure 1: CT scan showing a cartilaginous lesion growing around the ankle joint. View Figure 1
Surgical management was indicated where excision of the lesion that was causing impingement laterally was performed. A lateral incision was made, and a massive lesion found lateral to the fibula and anterior to the ankle was removed. The lesion measuring 60 × 45 × 12 mm consisted of bony fragments and dense cartilage tissue with possible overlying synovium.
On histopathological examination, the diagnosis of SC was made. However, there were concerning features, particularly the presence of increased cellularity at the periphery of the nodules with spindling of chondrocytes and nuclear atypia. These histological features are not diagnostic however they raise suspicion for a chondrosarcoma developing in the SC. It was suggested that immunostaining be performed to clarify the presence of histiocytic differentiation in these atypical cells. CD163 and CD 68 were performed and showed that many of the atypical looking cells are histiocytic in nature. However, Ki67 proliferation was low and PHH3 immunostaining failed to identify definite mitotic activity in these regions. Therefore, there were no conclusive features of malignancy.
An MRI was performed after the operation to look for evidence of malignancy. A T2 hyperdense lobular lesion was found in the ankle and subtalar joints and this appearance suggested the diagnosis of SC with no other notable features pointing towards to a malignancy. The MRI also showed multiple deposits remaining in the ankle joint.
Patient was pain free post-surgery supporting a diagnosis of lateral impingement caused by the tumour mass. Bone tumour units in Royal Prince Alfred and New York Bone Tumour reviewed the histology as seen in Figure 2 and suggested complete excision of all SC deposits. Further resection was then performed and no malignant transformation identified (Figure 3).
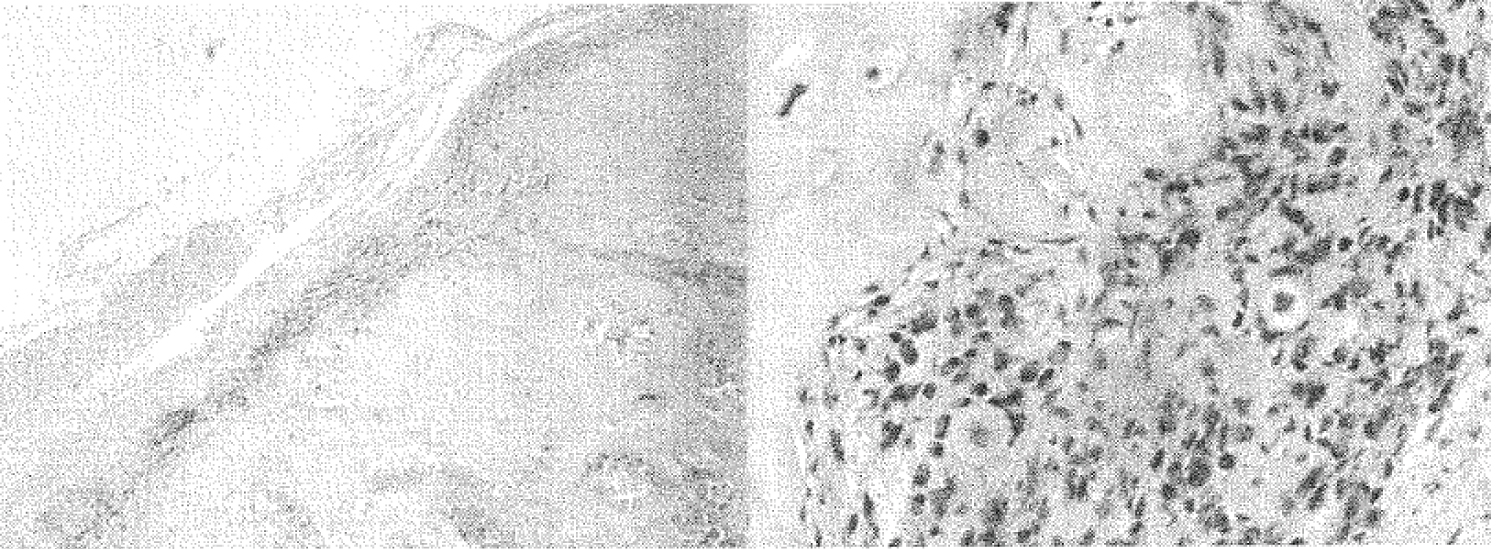 Figure 2: Spindling and atypia of the cells seen at the perimeter of lobules. View Figure 2
Figure 2: Spindling and atypia of the cells seen at the perimeter of lobules. View Figure 2
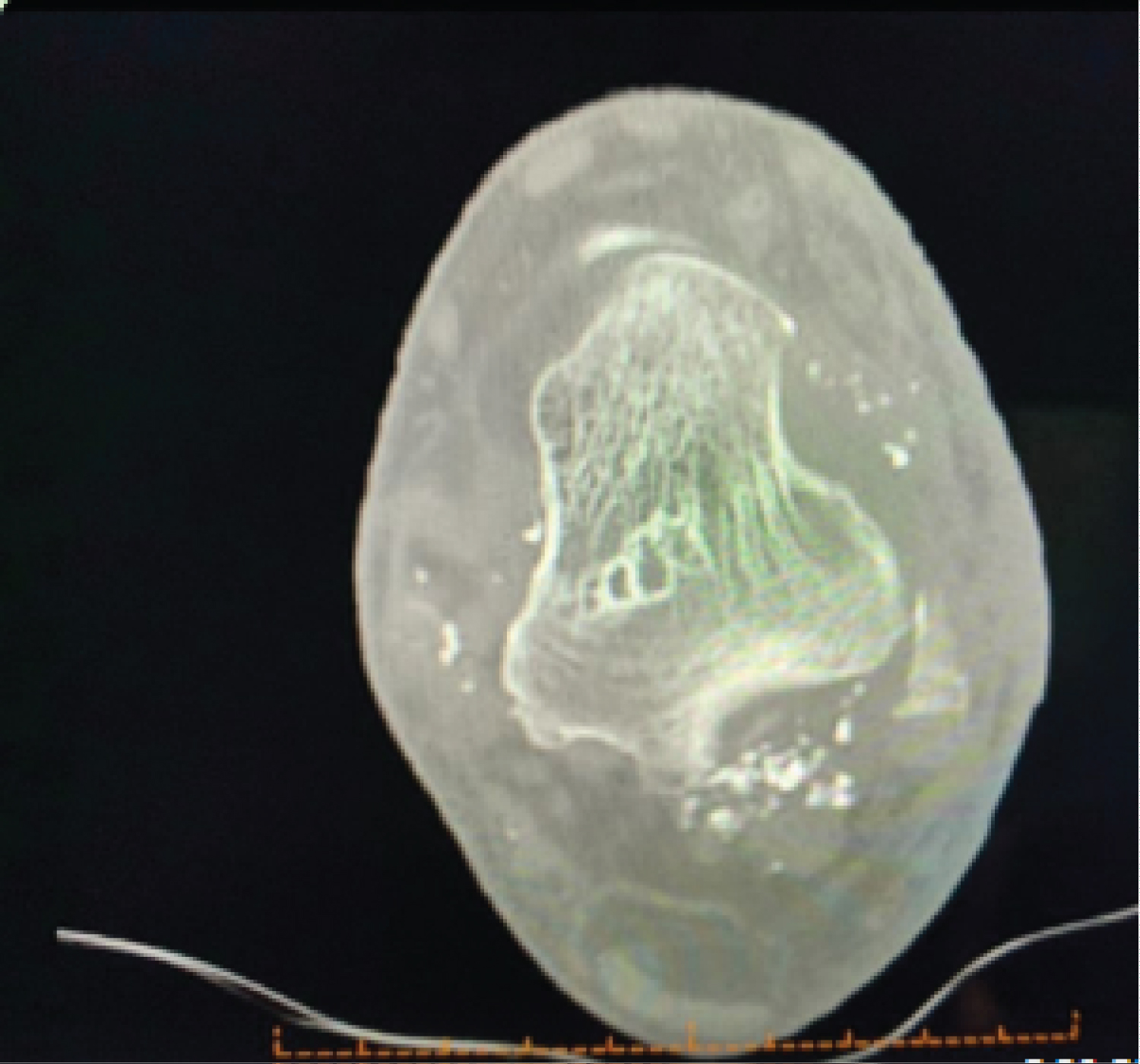 Figure 3: MRI performed post first surgery showing multiple deposits around the ankle joint. View Figure 3
Figure 3: MRI performed post first surgery showing multiple deposits around the ankle joint. View Figure 3
SC is an uncommon benign metaplastic condition which involves the formation of cartilaginous bodies within the synovium and subsynovial connective tissues of typically large joints [1]. Milgram's study demonstrated 3 phases of disease process. Phase 1 involves metaplasia of synovium with active synovitis and absence of loose bodies. Phase 2 involves active synovitis with the formation of loose bodies, which are still cartilaginous. Phase 3 occurs when these loose bodies calcify and the synovitis subsides [8]. SC usually presents with pain, swelling and may have a mass. It can be diagnosed using X-ray, CT or MRI with MRI being described as the best imaging modality when ossification and calcification cannot be demonstrated [9].
While SC is a benign condition, it has the potential to undergo malignant transformation. Primary SC has the tendency for recurrence however does not metastasize. It can be managed with a total synovectomy along with removal of the loose bodies [10]. Chondrosarcoma however is a malignant condition requiring wide excision of the lesion and depending on the extent of the spread, an amputation may be required [11]. One study observed that the mean age of their participants presenting with SC was 28-years-old and median time from original diagnosis to malignant transformation being 20 years [6]. Because of the differences in prognosis and management, it is important to differentiate between these conditions.
An accurate diagnosis is made on the combined decision made from clinical findings, radiography (X-ray, MRI), and histopathology [12]. Histologically it is difficult to differentiate low-grade chondrosarcomas and SCs [13]. On histology, primary SC would be seen as lobules of hyaline cartilage that are frequently hypercellular with atypical histological features such multinucleation, nuclear crowding, nuclear enlargement and hyperchromasia with mild myxoid changes [14]. These atypical features could be interpreted as a low-grade chondrosarcoma when there is a high degree of cellularity and nuclear atypia. Another study discussed several histological features which favoured malignancy, and these include loss of clustering growth pattern typical of PSC, myoid change in the matrix, areas of necrosis, presence of mitotic figures and hypercellularity with spindling of the nuclei at the periphery [15], however might still not be accurate because they can be missed on resection [13].
Immunohistochemical markers can be used to differentiate however there is no definitive technique to diagnose chondrosarcoma [16]. There are some biomarkers which have been reported to help distinguish between the two pathologies such as reduced or absent expression of BCL2 [17] and expression of Ki67 which is associated with cell proliferation [18].
The patient's histopathology report was concerning because of the high degree of spindling and atypia of the cells at the periphery of the lobules. These could be a feature of low-grade chondrosarcomas but Synovial Chondromatosis can develop such features as well mimicking a low-grade chondrosarcoma [13]. On immunostaining, Ki67 proliferation and mitotic activity was not found which would be other key features of malignancy. Another feature that was concerning for our patient was the size of the lesion. The high degree of spindling was a cause of worry when reviewed by the Bone Tumor Units and they suggested that the patient undergo a repeat surgery to completely remove any remaining deposits [19].
This case adds on to the current literature of highlighting the dilemma of distinguishing a synovial chondrosarcoma from synovial chondromatosis. If there are features which could suggest malignancy on either histopathology or radiology, patients should undergo complete surgical excision of the lesion with removal of all remaining deposits. Patients should then be followed up regularly with serial MRIs.