The bipartite medial cuneiform (BMC) is a rare congenital variant in the Lisfranc joint. In the majority of the cases BMC is asymptomatic and diagnosed as an incidental imaging finding. Clinical awareness of this entity is relevant when evaluating a patient with midfoot pain following both acute trauma or in the setting of chronic and insidious midfoot complaints.
The authors present a case of a 33-year-old male patient with pain in the dorsomedial aspect of his left midfoot due to a symptomatic BMC. In this paper, the authors aim to discuss the clinical and radiological characteristics of the disease as well as the crucial steps for a correct diagnosis and treatment, while reviewing the literature related to management of BMC.
Bipartite medial cuneiform, Midfoot pain, MRI, E-sign
V; Therapeutic Studies, Expert Opinion
Bipartite medial cuneiform (BMC) is a rare congenital anatomical variant in the Lisfranc joint, first described in the 18 th century [1,2]. It refers to a non-fusion phenomenon of the two primary ossification sites of the medial cuneiform, which usually occurs in the second decade of life. Consequently, there is a separation of the normal medial cuneiform into two ossicles, forming a pseudo-joint that can be composed of cartilaginous synchondrosis, fibrous syndesmosis, or a combination of both [3,4]. BMC incidence is estimated to be between 0.1% and 2.4% in the general population [3-5].
In the majority of the cases, BMC is asymptomatic and diagnosed as an incidental imaging finding. Awareness of this anatomic variant may become clinically relevant when evaluating a patient with midfoot pain following both acute trauma or in the setting of chronic and insidious midfoot complaints [1].
According to the literature, conservative treatment is considered the first line of treatment including non-weight bearing, custom-design orthosis, non-steroid anti-inflammatory drugs, and image-guided corticosteroid injection [6-9]. Classically, surgical treatment is reserved for the cases that do not respond to conservative measures and can include fusion or excision procedures.
The authors describe a case of a 33-year-old male patient who works as a self-employed driver and has no significant medical history. He refers pain in the dorsomedial aspect of his left midfoot for two weeks. According to the patient, there was no recent history of injury. He reported that the pain was elicited with midfoot and hindfoot pronation, and it aggravated with load bearing. He didn't experience any nocturnal pain.
Inspection revealed no signs of swelling or other abnormalities on the skin of the left foot. There was focal tenderness over the dorsal aspect of the first tarso-metatarsal joint and pain was elicited on the same topography with passive inversion and inversion against resistance of the midfoot. No instability was observer in the medial column. Neurovascular examination was unremarkable. Silfverskiöld test was positive, indicating tightness in the gastrocnemius muscle, and a podoscopy examination showed normal plantigrade feet.
The initial diagnostic workup began with weight-bearing radiographs, which ruled out any acute fractures or diastasis of the mid-foot. Instead, the images revealed two well defined osseous segments that had replaced the normal radiological appearance of the medial cuneiform. Subsequently, Magnetic resonance imaging (MRI) was conducted and demonstrated that the medial cuneiform had a complete bipartite configuration. This configuration included a well-defined dorsal and plantar segment, with smooth, even cortical margins in the posterior region, and some irregularity in the anterior cortex, forming a synchondrosis (Figure 1, Figure 2, Figure 3 and Figure 4). Additionally, sub-cortical changes were noted, with presence of subchondral cysts in the dorsal medial segment of the cuneiform and a mild bone marrow edema pattern.
 Figure 1: T1-weighted (Fat-supression) left foot MRI, in sagittal view, showing the bipartite medial cuneiform with well-defined dorsal and plantar segment, forming the classic E-sign.
View Figure 1
Figure 1: T1-weighted (Fat-supression) left foot MRI, in sagittal view, showing the bipartite medial cuneiform with well-defined dorsal and plantar segment, forming the classic E-sign.
View Figure 1
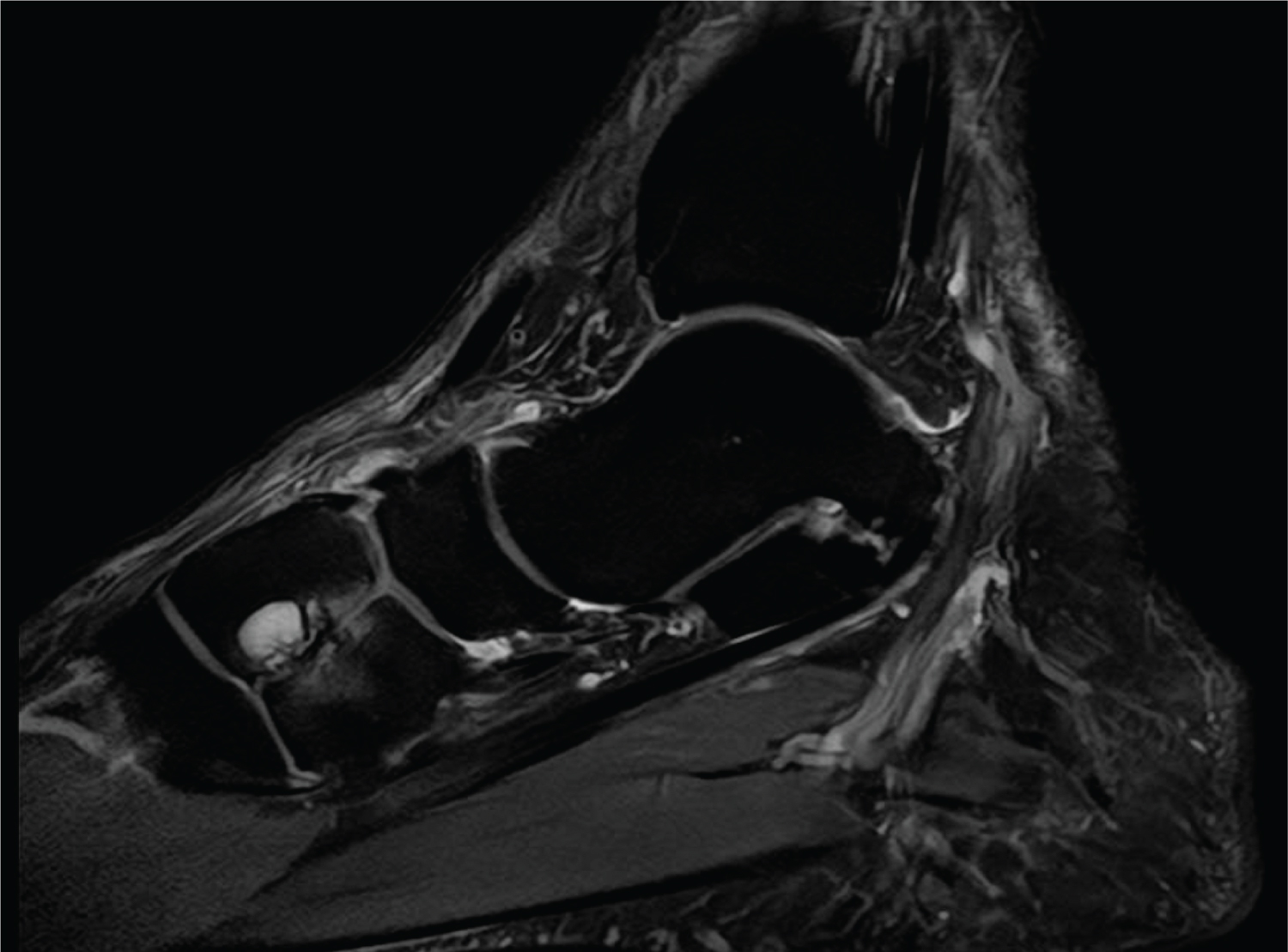 Figure 2: T2-weighted left foot MRI, in sagittal view, showing the presence of subchondral cysts in the dorsal segment of the medial cuneiform and a mild bone marrow edema pattern.
View Figure 2
Figure 2: T2-weighted left foot MRI, in sagittal view, showing the presence of subchondral cysts in the dorsal segment of the medial cuneiform and a mild bone marrow edema pattern.
View Figure 2
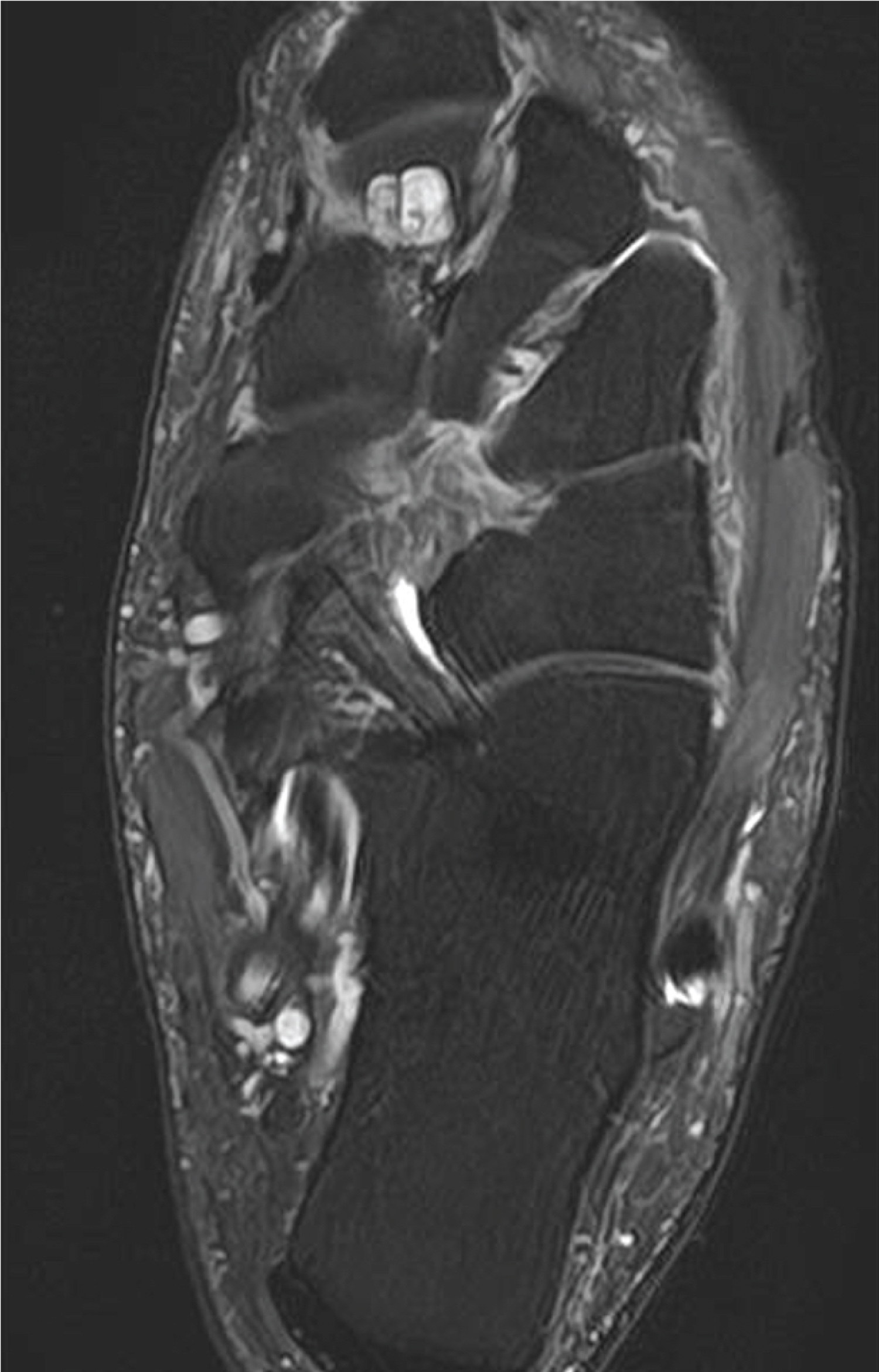 Figure 3: T2-weighted left foot MRI, in axial view, showing the presence of smooth, cortical margins in the posterior region of the medial cuneiform and some irregularity in the anterior cortex, forming a synchondrosis.
View Figure 3
Figure 3: T2-weighted left foot MRI, in axial view, showing the presence of smooth, cortical margins in the posterior region of the medial cuneiform and some irregularity in the anterior cortex, forming a synchondrosis.
View Figure 3
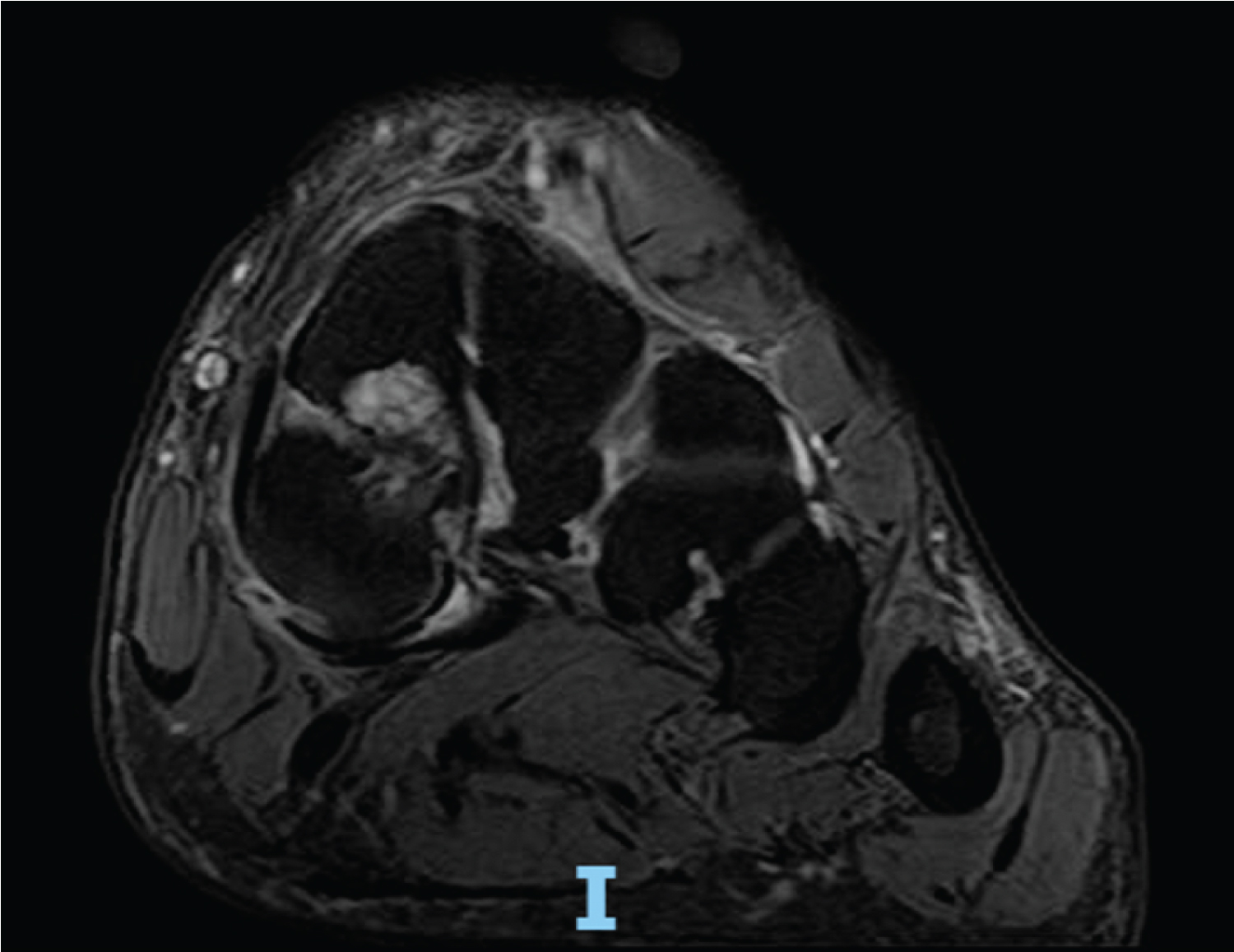 Figure 4: T2-weighted left foot MRI, in coronal view, showing the presence of subchondral cysts in the dorsal segment of the medial cuneiform.
View Figure 4
Figure 4: T2-weighted left foot MRI, in coronal view, showing the presence of subchondral cysts in the dorsal segment of the medial cuneiform.
View Figure 4
Conservative treatment was established with immobilization in a walker-boot, allowing partial weight-bearing during a period of two weeks and prescription of nonsteroidal anti-inflammatory drugs. After this initial phase, the patient was cleared for full-weight bearing and stiff custom-made plantar insoles with medial support were prescribed, to reduce motion of the mid-foot during gait. The patient also initiated a rehabilitation program focused on stretching the muscles of the posterior chain. The response to treatment was fairly positive. At three-month follow-up, the patient reported no pain during daily living activities, thus no further treatments were required.
BMC is a rare congenital anatomical variation occurring at the Lisfranc joint, representing a malsegmentation defect caused by non-fusion phenomenon of the two primary ossification sites of the medial cuneiform [3]. In the majority of the cases the bipartition displays a horizontal pattern, dividing the medial cuneiform in a plantar and dorsal segment [7]. The dorsal segment frequently presents lesser dimensions [1]. According to cadaveric studies, BMC has an incidence that ranges between 0.1% and 2.4% with a slight predilection for the male gender and can have bilateral expression in 60% of the cases [1,5,9]. BMC can be classified into three morphological categories: Type A: Complete bi-partition, with division of the medial cuneiform into dorsal and plantar segments. Type B: Incomplete bi-partition, with partial fusion of the two segments. Type C: Division occurring at the distal articular surface [10]. The type C seems to be the most commonly observed morphological variant [10].
Normally, BMC is asymptomatic and diagnosed as an incidental imaging finding. However, some authors hypothesized that this entity can alter the midfoot biomechanics and cause swelling, tenderness and dorsomedial foot pain [5].
According to Pollack, et al. BMC can be painful when there is micromotion between the two cuneiform segments, causing fibrocartilaginous synchondrosis inflammation and damage, that can ultimately predispose to arthritic changes [8]. Therefore, from a clinical standpoint it is important to consider BMC as differential diagnosis of acute or chronic midfoot pain. In the setting of acute trauma, BMC should be differentiated from an acute fracture. Making the diagnosis with plain radiographs can be challenging due to the superimposition of bony structures. A lateral 30° oblique views has been advoked to improve visualization of medial cuneiform bipartition [1]. The presence of the classical “E-sign” on the lateral view is also important in differentiating BMC from an acute medial cuneiform fracture and represents the joint space between the ossicles of the BMC and the first metatarsal base [5]. More advanced imaging techniques such as Computer Tomography (CT) and Magnetic Resonance Imaging (MRI) can be required to establish the correct diagnosis. CT scan permits 3D reconstruction, while MRI has the advantage of allowing visualization of bone marrow edema that is more characteristic of acute fracture, cyst formation and other arthritic alterations as well as evaluating the origin of Lisfranc ligament [8].
Conservative treatment is considered the first line of treatment including non-weight bearing, immobilization, non-steroid anti-inflammatory drugs and image-guided corticosteroid injection [6,8,9]. Eves, et al. reported a case of an 11-year-old patient with a symptomatic BMC treated with immobilization with a pneumatic walker boot, allowing increasing weightbearing as tolerated [4]. Offerhaus, et al. presented a posttraumatic symptomatic BMC in an adult patient that was treated with nonweightbearing and nonsteroidal anti-inflammatory drugs for 2 weeks with good functional results [1]. Panu, et al., Bismil, et al. and Steen, et al. reported 3 cases of successful symptomatic BMC treated with local corticosteroid injections [2,6,9].
Surgical treatment is reserved for cases that do not respond to conservative measures and can include excision of smaller fragments, osteosynthesis of the segments or fusion of the adjacent joints [8]. Excision procedures can be performed when the dorsal segment comprises 30% or less of combined segment area. Pollack, et al. postulated that fusion of BMC segments should be the preferred technique after failed conservative treatment in cases with no arthritic changes in the adjacent joints [8]. Extensive fusion procedures should be reserved to cases associated with clinical and imagological evident arthritic changes in the first metatarsal-cuneiform and first cuneiform-navicular joints [9].
The BMC is a rare developmental anatomic variant of the midfoot that is frequently asymptomatic. This clinical entity should be integrated in the differential diagnosis workup in cases of traumatic or chronic medial foot pain with no evidence of fracture on plain radiographs. This case demonstrates that conservative treatment should be always be attempted as first line of treatment prior to surgical intervention.
Informed consent was obtained from the patient for the publication of the case study.