Aggressive angiomyxoma are rare myxoid soft tissue neoplasms, affecting the pelvis and the perineum, rarely encountered in extragenital sites, with a marked preponderance for females in the reproductive age group. AAMs are thought to be benign, locally infiltrative and non-metastasizing. Here is case report of AAM located in the posterior chest wall.
50-year-old female presented with complaints of swelling over the back since 1 year. Insidious in nature, clinically suspecting lipoma.
MRI done gave an impression of cystic lesion likely to be a sebaceous cyst.
Following surgical excision we received a circumscribed mass with a smooth and slightly lobulated outer surface. Cut surface showed a poorly circumscribed myxoid and glistening tumor. Based on the histopathological features, radiological features and intraop finding a impression of angiomyxoma was done. One year follow up so far has showed no signs of recurrence.
Extragenital angiomyxomas are rare mesenchymal tumors. These lesions are classified as aggressive angiomyxomas, superficial angiomyxomas and angiomyofibroblastomas.
AAM needs to be differentiated microscopically from superficial angiomyxomas, fibroepithelial polyps, angiomyofibroblastomas, other myxoid tumors. The clinicopathological features, along with the immunoreactivity, help in the diagnosis.
AAMs are rare slow growing tumours with a high recurrence rate, seen almost exclusively in the pelvi-perineal region. The present case is unique in being located in the posterior chest wall. A histopathological examination, combined with radiological correlation, helped in distinguishing these lesions from the more commonly occurring similar entities, when they are located in sites other tan genital regions.
AAM: Aggressive Angiomyxoma
Aggressive angiomyxoma are rare myxoid soft tissue neoplasms which primarily affect the pelvis and the perineum and are rarely encountered in extragenital sites [1].
This tumour has a marked preponderance for females who are in the reproductive age group [2].
The aggressive angiomyxomas are thought to be benign, locally infiltrative and non-metastasizing.
Though common to the genital sites very few cases have been reported in the literature. Even fewer cases are reported in the extragenital sites, specially in the post menopausal age group.
Here is case report of AAM in the posterior chest wall encountered in an older woman.
A 50-year-old female presented with complaint of swelling of the back since 1 year, insidious in onset and gradually progressive in nature. On local examination swelling in interscapular region measuring 7 × 5 cm, smooth surface, no visible pulastions and was soft inconsistency. Radiological investigations implied it to be cystic lesion (Figure 1).
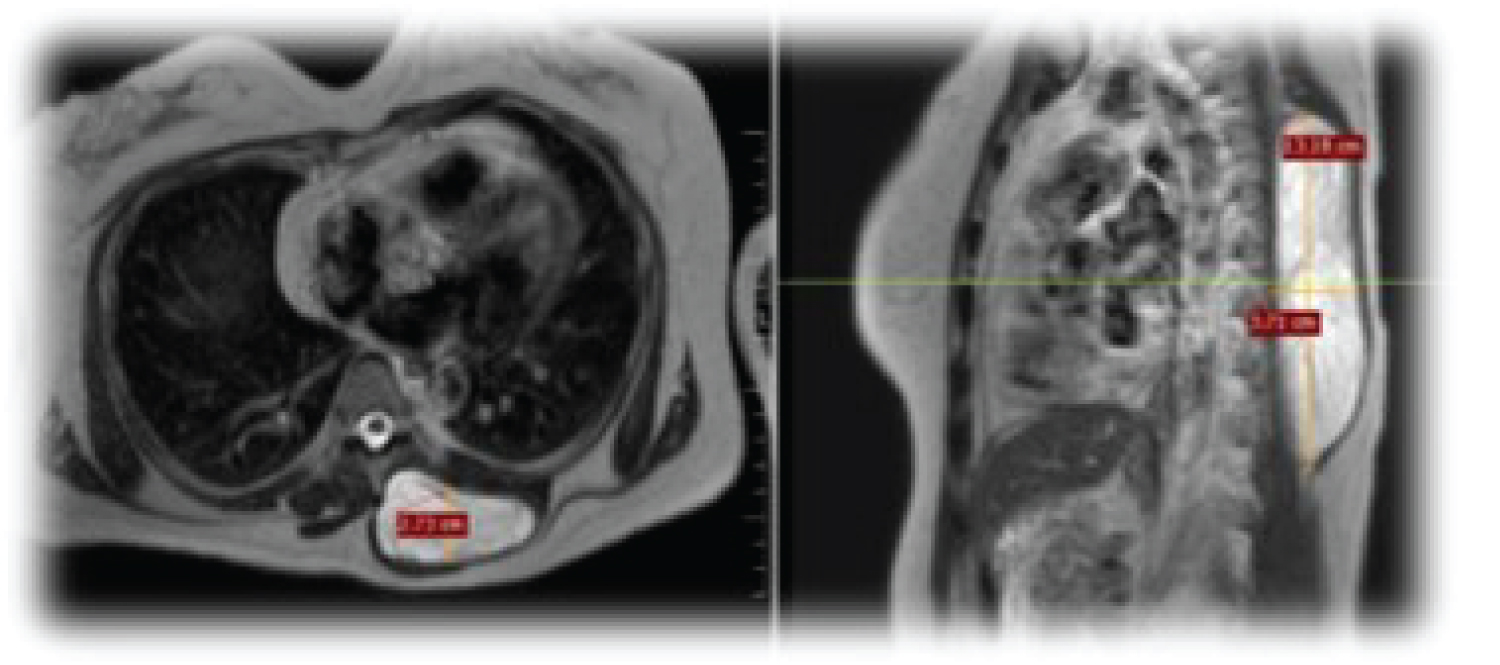 Figure 1: MRI: T1 hypointense, T2 hyperintense cystic lesion with multiple sepations and peripheral contrast enhancement seen in posterior chest wall. Likely epidermoid/sebaceous cyst.
View Figure 1
Figure 1: MRI: T1 hypointense, T2 hyperintense cystic lesion with multiple sepations and peripheral contrast enhancement seen in posterior chest wall. Likely epidermoid/sebaceous cyst.
View Figure 1
Patient underwent excision under general anesthesia and the gross specimen for sent for histopathological examination (Figure 2).
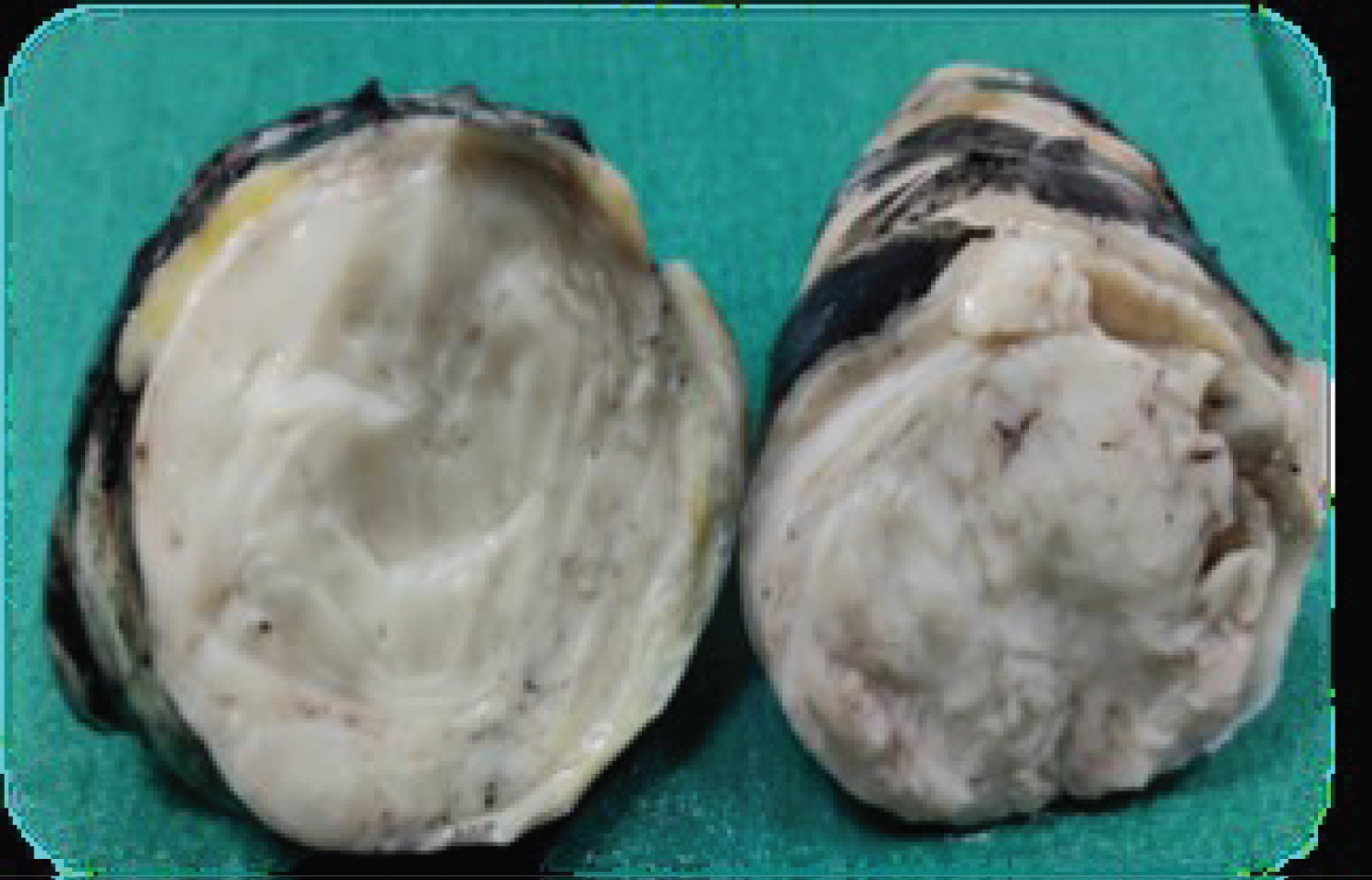 Figure 2: Smooth, lobulated mass measuring 11 × 6.5 × 3.5 cm.
Figure 2: Smooth, lobulated mass measuring 11 × 6.5 × 3.5 cm.
C/S: Circumscribed, unencapsulated, homogenous, solid and myxoid lesion.
View Figure 2
Grossly it was a smooth, lobulated mass measuring 11 × 6.5 × 3.5 cm. Cut surface revealed an unencapsulated, circumscribed tumor which was solid, homogenous with a myxoid and glistening appearance.
Microscopic examination showed an unencapsulated hypocellular lesion entrapping the adjacent adipose tissue. It shows two components, one with spindled cells with spindled and stellate bland nucleus in a myxoid background, also rich in collagen fibres. The other component is of the vessels of different calibres, some of them showing hylinization (Figure 3a, Figure 3b and Figure 3c). These morphological features and deep location and gross findings point towards a diagnosis of aggressive angiomyxoma (AAM). One year followup of the case does not report with any signs of recurrence.
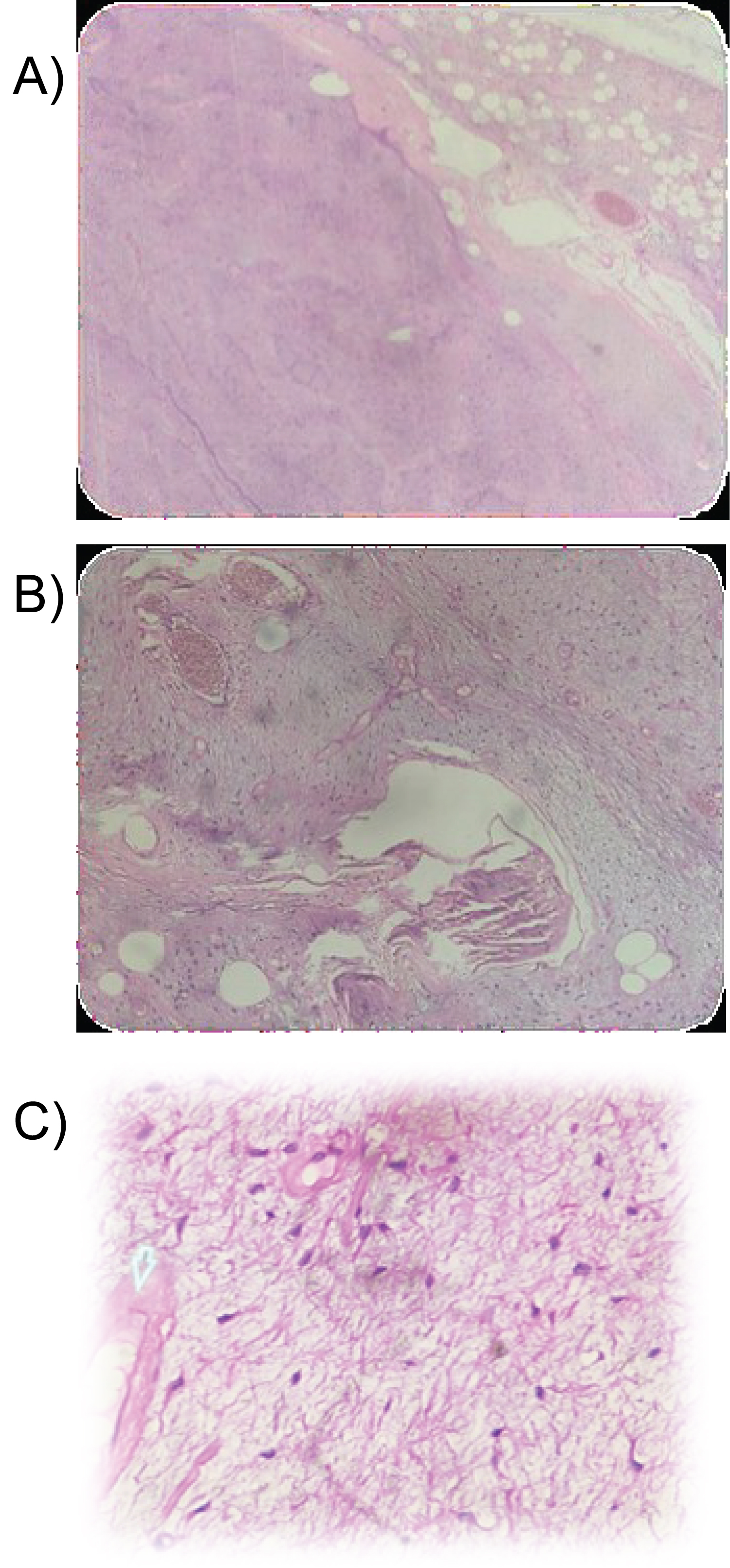 Figure 3: 3a) Hypocelluar lesion with Myxoid background Trapping or invading the adjacent adipose tissue; 3b) Two components Spindled cells scattered in a myxoid background and the blood vessels; 3c) Spindled and stellate cells with bland morphology, thick walled blood vessels and collagen bundles.
View Figure 3
Figure 3: 3a) Hypocelluar lesion with Myxoid background Trapping or invading the adjacent adipose tissue; 3b) Two components Spindled cells scattered in a myxoid background and the blood vessels; 3c) Spindled and stellate cells with bland morphology, thick walled blood vessels and collagen bundles.
View Figure 3
Angiomyxomas are rare, slow growing tumours of mesenchymal origin. They are known to involve the soft tissue of the perineum and the pelvis in both males and females, however extra genital occurance is rare. These lesions are classified as aggressive angiomyxomas, superficial angiomyxomas and angiomyofibroblastomas [1].
Grossly AAM is usually unencapsulated, bulky with a poor circumscription and with a glistening, gelatinous cut surface. The present case was different, as the tumour was well circumscribed, unencapsulated. The histopathological features include hypocellularity, hapahazardly arranged blood vessels of varying calibres, a myxoid stroma with collagen fibres. AAMs tend to infiltrate the adjoining soft tissue [3] as seen in this case. Immunohistochemically, AAMs show positivity for vimentin, desmin and smooth muscle actin. The immunoreactivity of the Oestrogen (ER) and the Progesterone (PR) receptors have been described to be the most characteristic feature [4].
AAM needs to be differentiated microscopically from superficial angiomyxomas, fibroepithelial polyps, angiomyofibroblastomas, myxoid neurilemmomas, myxoid malignant fibrous histiocytomas, myxoid lipomatous tumours, myxoid leiomyomas and cellular angiofibromas. The clinicopathological features, along with the immunoreactivity, help in the diagnosis.
In the present case the presence of medium sized thick walled blood vessels, the deep location of the tumours and the absence of stromal neutrophils in this case, excluded the possibility of a syperficial angiomyxoma, a fibroepithelial polyp and an angiomyofibroblastoma.
Aggressive angiomyxomas are rare slow growing tumours with a high recurrence rate and they occur almost exclusively in the pelvi-perineal region. The present case is unique in being located in the posterior chest wall. A histopathological examination, combined with radiological correlation, helped in distinguishing these lesions from the more commonly occurring similar entities, when they are located in sites other than the pelvis or the perineum.