The pattern of skin dermatoses in HIV infected individuals particularly children are associated with some factors. The type of skin dermatoses gives an insight on diagnosing HIV disease. This study was conducted to identify those factors among HIV infected children that are associated with the pattern of skin disorders among HIV infected children in Aminu Kano Teaching Hospital, Kano, Nigeria.
To assess the factors associated with pattern of skin disorders among HIV infected children in Aminu Kano Teaching Hospital Kano, Nigeria.
A cross-sectional study was conducted to determine the factors associated with pattern of skin dermatoses among HIV infected children attending Paediatric Infectious Disease Clinic of Aminu Kano Teaching Hospital, Kano, Nigeria. A total of 223 HIV infected children aged 6 months to 14 years were included in the study. Chi-square test or Fishers exact test where necessary were used to determine the difference between proportions of categorical variables and level of significance was set at 0.05. Binary logistic regression was used to further analyze significant relationships from the univariate analysis and the confidence interval was set at 95% and p < 0.05 was considered statistically significant.
A significant association was observed between low socio-economic class with Infections and infestations more specifically the bacterial skin infections. And an association between severe immunosuppression and fungal skin dermatoses was observed.
Therefore, there is an association between pattern of skin dermatoses among HIV infected children with their socioeconomic class and degree of immunosuppression.
Paediatric dermatoses, HIV infected children, Nigeria
Human immunodeficiency virus infection is a global health problem. HIV/AIDS was estimated to have infected more than 36 million people worldwide by the end of 2017 and 1.8 million among the infected people were children below 15 years most of whom are from sub-Saharsn Africa. In Nigeria, 220,000 children less than 14 years were infected with the HIV virus in 2017 [1].
Skin dermatoses are important in HIV infected children as they contribute to the risk of other life threatening illnesses like glomerulonephritis, sepsis, heart diseases and cancers [2,3]. The Skin is one of the early systems affected by HIV/AIDS and HIV/AIDS can affect all organs in the body [4].
Some factors such as degree of immunosuppression, sociodemographic factors and use of Antiretroviral drugs were found to be associated with pattern of skin dermatoses among HIV infected children by some authors [5-7].
In a study by Wannukul, et al. [5], 91 HIV infected children were recruited into the study they found that sebourrehic dermatitis was associated with mild immunosuppression. While oral thrush, drug reaction, pruritic papular eruption, cutaneous candidiasis, herpex simplex stomatitis were associated with moderate and severe immunosuppression. And cellulitis, molluscum contagiosum and dermatophytosis were found to be associated with moderate immune suppression. Penicillium marneffei was associated with severe immunosuppression.
Umoru, et al. [6] in Benin City, Nigeria, studied 100 HIV infected children and observed a significant association between pruritic papular eruption (PPE) and severe immunosuppression. Infections and infestations were more common among those with severe immunosuppression. Pityriasis versicolor and Acne were seen among those with no immunosuppression.
Endayehu, et al.. [8], found that non-infectious dermatoses were more prevalent among those aged greater than 5 years (46.4%), compared with those less than 5 years (35.5%). While infectious dermatoses were commoner among those less than 5 years (96.4%) compared with 78.8% among children 5-10 years and 81.4% among those > 10 years.
Nagendran, et al. [7] in India, studied the effect of antiretroviral therapy on mucocutaneous manifestations among 170 HIV infected patients irrespective of gender or age and observed that the advent of HAART had significantly altered the pattern of mucocutaneous manifestations. The prevalence of both infectious and inflammatory dermatoses had also reduced with the use of HAART; however, they observed an increased incidence of adverse cutaneous drug reactions.
There is paucity of data concerning the factors affecting pattern of skin disorders among HIV infected children in Northern Nigeria.
To determine the association between degree of immunosuppression and pattern of skin dermatoses among HIV infected children attending paediatric infectious disease clinic in AKTH.
To determine if there is an association between socio-demographic factors such as age, gender, socio-economic status and the pattern of skin dermatoses among children attending paediatric infectious disease clinic in AKTH.
To determine the effect of use of Anti-retroviral drugs on the pattern of skin dermatoses among HIV/AIDS infected children attending paediatric infectious disease clinic in AKTH.
It was a cross-sectional study to determine the factors associated with pattern of skin dermatoses among HIV infected children Aged 6 weeks to 14 years attending paediatric infectious disease clinic of AKTH.
Two hundred and twenty-three HIV infected children were recruited into the study using a systematic sampling method after obtaining an Ethical clearance from Ethical and Research Committee of Aminu Kano Teaching Hospital as well as Informed consent from the parents and verbal assent from children aged > 7 years. Confidentiality was ensured. Children who refused a physical examination and Children who have malignancies children whose HIV status has not been disclosed to them or those who have been on steroids for a long period (more than one month) and those on cytotoxic drugs were excluded from the study.
The study was conducted between 10th July and 20th October 2017. The investigator used a pre-tested interviewer administered questionnaire to collect the data.
A complete dermatological examination of the hair, scalp, trunk, nails, oral mucosa, genitalia and extremities and a complete physical examination of all systems were carried out on each child in a well-lit room after adequate exposure of the patient by the investigator to identify all the possible skin lesions. A chaperon was used for examination of the children. A picture of each lesion was taken. Most of the diagnoses were made clinically. Lesions requiring further evaluation and treatment were referred to the dermatology clinic of the Aminu Kano Teaching Hospital while those with readily treatable conditions had drugs prescribed.
Rapid HIV antibody testing by determine® method, PCR, CD4+ count, and Full blood count were retrieved from the subject’s record. Current CD4+ count done about 3 months before the study recruitment period was used.
The data was entered into a statistical package for the social sciences SPSS version 24 which was used to generate frequency tables and charts. Differences between proportions of categorical variables were evaluated using the Chi-square test or the Fisher exact test (where necessary).
The confidence level was set at 95% and a p-value less than 0.05 was considered statistically significant. Binary logistic regression was used to further analyse significant relationships from the univariate analysis and the confidence interval was set at 95% and p < 0.05 was considered statistically significant.
Two hundred and twenty-three HIV infected children aged 6 weeks to 14 years were enrolled. The mean age ± standard deviation of the HIV-infected children was 84.68 ± 40.34 month. There were 110 males (49.3%) and 113 females (50.7%) HIV positive children. Male to female ratio 1:1.1.
There was no significant association found in types of skin disorders based on age group or gender. This is shown in Table 1 and Table 2.
Table 1: Types of skin disorders in HIV infected children among various age groups. View Table 1
Table 2: Types of skin disorders in HIV infected children and sex. View Table 2
However, Table 3 shows that infections and infestations were significantly associated with socioeconomic status among HIV-infected children (χ2 = 10.60, p value 0.005) and there is an association between bacterial skin disorders and socioeconomic class (χ2 = 6.51, p value 0.04), moreover, Table 4 shows an association between fungal skin infection and immune status (χ2 = 6.97, p value 0.03).
Table 3: Types of skin disorders in HIV infected children and socioeconomic class. View Table 3
Table 4: Types of skin disorders in HIV infected children and degree of immunosuppression. View Table 4
Dermatophytoses were the commonest skin lesion found in all age groups. This is illustrated in Figure 1.
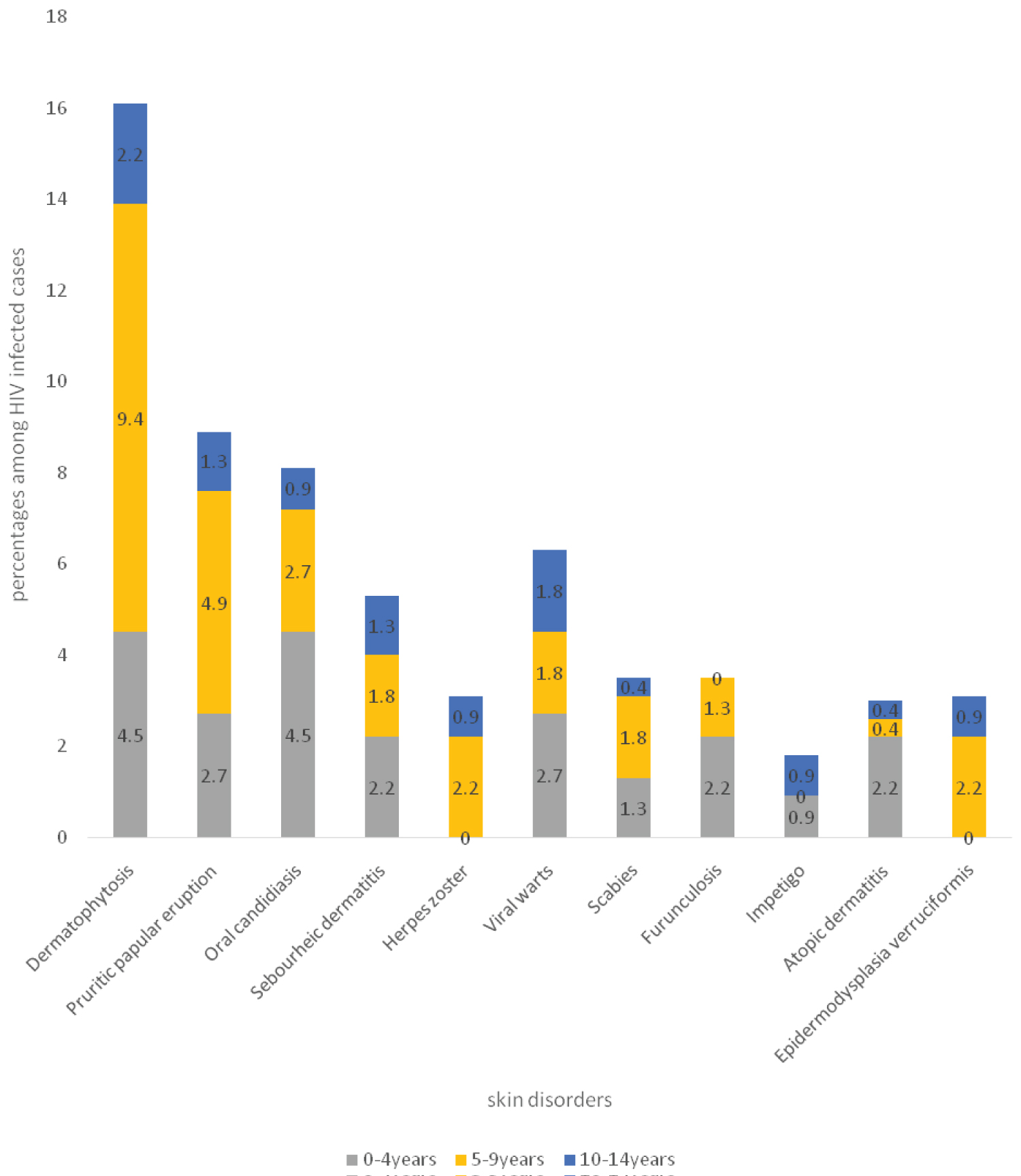 Figure 1: Comparison of types of common skin disorders among different age groups.
View Figure 1
Figure 1: Comparison of types of common skin disorders among different age groups.
View Figure 1
Dermatophytoses (9%), oral candidiasis (4.5%), and pruritic papular eruptions (4.9%), Epidermodysplasis verriciformis (1.8%), herpes zoster (2.2%) and impetigo (1.8%) were commoner among males, while furunculosis (6.7%) and atopic dermatitis (2.7%) were commoner among females. This is illustrated in Figure 2.
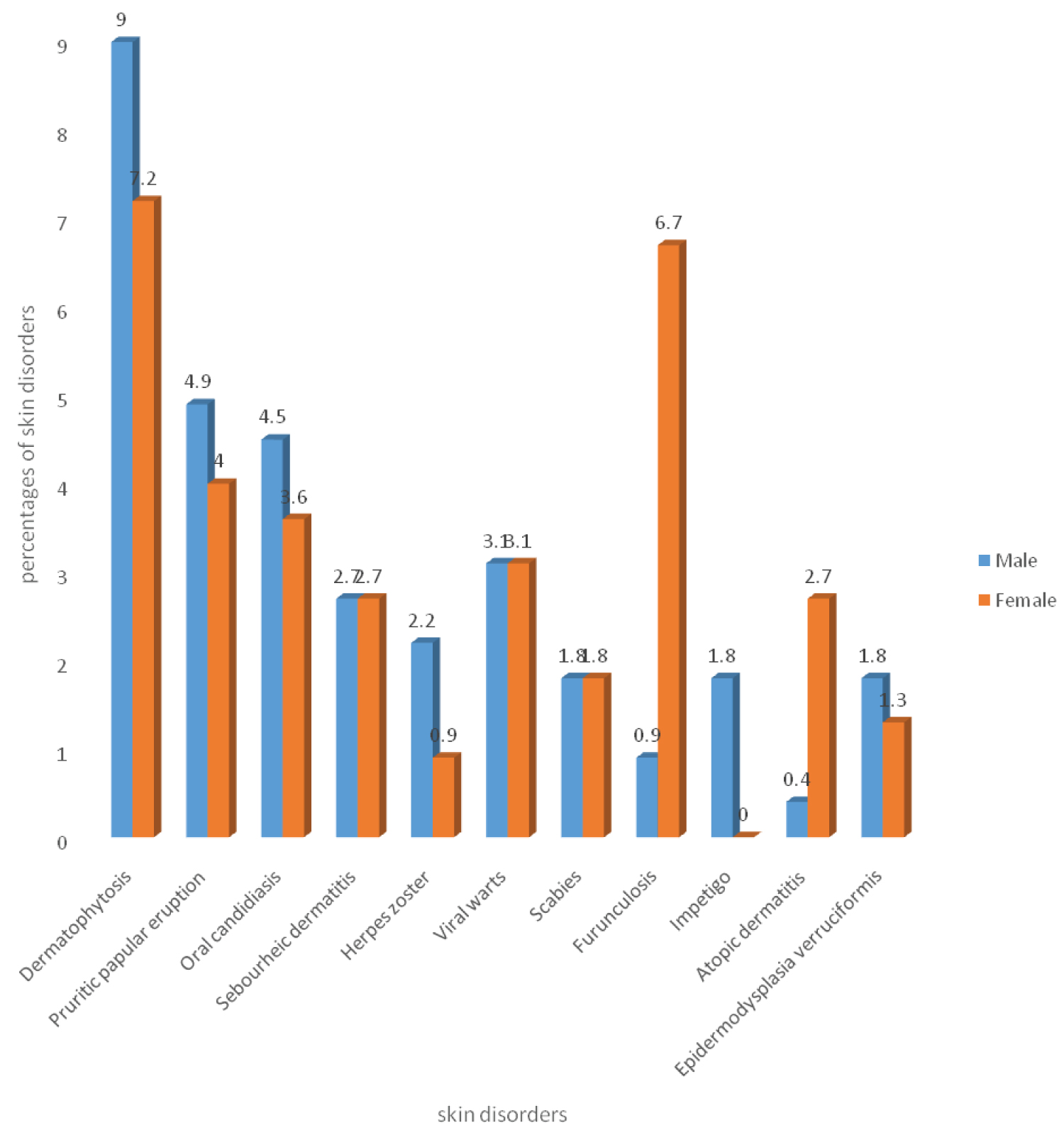 Figure 2: Comparison of types of common skin disorders with gender.
View Figure 2
Figure 2: Comparison of types of common skin disorders with gender.
View Figure 2
Pruritic papular eruption (6.3%), oral candidiasis (4.9%), seborrheic dermatitis (2.7%) were commoner among subjects from low socioeconomic class. Dermatophytoses (6.7%), viral warts (3.6%), epidermodysplasia verruciformis (1.8%), and herpes zoster (1.3%) were commoner among subjects from middle socioeconomic class. Impetigo (0.9%) was commoner among subjects from upper socioeconomic class. This is shown in Figure 3.
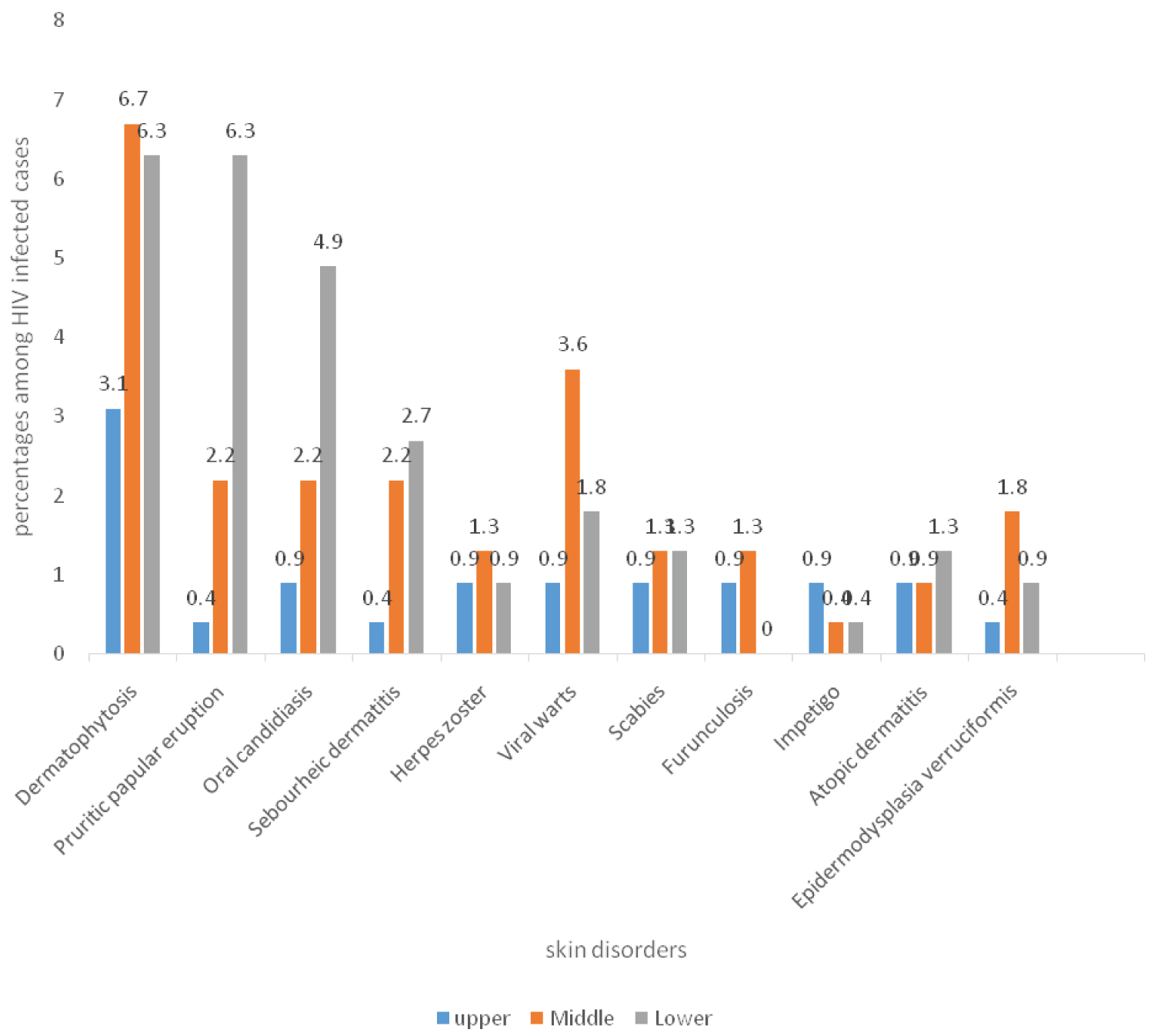 Figure 3: Comparison of types of common skin disorders and socioeconomic class.
View Figure 3
Figure 3: Comparison of types of common skin disorders and socioeconomic class.
View Figure 3
As shown in Figure 4, all forms of observed skin disorders were commoner among subjects with severe immunosuppression followed by those with moderate immunosuppression. Atopic dermatitis was equally common among those with severe and moderate immunosuppression.
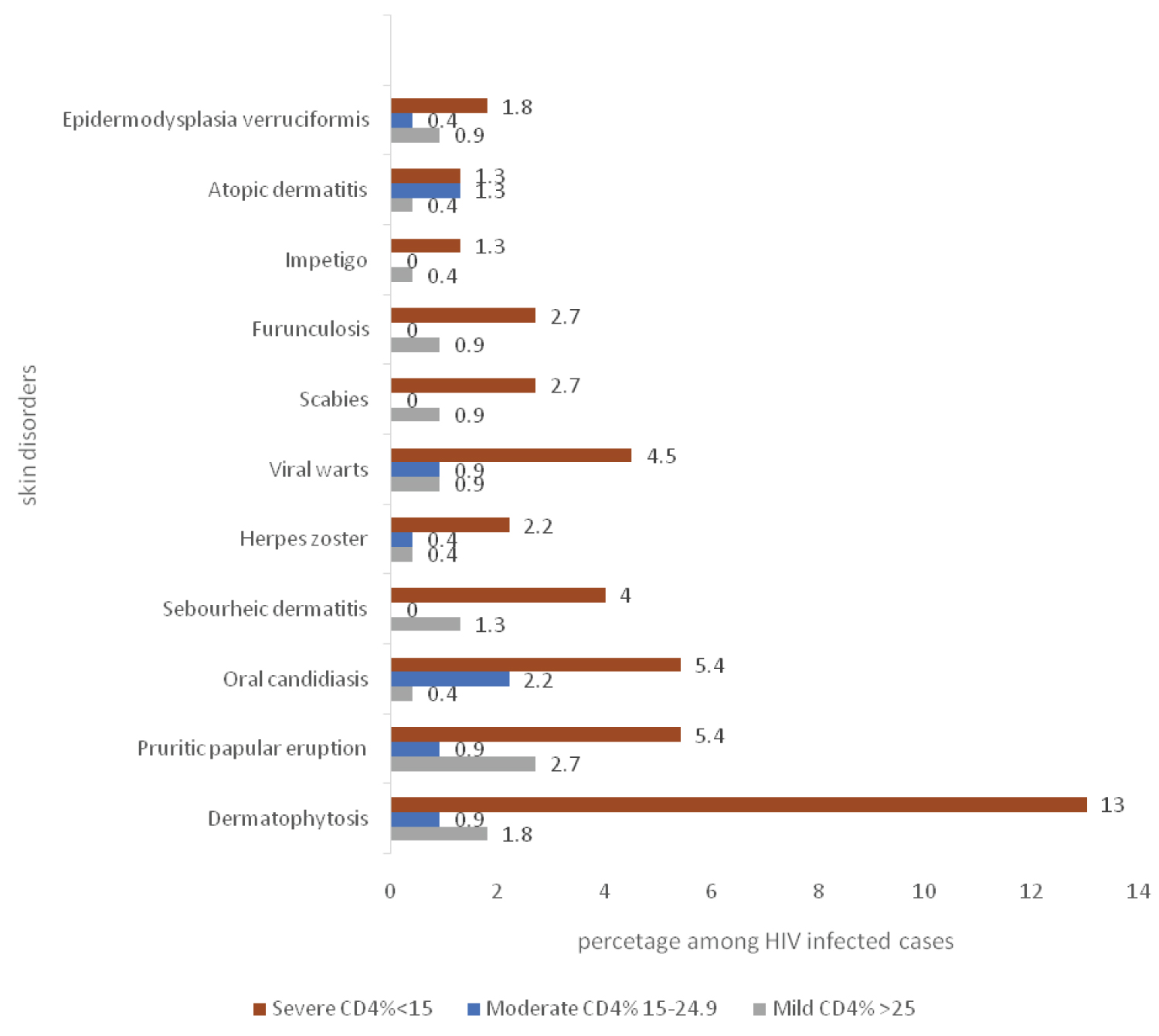 Figure 4: Common skin disorders and immune status.
View Figure 4
Figure 4: Common skin disorders and immune status.
View Figure 4
This study showed no significant difference in the types of skin disorders among HIV-infected children of different ages or gender, but there was significant association observed in this study between infections and infestations and low-socioeconomic status. It was not possible to make comparisons, because there were no studies found in the literature evaluating different types of skin lesions among HIV-infected children in relation to socioeconomic status. Several studies conducted among normal children whose HIV status were not considered have linked low socioeconomic status with the increased prevalence of certain skin disorders due to e.g. poor skin hygiene and sharing of personal items which is common among those from low socioeconomic class and low socioeconomic class was found to be significantly associated with the occurrence of some skin disorders, especially infections and infestations [9,10].
Dermatophytoses were commoner among males aged 5-9 years and those from middle and low socieconomic class and those with severe immunodeficiency in this study. This is similar to findings by Katibi, et al. [11] in Ibadan, Nigeria. This could be because the age range for the study population (6 weeks-14 years) used in this study and Ibadan study was similar. Dermatophytoses are frequently seen in HIV infected children especially those with low CD4 cell counts [12].
Pruritic papular eruption was commoner among children aged 5-9 years, males, those from low socioeconomic status and those with severe immunosuppression. The findings in this study differ from findings by Panya, et al. [13] in Tanzania, who reported PPE to be comparable among all ages and sexes and commoner among those with severe immuno suppression. Okechukwu, et al. [14] in Abuja, Nigeria also reported pruritic papular eruption as commoner among those with severe immunosuppresion. This difference could be as a result of different environmental conditions of the study sites from that in this study.
PPE is believed to be a form of hypersensitivity reaction of the skin to demodex folliculorum mite which is a normal commensal of the hair follicle. The distortion of the immune system is also responsible for it being frequently encountered among HIV infected people along with other non-infectious Dermatoses [15].
Oral candidiasis was found to be commoner among HIV infected children 0-5 years, male, those from low socioeconomic class and those with severe immunosuppression were more affected. This differs slightly from findings of Umoru, et al. [6] in Benin city, Nigeria who found oral candidiasis to be more among males and those aged 5-9 years, and those with severe immunosuppresion. This study enrolled both old and new cases most of whom were on ART, while Umoru, et al. [6] recruited only new cases who had not started any treatment which perhaps resulted in the differences observed in the two studies. The duration of ART theraphy among the HIV infected children in this study (48% of the subjects were on ART for six to twelve months) may also be a contributing factor to the differences observed. Oral candidiasis may represent onset of severe immunosuppression among HIV infected subjects and can progress to involve the oesophagus or even become systemic [16].
Viral wart was found to be commoner among children aged 0-5 years (2.7%), commoner among those from middle socioeconomic class (3.6%) and those with severe immunosuppresion (4.5%). No gender difference in frequency of its occurrence was observed. Smith, et al. [17] found viral warts to be associated with early stages of HIV disease different from what was found in this study. The difference may be because this study was among HIV infected children while Smith, et al. [17] recruited both children and adults in their study. Plane warts, and mucosal warts were the forms found in this study. Extensive plane warts have previously been described in the context of HIV [17]. However, reports have demostrated that viral warts can be seen in all stages of the HIV disease and is not associated with disease progression [18].
This study was not able to assess the effect of ART use on the pattern of skin disorders among HIV infected children as 98.0% of the subjects were on ART according to the current National guideline for treatment of HIV infected people.
Socio-economic status and degree of immunosuppression are the factors found to be associated with the pattern of skin disorders among HIV infected children in this study.
No conflict of interest.