The study was aimed to screen obsessive-compulsive disorder (OCD); a progressively burdensome, highly prevalent, untreated, poorly detectable psychic condition in general population of Turkey, of around 401 participants, mainly focusing on two parameters (Age groups and Gender). Screening Questions were asked through online questionnaire regarding different attributes of the disorder. In this study we consider a screening measure, a Questionnaire that is not actually designed to diagnose OCD but to help people determine and inform mental health professionals for further discussion about diagnosis and treatment plan. Occurrence of OCD in youth specially females of age ranging from 20-30 years is noticeable due to high inflation and recent pandemic. Questionnaire for screening in fields where affected individuals congregate seem persuasive, although evidence that screening is socially & clinically beneficial in terms of reducing morbidity is still lacking. People seems to be unaware of the sign & symptoms, its progression and hence the severity of disease, as it stays undetected due to lack of proper instruments, so evaluation of screening tools and their use in reducing disease burden are important areas for further research.
Obsessive compulsive disorder, OCD, Turkey, Psychic
Obsessive-Compulsive Disorder (OCD) is a stereotypical, commonness but misdiagnosed and poorly recognized neuropsychiatric disorder characterized by repetitive behaviors, recurrent distressing and undesirable thoughts or mental ceremonials in order to alleviate anxiety [1]. It actually consists of two terms Obsession and Compulsion. Obsession are repeated thoughts, mental images or cravings that cause anxiety e.g. Fear of germs and contamination, while on the other hand Compulsion are reiterating manners an doings that an individual suffering performs in response to an obsession e.g. Excessive washing and cleaning hands, ordering an arranging things in a particular way, numeration of things, in order to inspect if the door has been locked [2]. OCD is more common in young people because it is under recognized and untreated, the reason behind this is children at this age find the symptoms embarrassing and they don't disclose them until they are asked [3]. Half of people develop symptoms before 20 years, symptoms to develop after the age of 35 is unusual [4]. Symptoms are related to tics, jerks e.g. motor ticks which include sudden, brief repetitive movements like shoulder shrug and most often, eye blinking, vocal tics which usually include grunting sounds, sniffing and clearing of throat [2]. Lifetime tic disorder has been seen in 10% to 40% individuals suffering with OCD [5]. A most reliable four-factor structure was found out by a meta-analytic revision of symptom structures, the teams encircled a "taboo thoughts issue", a "symmetry factor", a "cleaning factor" and a "hoarding factor". The Taboo thoughts factor was relating to distressing and intrusive thoughts of religious, sexual or violent in nature. The symmetry issue correlates with obsessions involving symmetry, arrangement, numeration additionally as ordering and repetition compulsions. The cleaning factor was obsessions and compulsions relating to dirt, contamination and cleansing. The hoarding factor was obsession and compulsion related only to hoarding [6]. Neurophysiological findings of OCD show cognitive impairment in attention, visuospatial skills and nonverbal memory [7]. Structural Neuroimaging, and functional studies of brain implicate the basal ganglia, posterior cingulate cortex (PCC), insula, prefrontal cortex (PFC) and while Neurochemical and Genetic studies implicate monoamine neurotransmitters and glutamate, especially dopamine and serotonin [8]. Referring to an underrepresentation, the life time prevalence of OCD is around 2.3% because people are unaware of symptoms and they report it when it becomes severe [9]. In pediatric OCD, around 40% qualify for remission and around 40% still have OCD in adult hood [10]. It is most often accompanied by secrecy and shame leading to increased risk of suicide. OCD when not treated becomes chronic and runs a lifelong course with intensity fluctuating but rarely disappearing [11]. Symptoms are not permanent or persistent, they come and go, they are usually triggered by their obsessions, stress, alcohols or drugs like tranquilizers. It is usually misled with other mental disorders like anxiety and schizophrenia. In 2006, Obsessive-Compulsive related disorders (OCRDs) work group as a inference of meeting, the Research Planning Agenda of Diagnostic and Statistical Manual (Fifth Edition) (DSM-V) shows that OCD must be omitted from Anxiety Disorders which was in consonance with the present International Classification of Mental Disorder (ICD-10) as a distinguish category, although according to ICD-10 both lies under the same roof of "neurotic, stress-related, and somatoform disorders," [12]. Being poorly recognized, only a minority of patients receive the proper timely treatment [10]. Risk factors of OCD include Genetics (higher risk if the first cousin has a child with congenital OCD), Brain functioning and structure (dissimilarities in FC & subcortical parts of brain and congenital serotonin deficiency) and Environment, PANDAS has been suspected to cause OCD in children [2]. Serotonin transporter gene, h-SERT, mutation has been found as cause of OCD in unrelated families [13]. Serotonin receptor 2B gene (HTR2B; MIM 601122) has been found out to be a pharmacologically appreciable candidate gene in early onset of OCD [14]. Comorbidities associated with OCD include problems mentioned in Figure 1 [15]. Causes include alleviated fractional inhomogeneity in (AMI) anterior midline tracts, alleviated volumes of dorsolateral PFC connected to administrative function while increased white matter volume [16,17]. Alleviated amount of Dopamine2 binding in striatum [18]. Olanzapine (Zyprexa) like Atypical antipsychotics have been turned out to cause de-novo type of OCD [19]. OCD has been ranked with in twenty most leading cause of disability by World Health Organization WHO [11]. Clinical studies indicate that appreciable psychosocial morbidity is related to OCD as compared to alternative diseases [11]. All aspects of Quality of Life (QOL) and physiological functions are markedly affected in the person with OCD and are associated with depression severity and OCD severity [20]. Diagnosis includes Y-BOCS as a rating scale to estimate the severity of the disease [9]. First-line therapies that are recommended for OCD are ERP, CBT and SSRI [21]. CBT involves accumulated exposure to the issues whereas forbidding the incidence of repetitive behaviors [22]. Fluvoxamine FLV proved to be a safe and effective treatment as it improved the symptoms of depressed as well as non-depressed patients [23]. Naturally occurring inositol has been suggested to be used as treatment of OCD [24]. OCD symptoms might improve from µ-opioids, such as hydrocodone and tramadol [25]. NICE guidelines in 2006, put forward antipsychotics treatment for OCD that did not ameliorate with SSRI [26]. In severe and refractory cases ECT has been found to have effectiveness [27].
The aim of this study is to screen the obsessive-compulsive disorder (OCD) among the youth of Turkey. We hypothesize that the youth of Turkey is suffering from OCD especially after the high inflation and price hikes in almost each sector such as education, food and health. We hypothesize that the main group of people that are suffered right now because of the above-mentioned reason is youth, especially the students studying at the various universities in Turkey. Although, the young or adult students are unlikely to be affected by inflation but the responsibility of starting their career in Turkey as well as difficulty in making future planning is hitting in a very severe way to these people due to inflation as well as the damaged caused by COVID-19 in recent years. All of these stressful situations have triggered the mental disorders among the people especially the OCD. We have focused and compared our study with the past prevalence studies of OCD among US adults (2001-2003). Due to all these hypotheses, we expect the results of our study will be much alarming especially among the youth. To achieve our purpose, we have evaluated the mental perception of distress and focused on clinical analysis of psychotherapists via the results of questionnaire.
A cross¬-sectional study was conducted for the entire research population. The study site was Middle East Technical University, Ankara, Turkey. The study populace was the general population in Turkey irrespective of their history, ethnicity and socio-cultural belief. An organized, self-administered Questionnaire containing close ended questions was used as the screening tool for the Identification of the disorder. Using the cross-sectional study design data was collected by means of online questionnaire. The Questionnaire used is provided at the end of the Methodology. The method includes screening of general population or around 401 participants. With respect to genders e.g. male and female and with respect to different age groups e.g. 20-30y, 31-40y, 41-50y, greater than 50 years. Data was collected using an online questionnaire designed using google forms and link was shared via distinctive social media platforms. The screening questions were asked from the individuals to help them recognize and inform health professionals for further guidelines regarding the diagnosis as well as the treatment. Moreover, the frequency and the intensity of OCD is also assessed by using this screening measure. Data collected was calculated by using IBM SPSS Statistics 25. Data analysis consists of frequency analysis, reliability analysis and cross-tabulation for Chi-Square (χ2) by age and gender Table 1 and Table 2 respectively and Fisher's Exact test by Age (where cell counted less than 5 in person's chi square) to test for statistical significance. The study took around 4 months duration from April 2022 to July 2022. The questionnaire included a written consent form which stated all the necessary information regarding the purpose of study and ensured that the data provided by the patient will be kept private and not be misused in any illegal activity.
Table 1: Represents the results of cross-tabulation & chi-square test with respect to age. View Table 1
Table 2: Represents the results of cross-tabulation & chi-square test with respect to gender. View Table 2
On the basis of data collected through questionnaire response the descriptive statistics are presented in the Table 3. It was seen from Figure 2 and Figure 3 that Females of age group 20-30 years are more susceptible. The past prevalence studies of OCD among U.S Adults (2001-2003) did confirm the statistics Figure 3 [28]. According to the responses taken through the questionnaire it has been seen that people did seem persuasive but the evidence of screening process, being helpful clinically and socially lacks in reducing the morbidity and burden of disease.
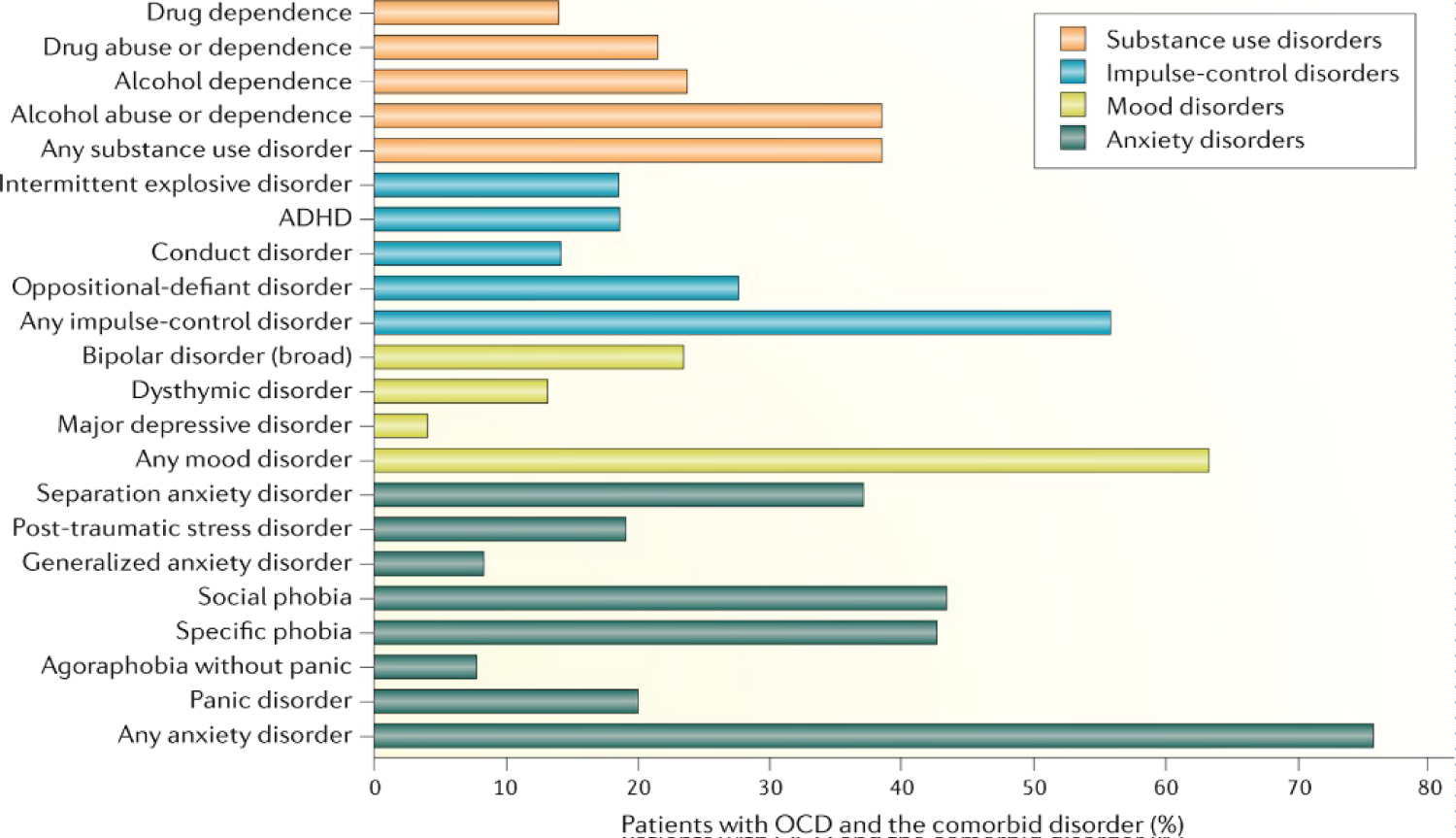 Figure 1: Percentile presentation of Comorbid disorders of OCD [15].
View Figure 1
Figure 1: Percentile presentation of Comorbid disorders of OCD [15].
View Figure 1
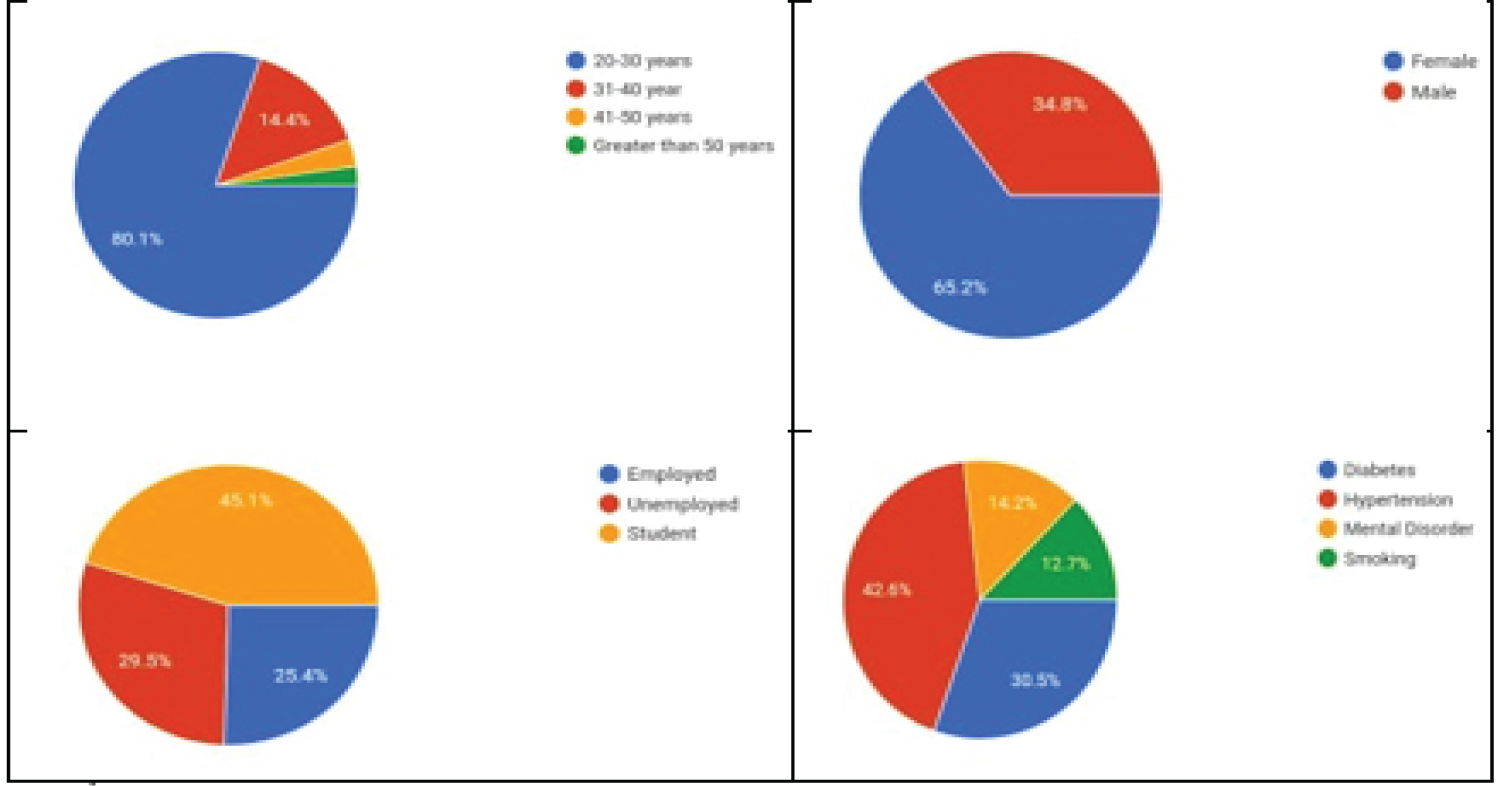 Figure 2: Descriptive statistics of demographic data.
View Figure 2
Figure 2: Descriptive statistics of demographic data.
View Figure 2
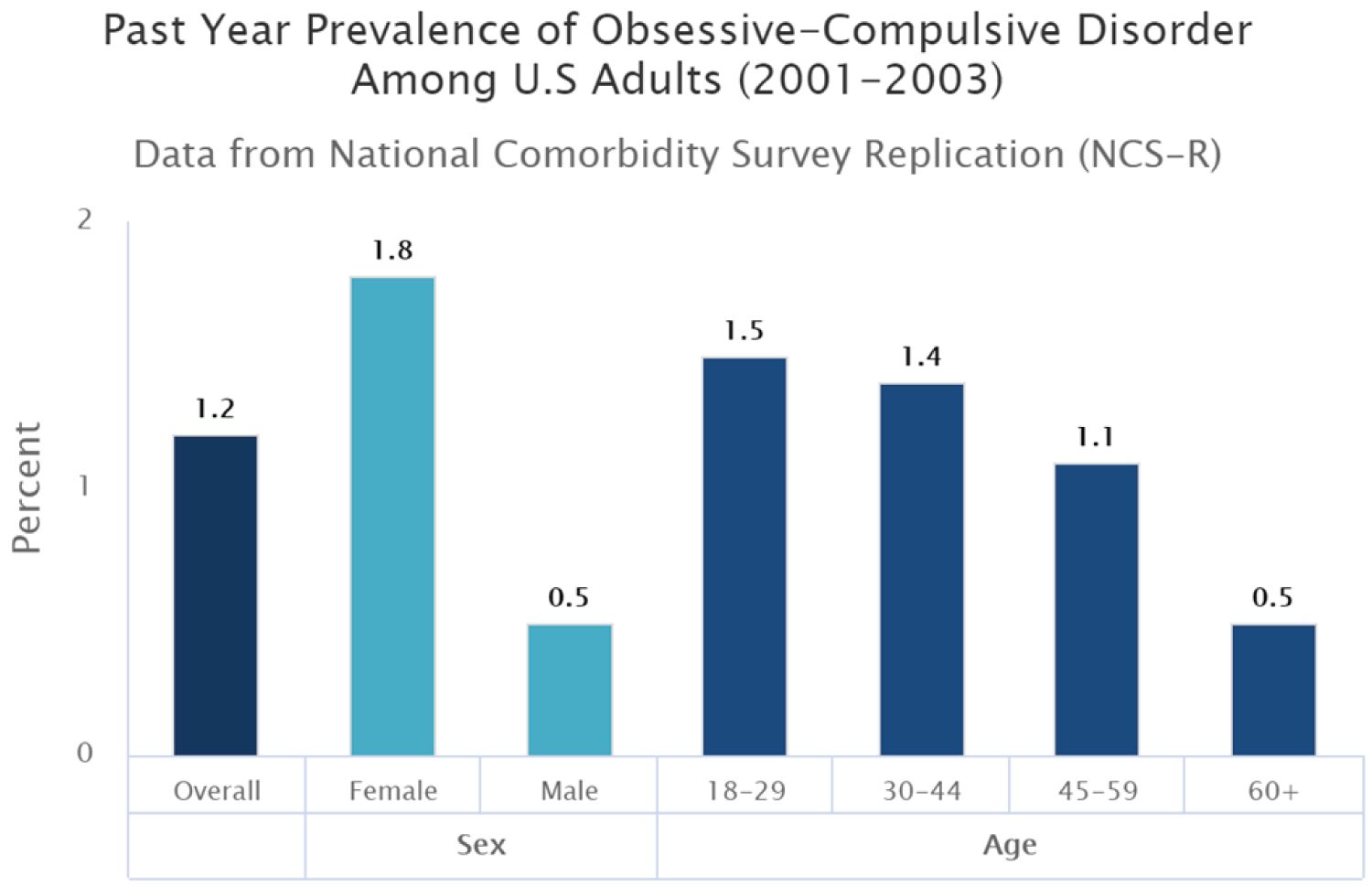 Figure 3: The prevalence of obsessive-compulsive disorder among American adults last year (2001-2003 [29].
View Figure 3
Figure 3: The prevalence of obsessive-compulsive disorder among American adults last year (2001-2003 [29].
View Figure 3
Table 3: Represents the results of fisher's exact test with respect to age. View Table 3
Study statistics and results are alarming and require professional attention as there is such a high count of patients suffering from OCD. The main cause behind this seems to be untreated OCD, which tells that due to some factors people don't get proper treatment. Most of the patients include young teenagers as the stats as well as past studies show a noticeable ratio of occurrence of OCD in adults. Reasons include unawareness of the sign & symptoms, progression and severity of the disease. Reasons behind unawareness are lack of acknowledgement and social stigma. Another main reason for untreated OCD is lack of screening tools, measures and instruments which makes OCD a misdiagnosed and poorly recognized disorder so evaluation of screening tools and their use in reducing disease burden are important areas for further research. Another reason of having such an alarming result of OCD among youth is the recent inflation that has hit the Turkish economy in a worst way. The lack of financial or social support among most of the students studying at Turkish universities has suffered the people with various mental disorders and OCD is one of the prominent disorders among them. As observed in the above tables, the major group of people suffering from this ailment is 20-30 years of age. Focusing on the gender, it is clear that OCD is more common among the females as compared to males. The possible reason is the more disturbances in the social life of woman as compared to men. In past years, various research studies have been carried out to prove that males are less likely to suffer from OCD as compared to women. Our demographic studies have reported female predominance in prevalence which has been reported in past studies across the world [28-30]. Subjects with OCD in our study had history of hypertension 42.6% followed by diabetes 30.5%, mental disorder 14.2% and tobacco smoking 12.7%. Around 51.2% people agree that their routine activities take a long time to complete, this could possibly lead to academic failure and occupational impairment as well. 56% people agree that they need reassurance about their doings which could possibly lead to lack of self-confidence and self-esteem.
Overall study findings add to the growing evidence that OCD is common and is usually ignored which leads to progression of the illness and Is associated with suicidal attempts. The statistics and results suggest that those people who are not fulfilling the criteria of OCD do need primary care, professional support to reduce the risk of morbidity.
The screening of OCD was based only on the self-administered questionnaire and self-reported responses of the participants. No interview regarding diagnosis was conducted to confirm the diagnosis. Unawareness of sign & symptoms, lack of knowledge, lack of screening tools and measures are the reason due to which this common illness remains unrecognized. There for estimate of prevalence might not be precise due to lack of proper screening tools, measures and instruments.
The statistics and the result of the study demonstrates that Obsessive-Compulsive disorder is taking an alarming turn as a mental disorder in youth of Turkey and the demerit is, lack of screening or diagnostic tools make its determination and identification difficult which leads to progression of the disease. Untreated OCD is more common in young females and have noticeable morbidity including suicidal thoughts. This finding is of high significance but in Turkey, it is not given that much importance like other mental illnesses such as anxiety & depression. So in nutshell, primary care health professionals and mental health professionals need to start looking OCD as a life threatening illness and should arrange awareness seminars and more importantly introduce proper screening tools and treatments to alleviate the spread of this life threatening disease.
This study has been carried out as an observational study using various questions. The request to publish the data has been sent to the ethical committee. All the participants of this study were informed before and had taken under the written consent to participate in this study.
Authors declare that there is not any conflict of interests in this study.