Clinical case: 24-year-old male with an initial diagnosis of first metatarsophalangeal (MTP) arthritis, on imaging tests the only abnormal findings were a bipartite medial sesamoid versus medial sesamoid fracture. During follow-up, patient developed fistulization of the first MTP with a positive culture for methicillin-sensitive Staphylococcus aureus (MSSA) and was diagnosed with septic arthritis (SA) of the first MTP joint. He was treated with surgical debridement and targeted antibiotic therapy, resulting in good outcomes and satisfactory progress.
Conclusion: Sesamoid bone pathology is uncommon, with fractures or sesamoiditis being the most common conditions. Acute or chronic infections (osteomyelitis) of sesamoids are very rare, and aggressive treatment is required. Sample collection should be performed to initiate targeted antibiotic therapy for the causative organism, with Staphylococcus aureus or Pseudomonas aeruginosa being the most common. Subsequently, broad surgical lavage and debridement should be carried out, aiming to avoid complete sesamoidectomy due to its significant comorbidity.
Sesamoid, Sesamoiditis, Septic arthritis, Osteomyelitis
A 24-year-old male was evaluated in the clinic due to swelling and pain in the right hallux of his foot that had been ongoing for two weeks, unrelated to any trauma or overexertion. He had no relevant personal medical history. The patient had previously been assessed at another medical center with a diagnosis of first MTP arthritis of unknown etiology. On examination, there was significant swelling of the hallux without warmth or redness in the area. It was painful upon movement, with no other significant findings. He provided plain X-rays and a magnetic resonance imaging (MRI) from a prior evaluation, which showed no pathological findings. Given the suspicion of monoarthritis, pain control with anti-inflammatory medication and a reverse-heeled shoe was recommended.
After three weeks, in addition to swelling, the patient exhibited redness and warmth in the hallux, with a significant improvement in pain. An MRI was repeated, which indicated a bipartite medial sesamoid versus medial sesamoid fracture, with signs of joint effusion (Figure 1).
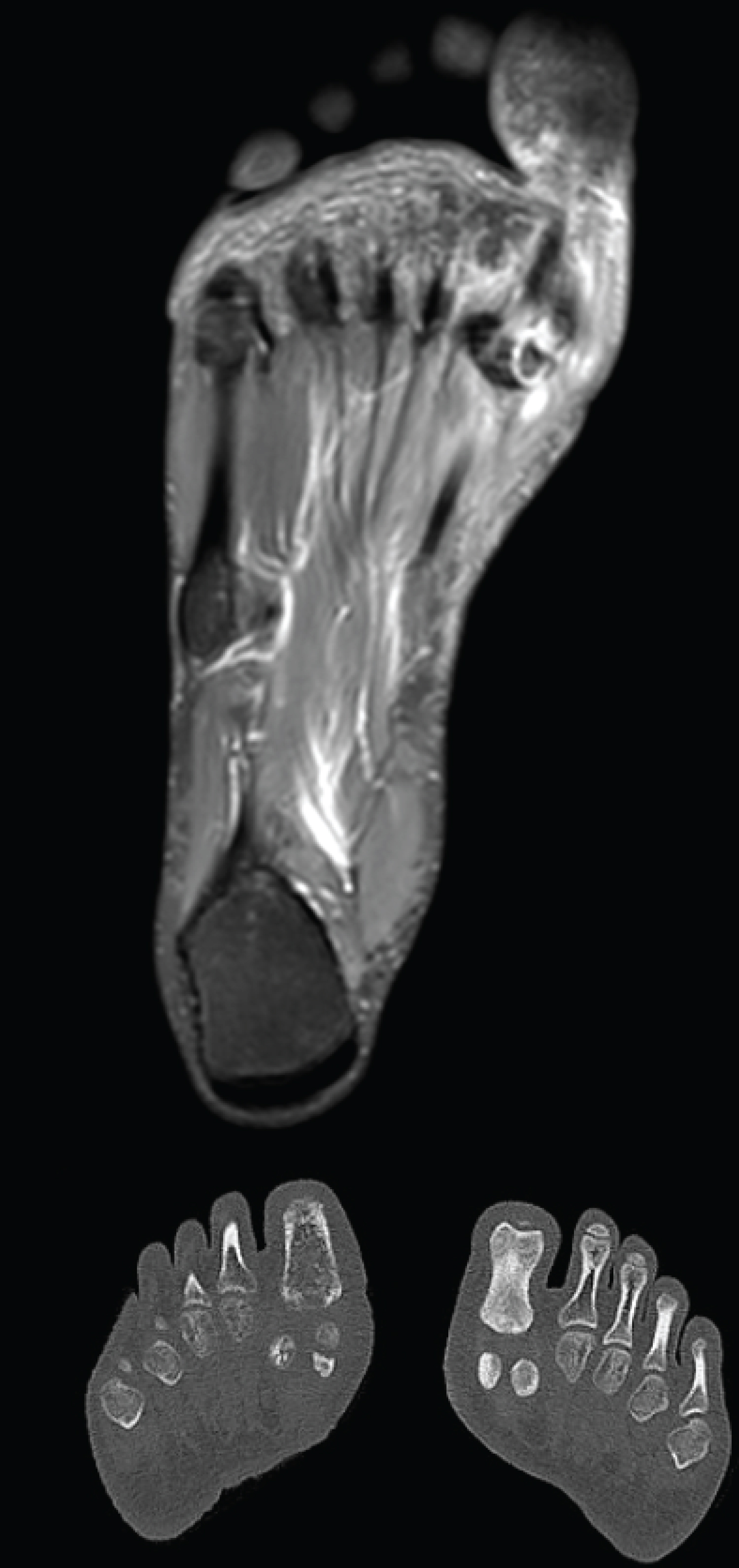 Figure 1: MRI showing a bipartite medial sesamoid versus a medial sesamoid fractura, with signs of joint effusion.
View Figure 1
Figure 1: MRI showing a bipartite medial sesamoid versus a medial sesamoid fractura, with signs of joint effusion.
View Figure 1
At five weeks from the onset of symptoms, the patient returned to the clinic with spontaneous fistulization of the hallux, accompanied by purulent drainage. Examination revealed erythema and redness in the area, with less swelling than before, and a fistulous tract on the medial and plantar aspect of the hallux actively discharging purulent material. Suspecting SA, a culture was obtained, and the patient was admitted for further evaluation with fistulography. The fistulogram revealed a 1-2 cm fistulous tract extending from the plantar, medial, and proximal aspects of the hallux to the medial sesamoid, with no communication to the lateral sesamoid or other structures, along with gas bubbles within the tract (Figure 2).
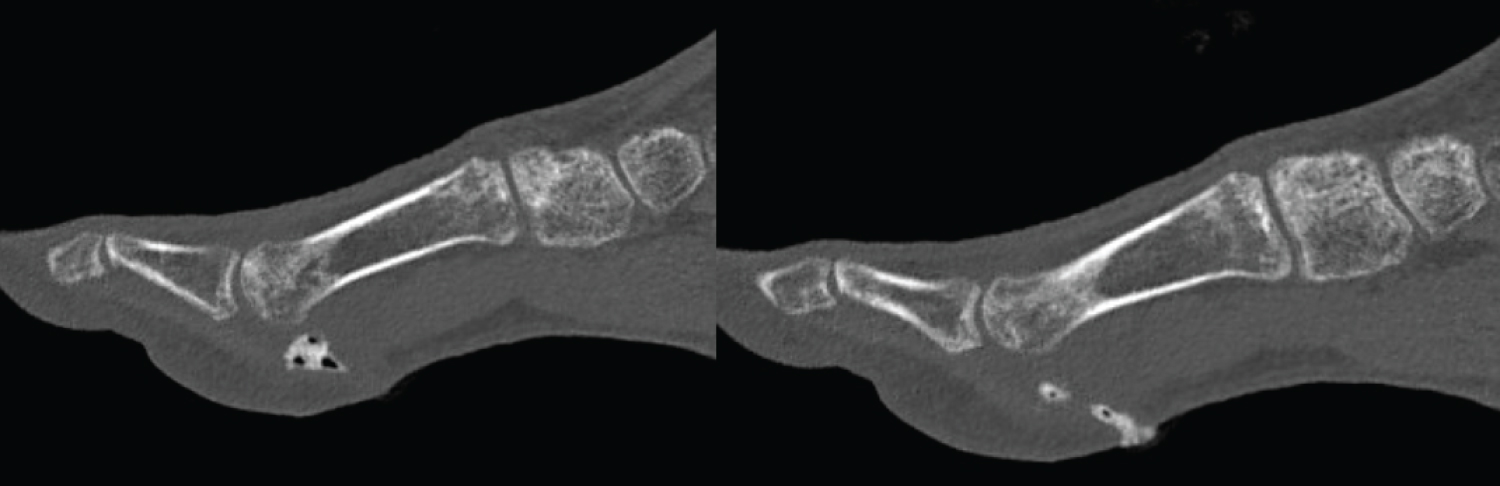 Figure 2: Fistulogram showing a 1-2 cm fistulous tract extending from plantar to the medial sesamoid, without communication to the lateral sesamoid, along with gas bubbles within the tract.
View Figure 2
Figure 2: Fistulogram showing a 1-2 cm fistulous tract extending from plantar to the medial sesamoid, without communication to the lateral sesamoid, along with gas bubbles within the tract.
View Figure 2
Due to the sesamoid infection, surgical intervention was performed, involving a plantar approach following the fistulous tract and a medial approach. Curettage, sample collection, and Friedrich's procedure at the edges were performed until achieving a bleeding and vitalized bed (Figure 3).
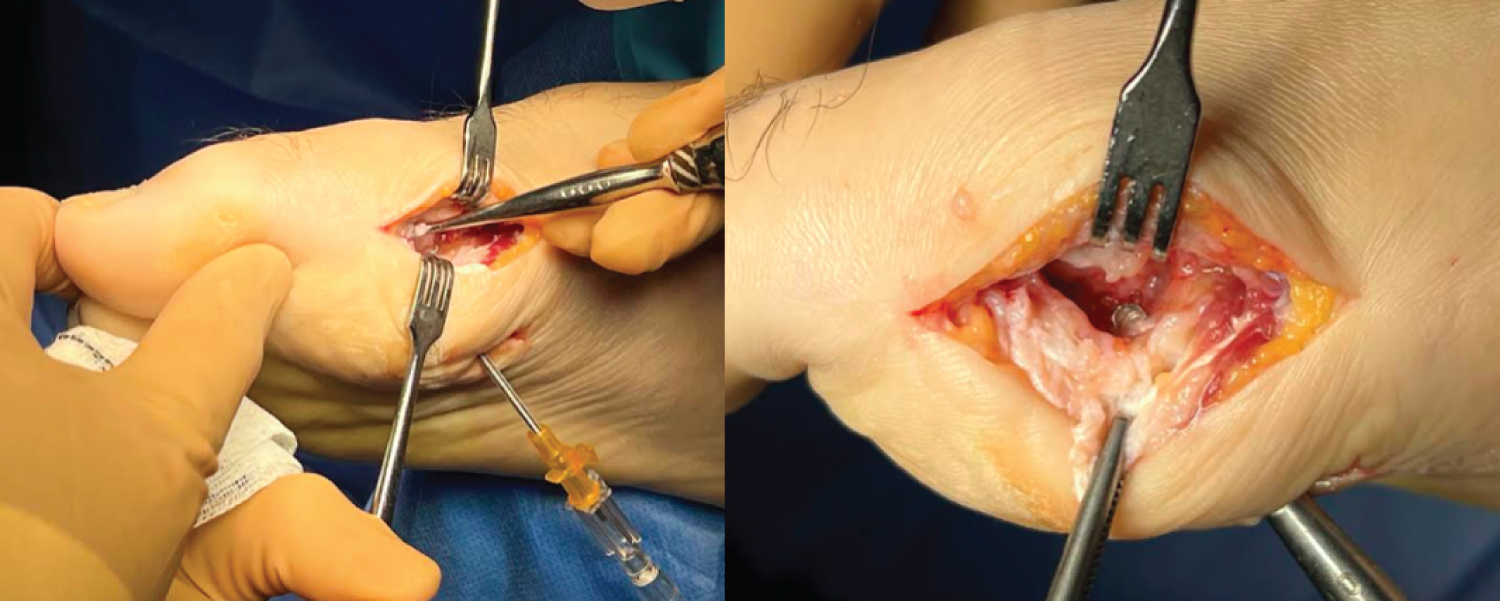 Figure 3: Surgical image showing the insertion of a cannula into the fistulous tract.
View Figure 3
Figure 3: Surgical image showing the insertion of a cannula into the fistulous tract.
View Figure 3
The culture results were positive for MSSA. Consequently, the patient received three weeks of targeted intravenous antibiotic therapy, followed by an oral regimen, as well as partial weight-bearing for 15 days until the wound closure.
After 6 months of follow-up, the patient has shown good progress, with no surgical wound complications or recurrence of the infection.
Sesamoid bones are of vital importance for the functioning of the foot. They are embedded within the tendon of the short flexor of the hallux [1], beneath the head of the 1 st metatarsal (MTT), facilitating its sliding, the flexion of the 1 st toe, and supporting the body's load [1-3].
Sesamoid bones ossify around 8 years of age in females and 12 years in males [4]. They may frequently develop bipartite morphology, with an incidence of 19-31% in the population [5,6], occurring bilaterally in 90% of cases [1,7].
Pathological conditions involving sesamoids are rare and diverse, including acute fractures (especially in the medial sesamoid) and stress fractures, ischemia (predominantly in the peroneal sesamoid) [1,8], due to their extraosseous and predominantly plantar vascularization [9], sesamoiditis, and acute or chronic infections (osteomyelitis), the latter being very infrequent [1,10].
The term sesamoiditis encompasses numerous conditions affecting sesamoids, including osteonecrosis, chondromalacia, or mechanical overload [9]. Initial treatment always involves conservative management [1] based on analgesia with anti-inflammatories and offloading.
Osteomyelitis of sesamoids occurs with equal incidence in both medial and lateral sesamoids, and it is a rare condition with only a few case reports in the literature [10,11]. It has two well-defined etiologies. Traumatic, which is more common, with Staphylococcus aureus and Pseudomonas aeruginosa as causative agents, often occurring in patients with a history of diabetes mellitus (DM) [11]. The hematogenous distribution origin, in which the pathogen is exclusively Staphylococcus aureus , is limited to paediatric and adolescent cases [10,12]. The onset of the condition is typically subtle, with mild pain and swelling in the area, tempting conservative management with antibiotics, immobilisation, and offloading. However, up to 83% ultimately require surgery [10].
SA in the foot joints is extremely rare, accounting for 3-7% of SA cases [13]. The tibiotalar joint and the 1 st MTP joint are the most affected [14]. Treatment should be based on prolonged antibiotic therapy [15,16] as soon as microbiological samples are obtained and aggressive surgical lavage/debridement [17-19]. Open or arthroscopic approaches can be used for purulent material lavage [15]. In the case of an open approach, the choice depends on the affected sesamoid, taking into consideration skin tension lines and allowing for proper visualisation of the sesamoid and flexor tendon. The most commonly used approach for the medial sesamoid is the plantar-medial, in which the medial plantar nerve is mobilised with the skin flap, while for the lateral sesamoid, a longitudinal plantar approach is employed [5].
Whenever possible, preservation of the sesamoid or a portion of it should be attempted due to the significant comorbidities associated with excision [5,20-22]: Hallux valgus/varus, claw toes [20,23], stiffness, transfer metatarsalgia, and neuromas [24,25].
Acute infections of the 1st MTP joint and sesamoid bones are an extremely rare condition with scarce literature describing it. Osteomyelitis in this location, although also infrequent, can be associated with direct trauma or hematogenous dissemination, especially in the paediatric and adolescent population. While the clinical presentation may initially be subtle, clinical suspicion and etiological diagnosis are crucial for initiating optimal treatment promptly. Targeted antibiotic therapy, combined with surgical debridement, achieves remission in up to 83% of cases. In cases of chronic infection, partial or complete sesamoidectomy should be considered to ensure complete healing.