Numerous graft materials have been utilized and described to achieve deformity correction in lateral column lengthening procedures (LCL) including autograft, allograft, xenograft, and porous titanium wedges (PTW). PTWs offer a potentially advantageous substitute for traditional grafts. Evidence regarding outcomes and complications of these grafts remains limited. This systematic review aims to describe functional outcomes and complications associated with LCL using PTWs. A standard methodology for performing a systematic review was followed using PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines. PubMed, Google Scholar, OVID, Embase, and Cochrane were searched. Publications with 1-year follow-up and LCLs performed with PTWs were included. Non-English articles and those that did not perform LCL with PTWs were excluded. 508 articles were identified. 7 studies met the inclusion criteria following our review. 246 LCLs (236 patients) using PTWs were reported. The Foot and Ankle Ability Measure Activities of Daily Living (FAAM-ADL) score measured at 80.45 (80.0-80.9) post-operatively. FAAM Sports subscale measured at 58.5 (50.0-66.9) post-operatively. VAS pain score decreased from 5.45 (5.0-5.9) pre-operatively to 2.43 (1.6-3.0) post-operatively. The total complication rate was found to be 15.2% (36/236). Major complications including non-union, reoperation, deep infection, and chronic regional pain syndrome (CRPS) were 2.1% (5/236). The evidence from this systematic review suggests that LCL with PTWs can be an effective and viable option for correcting flexible flatfoot deformities. The use of PTWs appears to offer comparable functional results and complication rates to traditional allograft or autograft wedges.
Level 3
Calcaneal lengthening osteotomy, Flexible flatfoot, Evans osteotomy, Graft, Lateral column lengthening, Porous titanium wedge
A flexible flatfoot deformity is a common condition characterized by a progressive collapse of the medial longitudinal arch of the foot [1]. It can be a debilitating condition resulting in significant pain, discomfort, and functional limitations for affected individuals. Various surgical techniques have been developed to correct this flexible deformity and restore normal foot function [2,3]. One such technique is lateral column lengthening (LCL), a workhorse joint-sparing procedure for surgeons treating flexible flatfoot deformities [1,4]. LCL requires interposition grafting to achieve and maintain deformity correction. Numerous wedge graft materials have been successfully described and utilized to achieve deformity correction including autograft, allograft, xenograft, and more recently, porous titanium materials [5-8].
Autograft harvested from the iliac crest has been historically considered the “gold standard” due to its osteoinductive and osteoconductive properties, however, it has been shown to correspond with donor site morbidity and increased operating room time [5]. Allograft and xenograft have been utilized to prevent donor site morbidity, however, both carry the risk of increased risk of non-union, graft rejection/resorption, and disease transmission [7,9]. Grier, et al. found increased union rates for LCL with the implementation of allograft wedges with the addition of platelet-rich plasma (PRP) when compared to tricortical iliac autograft [10]. Other comparative studies have shown no statistically significant differences between autograft and allograft wedges [6,7].
Ideal grafting material for LCL, as well as other foot and ankle procedures, is one that maintains long-term deformity correction and stability, reduces harvesting complications, eliminates potential disease transmission, and has osseointegration properties. Porous titanium wedge (PTW) grafts offer a potentially advantageous substitute versus more traditional LCL graft wedges. The use of porous metal grafts, most notably porous tantalum, is well established as a bone graft substitute in the hip and knee [11,12]. With its titanium structure, it effectively eliminates the risk of graft resorption and or vector transmission. The porosity allows osseointegration, promoting bone growth and fusion to surrounding osseous surfaces. Porous titanium has an elastic modulus and porosity, similar to that of subchondral bone, making it a viable substitute for conventional bone graft for structural support in deformity correction [13].
While LCL with PTWs has gained popularity in foot and ankle surgery in recent years, the evidence regarding its outcomes and potential complications remains limited. By analyzing a pool of relevant studies, this systematic review aims to assess the functional outcomes and complications associated with lateral column lengthening using PTWs.
The systematic review identified articles on LCL utilizing PTW for deformity correction which discussed outcomes as well as complications. A standard methodology for performing a systematic review was followed using PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines. PubMed, Google Scholar, OVID, Enbase, and Cochrane were searched on June 6, 2023. All publications with greater than 1-year follow-up, including LCLs performed with PTWs, were included in the systematic review. The following search criteria were performed: “Calcaneal lengthening osteotomy” AND “Flexible flatfoot” AND “Evans osteotomy” AND “Evans osteotomy graft” AND “Lateral column lengthening” AND “Porous titanium wedge”. Limits were placed to include articles in the English language.
A total of 508 articles were identified in the initial search. Each article was reviewed by 1 of 5 junior authors. If there was a question as to whether a particular article met the inclusion criteria, a second opinion was provided by the senior author (RM). After a thorough review of the pooled articles, 7 studies met the inclusion criteria. Data regarding functional outcomes as well as complications following LCL with PTWs were compiled by 5 researchers and accuracy was confirmed by the lead author (Figure 1).
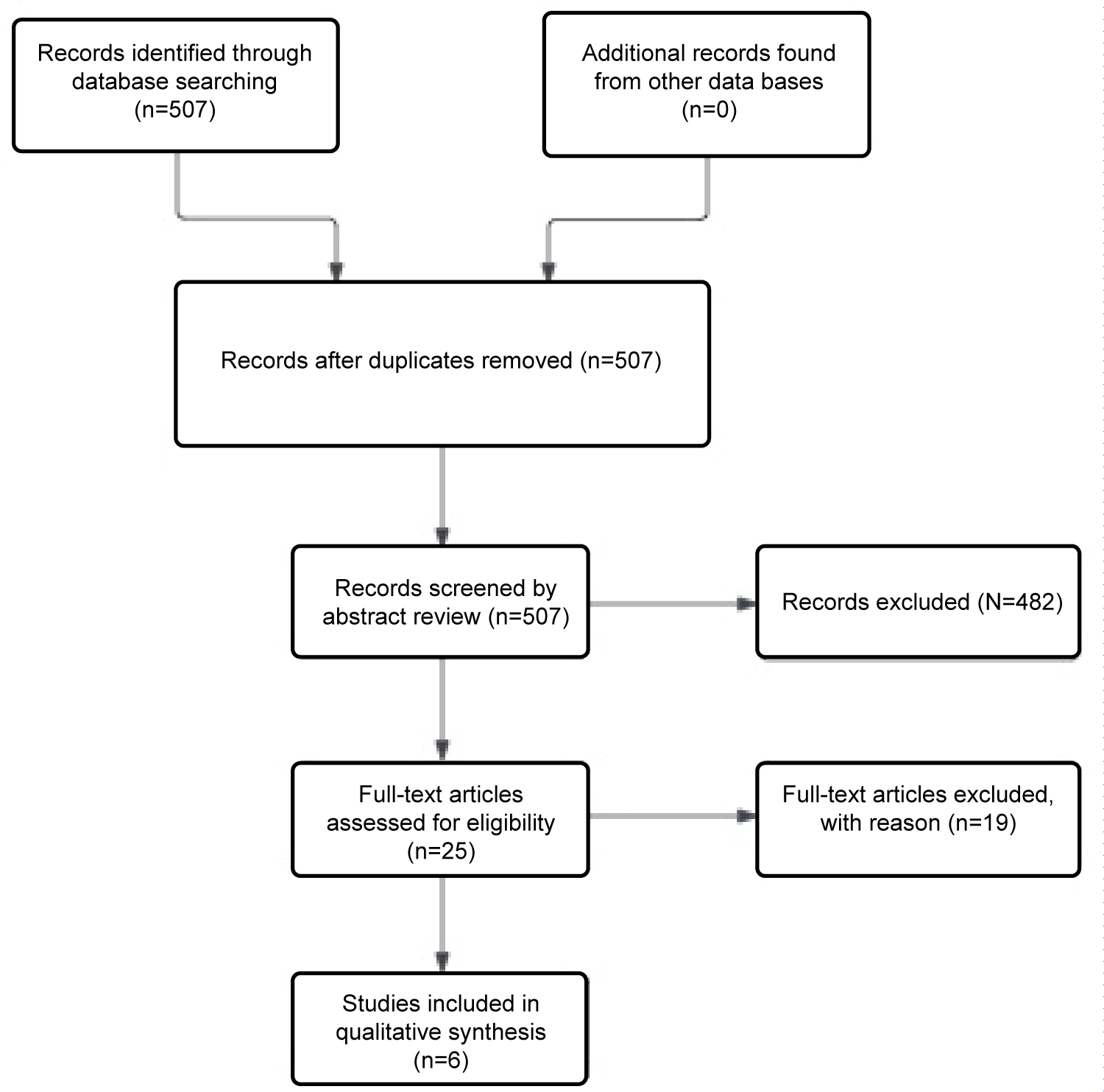 Figure 1: Systematic review methodology according to PRISMA guidelines. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
View Figure 1
Figure 1: Systematic review methodology according to PRISMA guidelines. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
View Figure 1
Following the review of 508 articles regarding LCL performed with PTWs, 7 articles met the inclusion criteria. Of the included studies, four were level 4 evidence and two were level 3. A total of 246 LCLs performed with a PTW was reported among 236 patients. The average age of the patients at the time of the procedure was 40.9 years-old (9-74 years). The average follow-up was 28.1 months (6-43 months). The average BMI of the included patients was found to be 29.4 (27-30.2).
The indication for the LCL procedure was a stage II flexible flatfoot according to the previously described Johnson and Strom classification [14] in 100% (236/236) of the included patients. Reported ancillary procedures varied from study to study. A cotton osteotomy was performed in conjunction with a LCL in 37.3% (92/246) of the patient cohort, tendon transfer in 26.4% (65/246), medial calcaneal displacement osteotomy (MCDO) in 20.7% (51/246), posterior tibial tendon (PTT) debridement in 13.0% (32/246), spring ligament repair in 11.7% (29/246), posterior muscle group lengthening in 8.9% (22/246), medial column fusion in 2.8% (7/246), distal bunion correction 0.8% (2/246), ankle arthroscopy in 0.4% (1/246), peroneus brevis repair in 0.4% (1/246), and first metatarsophalangeal joint arthrodesis in 0.4% (1/246) (Table 1).
Table 1: Reported ancillary procedures performed in conjunction with LCL utilizing a PTW. A Cotton osteotomy was performed most often with LCL. View Table 1
Four of seven studies reported no fixation for LCL titanium wedge stabilization [15-18]. Two studies utilized one or two 2.4 mm cortical screws for titanium wedge stabilization in all patients [19,20]. Another study discussed the placement of a lateral plate in conjunction with the LCL titanium wedge but did not discuss the number of patients or indications for this additional fixation [8]. The size of the graft(s) utilized was reported in 6 of 7 of the included studies [8,15-19] though two studies [15,16] reported a range of the graft size used, not individualized for each patient. Stamatos, et al. did not report the graft size used [20]. The size of the titanium wedge ranged from 4.5-12 mm with 8 mm being the most commonly reported graft size used (60 patients) [8,15-20].
Outcome measures were reported in three of the included studies [15-17]. The Foot and Ankle Ability Measure (FAAM) was reported in 99 patients and the Visual Analog Scale (VAS) pain score was reported in 71 patients. The FAAM Activities of Daily Living (ADL) score was measured post-operatively at 80.45 (80.0-80.9). Only Tsai, et al. reported preoperative values of FAAM ADL and Sports subscales at 56.0 and 31.25, respectively [15]. FAAM Sports subscale was measured post-operatively at 58.5 (50.0-66.9) (Table 2). The VAS pain score decreased from 5.45 (5.0-5.9) pre-operatively to 2.43 (1.6-3.0) post-operatively (Table 3).
Table 2: Outcome Measure - Reported FAAM ADL/Sport Subscale scores from included studies of patients undergoing LCL procedures with PTWs. View Table 2
Table 3: Outcome Measure - VAS Pain Score reported for patients undergoing LCL procedures with PTWs. View Table 3
The overall complication rate utilizing PTWs for LCL was found to be 15.2% (36/236). The reported complications from each study were further divided into major and minor complications. Major complications included non-union with or without reoperation due to non-union, development of deep infection, and chronic regional pain syndrome (CRPS). Major complications occurred in 5/236 (2.1%) of included patients. 4 patients (1.7%) went on to non-union of the titanium LCL wedge with 3 (1.2%) patients requiring revision surgery to address the non-union/painful hardware. Zero patients had a reported development of deep infection following surgery. One patient developed CRPS post-surgically. Minor complications included transient painful hardware, transfer pain, sinus tarsi syndrome, lateral column overload, lateral ankle pain, development of adjacent joint arthritis, and superficial wound complications. Minor complications totaled 31/236 (13.1%) of included patients. Of the minor complications, 2 developed painful hardware, 2 transfer pain, 6 sinus tarsi syndrome, 10 lateral column overload, 2 lateral ankle pain, 6 developed adjacent joint arthritis, and 3 superficial surgical wound complications which resolved with local wound care and oral antibiotics (Table 4).
Table 4: Reported complications with LCL procedures utilizing PTWs in reported studies included in systematic review. View Table 4
LCL is a tri-planar correction of the flexible flat foot deformity with realignment of forefoot abduction, collapse of the medial arch, and hindfoot valgus [19,21,22]. There have been numerous studies comparing the outcomes and complications of autograft versus allograft wedges used for LCL procedures [5-8] with autograft harvest from the iliac crest previously described as the “gold standard” [5]. In recent years, surgeons have been utilizing PTW grafts, rather than iliac crest autograft or allograft, in hopes of diminishing non-union rates and donor site morbidity [8,15-20]. There is currently a paucity of literature describing the outcomes and complications associated with LCL with PTWs.
In this review, the indication for LCL with a PTW was a flexible flat foot deformity for 100% (236/236) of the patients. LCL, as a joint-sparing procedure for flexible flat foot deformities, has shown favorable outcomes [1,23,24]. LCL procedures are often performed in conjunction with ancillary procedures to adequately address and correct the multiplanar flat foot deformity [1,14,23]. Across all included studies, a cotton osteotomy was found to accompany an LCL most often (n = 92), followed by tendon transfer (n = 65), MDCO (n = 51), PTT debridement (n = 32), spring ligament repair (n = 29), posterior muscle group lengthening (n = 22), medial column fusion (n = 7), etc.
Literature is limited in regard to outcome scores for LCL with PTW. Three of the seven studies in our systematic review included patient-reported outcome measures. Overall, preop VAS scores improved from 5.45 to 2.43 postoperatively, while postoperative FAAM ADL and Sports Score improved to 80.45 and 58.5, respectively. Only one study included preoperative FAAM ADL and Sports Scores of 56.0 and 31.25, respectively [15]. These outcome scores are similar to previously published literature on allograft wedges utilized for LCL. Colo,' et al. evaluated outcome scores following LCL utilizing a bony allograft wedge [25]. They found VAS scores improved from 7.7 ± 0.7 (7-9) preoperatively to 1.8 ± 1.6 (0-7) at final follow-up, while FAAM scores improved from 36.6 ± 6.2 (30-52) preoperatively to 71.8 ± 11.2 (25-84) at final follow-up.
Sequeira, et al. performed a retrospective case series on 54 patients undergoing LCL with titanium wedges, seeking to evaluate characteristics that correlate with poor functional outcomes [16]. They found an overall improvement in FAAM ADL and Sports scores postoperatively. However, they noted patients with a lower BMI and higher preoperative hindfoot valgus are potentially correlated with improved postoperative functional scores. Tsai, et al. performed a retrospective review of 45 patients undergoing LCL in combination with Cotton osteotomy [15]. They found significant improvement in all functional scores evaluated, including VAS pain, FAAM ADL, and FAAM sports. Thus, we found that postoperative outcome scores for LCL with PTWs are similar to the commonly utilized allograft wedges, while a higher BMI and lower preoperative hindfoot valgus may negatively influence these outcomes.
In general, numerous complications can occur with the LCL procedure. These can be secondary to the graft itself, such as non-union, dorsal displacement of the anterior process, over-correction leading to calcaneocuboid joint arthritis, or under-correction leading to recurrence of deformity. The complications can also be due to the dissection, such as sural neuritis or wound infection and dehiscence. Within our systematic review of titanium LCL wedges, our overall complication rate was 15.2% (36/236), with 5 (2.1%) major complications, and 31 (13.1%) minor complications. Among the 236 patients in this review, 4 patients (1.7%) demonstrated a non-union at the graft site. This rate is similar to the 1.4% non-union rate among 73 patients reported by Prissel, et al. among unfixed LCL procedures using allograft or autograft wedges [26]. Other studies have reported non-union rates of up to 15.4% [6,23,27].
The most common minor complications we encountered were sinus tarsi syndrome (2.7%), lateral column overload (4.2%), and development of adjacent joint arthritis (2.7%). Within the available literature on all LCL grafts, there is a correlation between larger graft sizes and the incidence of lateral column pain and CCJ arthritis [6,23,28-31]. The findings of this systematic review of PTW for LCL demonstrate a similar complication rate and similar non-union rate as previously published data on allograft or autograft wedges.
Outside of the clinical and functional patient evaluation, radiographic outcomes are used to discern the extent of correction obtained from the surgery performed. Various radiographic angles are used to determine the amount of flexible flatfoot correction in different planes, which can be compared between procedures. In this study, we chose not to evaluate radiographic outcomes due to the variability in reporting and the addition of concomitant procedures performed which could affect final measurements. However, we recognize the need for radiographic evaluation and its utility in the everyday evaluation of patients undergoing LCL.
A recent study by Stamatos and colleagues evaluated radiographic outcomes of the Evans procedure comparing titanium wedge versus allograft/autograft [20]. Ultimately, they found a significant improvement in all postoperative radiographic angles after the LCL procedure regardless of implant used. There was no difference in postoperative talonavicular coverage angle, incongruency angle, or calcaneal pitch between PTWs and autograft/allograft groups at 6 months and 1 year post-operatively, though there was a significantly higher talonavicular coverage angle in the titanium implant group preoperatively. Additional studies confirm improved radiographic outcomes after titanium wedge implant in LCL procedures for flatfoot deformity, especially in the talo-first metatarsal angle, talonavicular coverage angle, lateral talar-first metatarsal angle, metatarsal adductus, and calcaneal pitch [17,19]. We found it difficult to determine truly successful radiographic deformity correction of LCL with PTWs due to the number of reported adjunct procedures, though the above-mentioned outcomes are comparable to traditional graft options.
This systematic review evaluated the functional outcomes and complications associated with LCL using PTWs for the treatment of flexible flatfoot deformities. The use of PTWs appears to offer comparable functional results to traditional allograft or autograft wedges commonly utilized in LCL procedures. While the overall complication rate was found to be 15.2%, the majority of complications were minor and manageable, including issues such as painful hardware, lateral column overload, and sinus tarsi syndrome. Notably, the rate of non-union with the titanium LCL wedge was similar to rates reported for other graft materials. Additionally, the avoidance of autograft harvest from the iliac crest reduces donor site morbidity and operating room time.
Despite promising findings, it is important to acknowledge the limitations of this review, including the relatively small number of included studies and the variability in reporting radiographic outcomes. Additionally, when comparing outcomes to the traditional LCL grafting techniques, one has to consider the cost differences between PTW and traditional allogenic bone grafts. Data on this subject is limited and is likely institution-dependent. Tsai, et al. reports comparable costs between PTWs and allogenic bone graft [15]. We found similar results at our institution with the average cost of a PTW being $2,059 and average cost of pre-contoured LCL allograft wedges being $2,062. Gross, et al. report PTWs at a cost of $1000 compared to tricortical allograft, which costs, on average, $1125 [17].
Additional considerations include challenges encountered when having to revise the LCL into an arthrodesis or the options for revision surgery when a non-union is present. Bony loss with the removal of the PTW, arthrodesis, and fixation around the PTW are all issues that surgeons must account for prior to initial placement. PTWs, as opposed to allograft or autograft wedges, cannot be customized and or reshaped intraoperatively. Lastly, a majority of the patients included in this study had an adult stage II flexible flat foot deformity and there is little to no information with relationship to flexible pediatric or adolescent cases and the use of PTWS. Further studies with larger sample sizes and longer follow-up periods are warranted to confirm the long-term efficacy and safety of PTWs for LCL procedures.
In summary, the evidence from this systematic review suggests that LCL with PTWs can be an effective and viable option for correcting flexible flatfoot deformities. Surgeons should consider this technique as an alternative to traditional graft materials, given its potential advantages in maintaining deformity correction, reducing complications, and promoting Osseo integration. As the use of PTWs continues to evolve, it has the potential to contribute positively to the management of flexible flatfoot deformities and improve the quality of life for affected individuals. However, further research and ongoing evaluation are essential to fully understand the long-term outcomes and safety profile of this approach.
The authors report no funding or conflicts of interests applicable to this manuscript.