Lymphangiomas of the ovary are unusual benign tumours characterised by proliferation of lymphatic channels, composed of cystic spaces lined by a single layer of endothelial cells. We present a case of 61-year-old woman who presented with complaints of pain abdomen. Investigations revealed a large left ovarian multiseptate multiloculated cystic mass extending to pelvis, abdominal cavity and infraumbilical region likely neoplastic. Total abdominal hysterectomy with bilateral salpingo-oophorectomy was performed suspecting malignancy. Histopathological examination revealed an ovarian lymphangioma. Patient was disease free 1 year post-surgery. Ovarian cystic lymphangiomas must be included in the differential diagnosis of cystic ovarian masses and long term follow up is suggested to exclude a possibility of malignant transformation.
Cyst, Histopathology, Lymphangioma, Ovary
Lymphangiomas are benign and slow-growing tumours of the lymphatic system [1]. They are characterised by lymphatic proliferation and composed of multiple cystic spaces lined by single layer of flattened endothelial cells, which are separated by fibrocollagenous septae. They can be differentiated according to the size of lymphatic vessels into capillary, cystic, or cavernous and contain either serous or chylous fluid [2,3]. Lymphangiomas may appear anywhere in the body most common being head, neck and axillary regions in children, the superficial skin and intra-abdominal sites in adults. Visceral lymphangiomas are infrequent [4]. Lymphangioma of the ovary is an extremely rare condition which is usually asymptomatic for a long time and is most often encountered incidentally. Some occasionally grow large enough to present symptomatically with lower abdominal pain and mass effect. The clinical and radiological findings are non-specific and are often confused with a malignant ovarian mass. Hence histological assessment is mandatory for a definitive diagnosis.
A 61-year-old post-menopausal woman complaints of pain abdomen of 6 weeks duration. There were no other complaints or significant past history. General examination was unremarkable. Ultrasound whole abdomen showed a large pelvic and abdominal multiloculated cystic mass with eccentric solid tissue in the mid pelvis slightly inclined to the right side measuring 14.6 × 10.2 cm. There was no demonstratable vascularity within the lesion. CT abdomen showed a large multiloculated and multiseptated cystic mass measuring 13.2 × 12.18 × 11.5 cm involving the pelvic cavity and adnexa extending into the abdominal cavity up to infraumbilical region. On imaging, the features were suggestive of a left ovarian complex cyst - likely neoplastic. Serum tumour markers (CA125, Beta hCG and Alpha fetoprotein) were within normal limits. Other systemic examination did not reveal any significant pathology. There was no evidence of lymphadenopathy or lymphatic obstruction. In view of radiological diagnosis of a neoplasm, patient underwent total abdominal hysterectomy with bilateral salpingooophorectomy. On gross examination, left ovarian mass measured 14 × 13 × 10.5 cm. Cut surface was multiloculated with varying sized cysts filled with straw colour fluid, most of which were less than 1 mm but few of them were up to 4 mm. Right ovary, bilateral fallopian tubes and rest of the uterus were macroscopically normal. Histopathological examination of the left ovarian cystic mass revealed multiple varying sized dilated vascular channels lined by a single layer of flattened endothelial cells without any atypia or hyperchromasia. There were no mitoses or necrosis. The vascular lumen was filled with lymph fluid separated by thin intervening fibrous stroma (Figure 1). Right ovary, bilateral fallopian tubes, rest of the uterus and bilateral pelvic lymph nodes were unremarkable microscopically too. Provisional diagnosis was Lymphangioma. The vascular nature of lymphangioma can be determined by endothelial markers such as CD-31, CD-34, Factor VIII-related antigen, FLI-1 and D2-40. D2-40 is a specific marker for lymphatic endothelium and hence has been used in the present case for confirmation (Figure 2). Adjuvant chemotherapy or radiotherapy was not given since lymphangioma is a benign lesion. Patient was disease free 1year post-surgery.
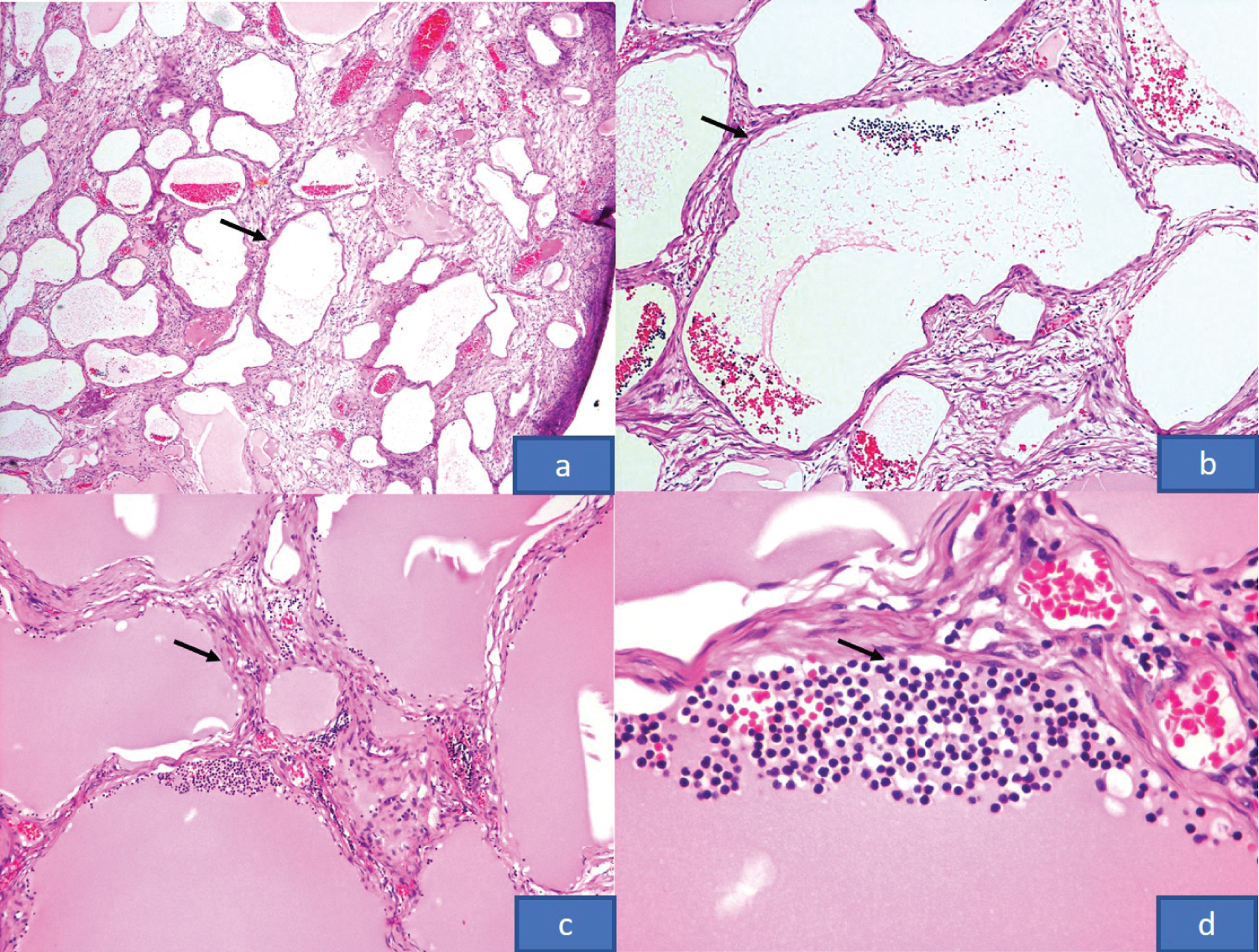 Figure 1: (a, b) Multiple cystic spaces within the ovarian stroma (H&E x40, x100); (c, d) Lymphatic channels lined by a single layer of endothelial cells, lumen filled with lymph fluid and lymphocytes (H&E x100, x400).
View Figure 1
Figure 1: (a, b) Multiple cystic spaces within the ovarian stroma (H&E x40, x100); (c, d) Lymphatic channels lined by a single layer of endothelial cells, lumen filled with lymph fluid and lymphocytes (H&E x100, x400).
View Figure 1
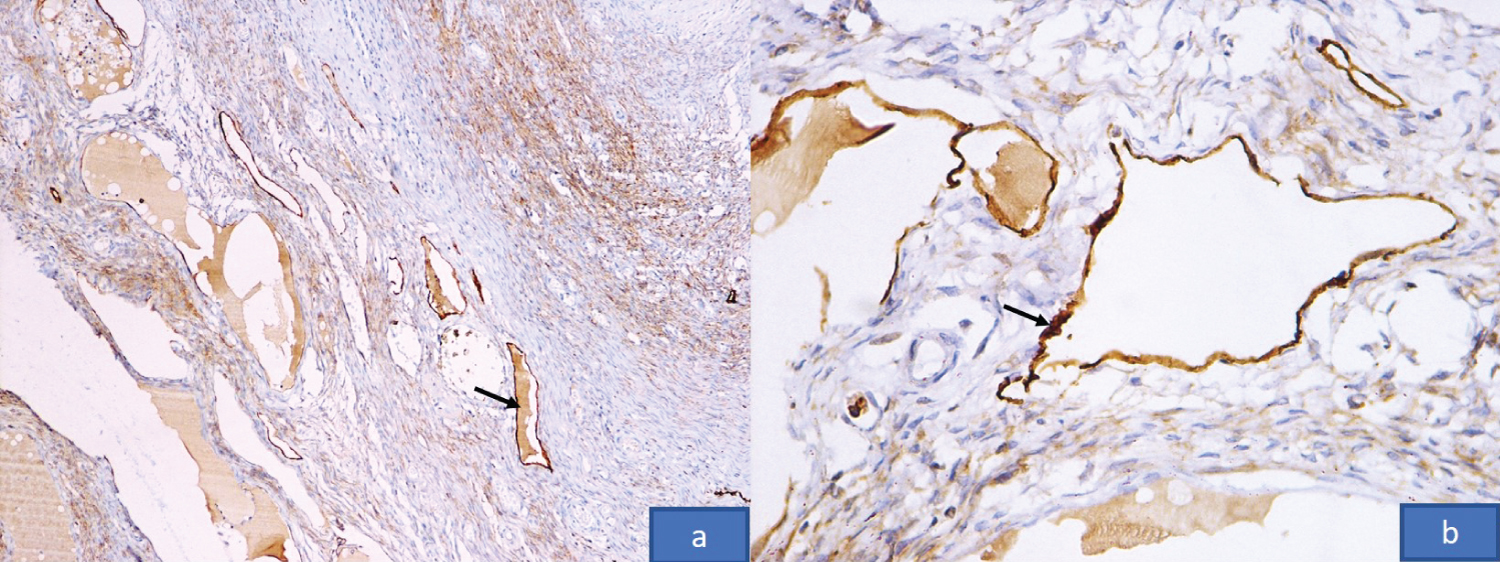 Figure 2: Immunohistochemistry with D2 40 highlighting the endothelium of lymphatic channels (x100, x400).
View Figure 2
Figure 2: Immunohistochemistry with D2 40 highlighting the endothelium of lymphatic channels (x100, x400).
View Figure 2
The lymphatic system comprises of a network of uni-directional lymphatic vessels that carry clear fluid called lymph directed towards the heart [5]. The lymphatic vessels are found throughout the body sparing the brain, anterior chamber of the eye and in organs composed of rich sinusoidal networks such as bone marrow and spleen. Lymphangiomas are benign lesions of the lymphatic system and are rare [6] that most commonly involve head, neck and axillary regions. In children, they occur due to congenital malformation of the lymphatic system. Visceral lymphangiomas are very rare and mostly present in intestine and mesentery. Lymphangioma of the ovary is an extremely rare entity. It was first described by Kroemer in 1908 [6]. Due to the rare occurrence of ovarian lymphangioma, little is known about its pathogenesis. However, few hypotheses have been put forward. Some authors suggest that it is a hamartomatous process due to sequestration of lymphatic tissue during embryonic development, while others believe that they are true neoplasms. There can be a variety of causes for acquired lymphangiectasia leading to lymphangioma such as inflammatory and genetic factors, degeneration of lymph nodes, mechanical pressure, trauma, and radiation therapy. In our case, there was no such history; therefore, it suggests a hamartomatous or a neoplastic aetiology.
Lymphangiomas are composed of multiple closely packed thin walled vascular spaces lined by widely spaced flattened endothelial cells containing lymphocytes and pale eosinophilic material in the lumen called lymph. The stroma also contains lymphocytic aggregates.
In our case, the differential diagnoses considered were Hemangioma, Teratoma and Adenomatoid tumour. The histological appearance of lymphangioma is similar to hemangioma but the latter has more red cells within the vascular lumen, lined by continuous endothelial cells and lack lymphocytes within the wall. The absence of other elements in the present case ruled out the possibility of a teratoma with a prominent vascular component. Adenomatoid tumour is a benign solid tumour of mesothelial origin affecting both male and female genital tracts. This tumour is composed of cystic spaces lined by continuous cuboidal or flattened mesothelial cells and do not contain lymphocytes in the stroma. Immunohistochemically, it is positive for cytokeratin (HMW), calretinin and negative for endothelial markers, while the opposite is true with lymphangioma.
Malignant transformation in a lymphangioma is extremely rare. Studies in past like Rice et al. [7] and Aristizabal et al. [8] have described Lymphangioma with rare malignant counterparts. Aristizabel et al. [8] described a peritoneal lymphangioma which recurred twice within two years, hence radiation was given to control the disease. Rice et al. [7] described a benign ovarian lymphangioma which recurred within 6 months with involvement of contralateral ovary, liver metastasis and diffuse peritoneal involvement. Patient had succumbed to the illness. Histopathological examination showed plump endothelial cells with hyperchromasia, necrosis and haemorrhage. These examples suggest that histology is not an absolute indicator of the subsequent behaviour. Complete wide excision with clear margins and a close follow up for at least two years is mandatory.
This case is presented to highlight the importance of considering lymphangioma in the differential diagnosis of a multicystic lesion of the ovary. Its diagnostic confirmation is solely based on histopathological examination and immunohistochemical confirmation. Even though malignant transformation is rare, complete surgical excision and regular follow up is mandatory.