There is a high prevalence of goiter in Bisha despite more than 15 years of the national campaign for increased dietary iodine supplementation. The cause is multifactorial. It is associated with non-neoplastic and neoplastic conditions. Surgical management has evolved over many years.
To describe the pathological types of goiter in Bisha along with their management and to discuss current surgical considerations.
A retrospective review of 339 patients with goiter diagnosed by FNAC and or histopathological examination and managed surgically or non-surgically.
There were 339 patients, of which 280 (82.6%) were females and 59 (17.4%) males. Age range was seven to 94 years with a mean of 39.18 ± 13.87 years. There were 138 (40.7%) multinodular goiters, 82 (24.2%) colloid goiters, 8 diffuse goiters (2.4%), 40 (11%) solitary thyroid nodules, 10 thyroid nodules (2.9%), 14 thyroid cysts (4.1%), 20 Hashimoto's thyroiditis (5.9%) and two de Quervain's thyroiditis (0.6%). Benign thyroid neoplasms comprised of 25 (7.4%) follicular adenomas and 11 (3.2%) Hürthle cell adenomas. Malignant thyroid disorders consisted of 18 (5.3%) papillary thyroid cancers, 7 (2.1%) mixed papillary/follicular thyroid cancers, one (0.3%) mixed follicular/papillary thyroid cancer, and three (0.9%) follicular thyroid cancers respectively. There were 128 (37.1%) total thyroidectomies, 70 (20.6%) hemithyroidectomies, 10 (2.9%) subtotal thyroidectomies and, 5 (1.5%) near-total thyroidectomies. There were 125 (36.9%) patients who had no surgery. The overall complication rate was 14.5%.
Thyroid disorders are still prevalent despite years of dietary iodine supplementation campaigns. The rate of complications following total thyroidectomy is significant and guidelines are changing.
Thyroid disorders, prevalence, thyroidectomy, Bisha, Saudi Arabia
Goitre is common in the Southwestern region of Saudi Arabia where Bisha is located, in the longest valley of the Arabian Peninsula, standing at an altitude of approximately 610 meters (2,000 ft.) above sea level. In fact, recent studies have shown that Asir region Province (where Bisha is located) has the highest prevalence of goiter in Kingdom of Saudi Arabia (KSA) [1-4]. This is associated with a variety of pathologic conditions including thyroiditis, endocrine dysregulation, autoimmune disease and neoplasia. Many factors may account for this rate. An obvious factor is iodine deficiency which has been found to correlate with a proportionate increased prevalence and severity of the disease. A study of 3046 schoolchildren's urinary iodine content in 2015 found that iodine deficiency was still prevalent and endemic (more than 23% of the number studied) in the Asir region [4]. This was despite a universal iodization of salt started in 1997 in the Kingdom. The recommended dietary iodine salt in KSA is between 70 and 100 ppm as potassium iodate, even though this is higher than the WHO recommended level of 15-40 ppm [5-7]. A recent National study shows that only 61.8% of the Asir population studied use recommended iodized salt in cooking [8].
The salt content of the soil is also correlated to incidence of goiter where high salt content may be goitrogenic despite iodination of table salt. There are several studies carried out in some regions of Saudi Arabia that reported the presence of high calcium in drinking water and concluded that some samples were not suitable for human consumption [9]. Alqahtani, et al. recently published a study of the soil characteristic in Bisha which demonstrated “very hard” water in 92% of the samples studied with major elements (Na, Mg, and Ca) exceeding the guideline limits of WHO in some samples [10]. Hard water contains mainly calcium or magnesium carbonate. Calcium is goitrogenic.
The role of nitrates, as environmental pollutants, in thyroid carcinogenesis is generating increasing interest recently. Nitrates commonly contaminate water and food as they are used as fertilizer in nitrate-rich manure. This may lead to high amounts present in fruits and vegetables, especially those grown in greenhouses. Nitrate competitively inhibits iodide uptake at the sodium-nitrate symporter and, by so doing, prevents the uptake of iodine by the thyroid gland. They are competitive inhibitors to iodine and may generate N-nitroso-compounds which are carcinogenic. It has been implicated in the aetiopathogenesis of differentiated thyroid cancer [11]. In recent decades, differentiated thyroid cancer (DTC) incidence has been increasing worldwide. It is the second most common cancer among women in Saudi Arabia [12,13].
Currently, the diagnosis of a thyroid mass is by FNAC which in the hands of an experienced thyro-cytologist, accurately categorizes the histological types in over 90% of samples [14-17]. FNAC helps to determine the nature of a thyroid mass and to diagnose malignancy preoperatively. However, it can be a subjective area of diagnosis and subject to different interpretations.
The commonest reason for thyroidectomy is cosmesis but fear of malignancy is the basis for some patients to seek surgical intervention. Ideally, the extent of thyroid resection should determine by the reason for the surgery. Recurrence, problems with reoperation and need for completion thyroidectomy if incidental thyroid cancer is found, have changed the behavior of surgeons towards favoring total thyroidectomy as procedure of choice when the entire gland is involved with disease or when there is malignancy. However, this practice needs to be evaluated by meta-analysis and clinical reviews.
King Abdullah Hospital Bisha has become strategic referral center in the southwestern region and receives many patients from the surrounding towns. A complication of thyroidectomy is one of the common cases resulting in litigation. We hereby conduct an epidemiological study to investigate the pathological types of thyroid disorders and their management, the incidence of complications and discuss current management considerations and strategies.
Institutional approval was obtained from the ethical committee of King Abdullah Hospital. This is a retrospective study conducted in Surgery department of King Abdullah Hospital Bisha between December 2013 and December 2019. The clinical records of the patients were retrospectively reviewed, and a proforma was used to obtain information from the records that included demographic information, clinical features, methods used in diagnosis (Fine Needle Aspiration Cytology, thyroid ultrasound scan, CT scan of the neck, thyroid function test), type of treatment received (surgical or non-surgical), and result of postoperative histopathological examination of the resected thyroid gland.
Data was collected from both sexes of all age groups. All patients with clinically confirmed goiter were included. Excluded from the study were subjects with inadequate specimen for diagnosis, and incomplete data or data acquisition errors. A final 339 patients were analyzed by the study (Figure 1).
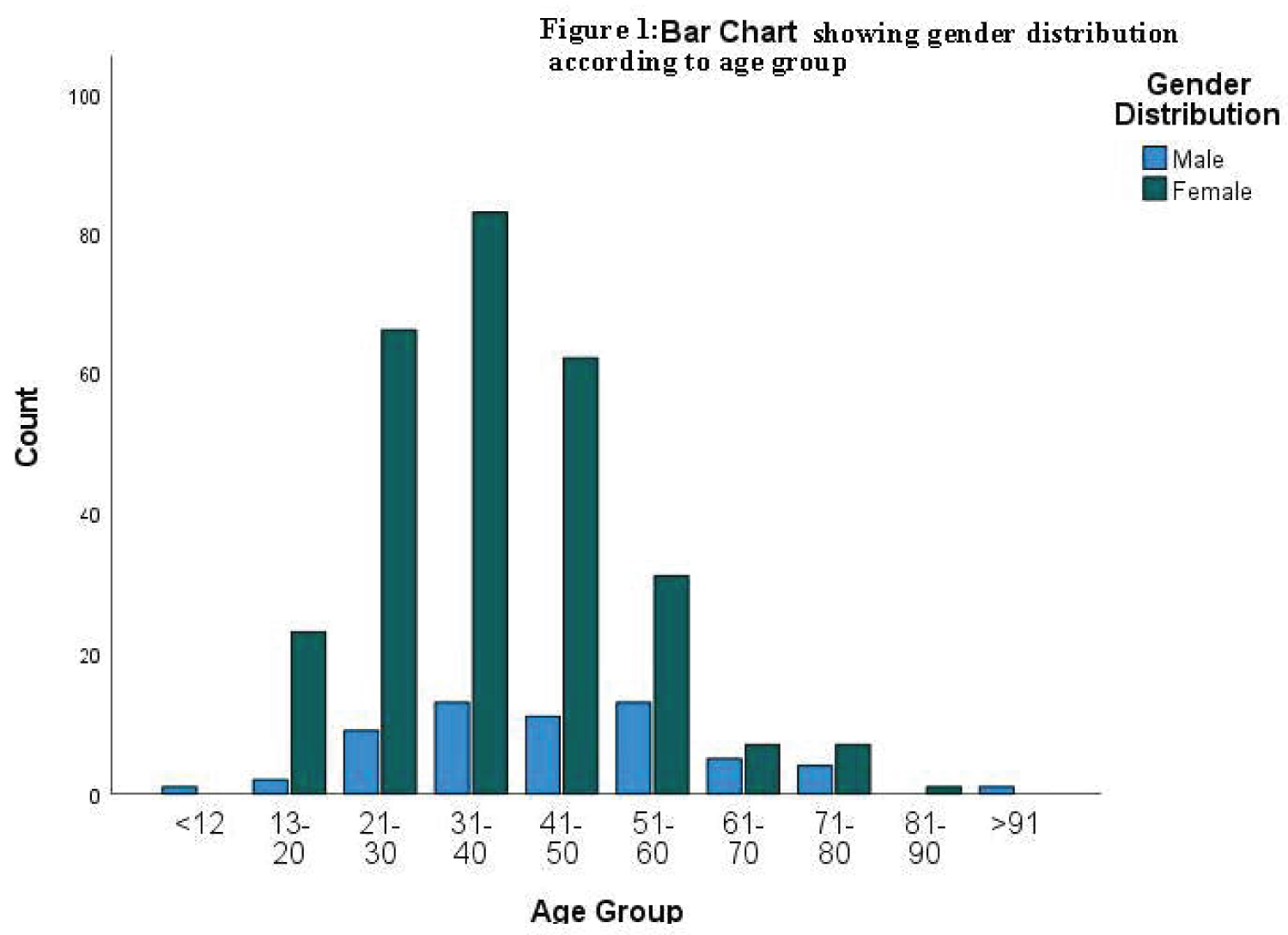 Figure 1: Gender & Age distribution chart.
View Figure 1
Figure 1: Gender & Age distribution chart.
View Figure 1
A proforma was used to obtain the demographic data, and medical history of each patient. Demographic data included gender, age, and nationality.
Total leukocyte count, thyroid function test, blood chemistry analyzed by a HITACHI automated biochemical analyzer (7600 HITACHI Ltd., Japan).
Total T4 (bound and free T4): 4.5-11.5 ug/dL; Free T4 (FT4): 0.8-1.7 ng/dL; T3 (Triiodothyronine) Free (serum): 0-6 years: 2.4-4.2 pg/mL; 7-17 years: 2.9-5.1 pg/mL; > 18-years-old: 2.3-4.2 pg/mL; TSH: 0.3-5.0 U/mL
The records of all thyroid ultrasound examination were reviewed as performed by certificated sonologists using a SonoScape X5 ultrasound device with 5-15 MHz L741 linear probe, and a GE LOGIQ device with 7-10 MHz linear probe. For this study, goiter is defined as a total volume greater than 18 mL in women and 25 mL in men [18].
The Statistical Package for Social Sciences (SPSS) version 26 was used to measure qualitative and quantitative variables. The quantitative variables like age and the qualitative variables like histopathological diagnosis were analyzed.
Data from 354 patients' files were obtained. Of these, five patients had incomplete data, and 10 patients had FNAC results either with inadequate specimen collection or indeterminate diagnosis. Data from 339 patients were valid. Table 1 illustrates the age group and sex distribution of the patients studied. Of these, there were 280 (82.6%) females and 59 (17.4%) males resulting in a female/male ratio of 4.75:1. Age ranges from 7 to 94 years with a mean of 39.18 ± 13.87. There was only one (0.3%) case of thyroid disorder below 12 years of age. The incidence of thyroid disorders rises from 7.4% (2 cases) in the age group 13-20, through 22.1% (75 cases) in the age group 21-30 to peak at 28.1% (96 cases) in the age group 31-40. The incidence then drops from 21.5% (73 cases) in the age group 41-50, through 13.0% (44 cases) in the age group 51-60, 3.5% (12 cases) in the age group 61-70, and 3.2% (11 cases) in the age group 71-80, to tail at 0.3% each in the age groups 81-90 and above 90, respectively. Most of the males were in the age groups 31-40 (3.5%) and 51-60 (3.5%) while most females were in the age group 31-40 (28.3%). Distribution of patients according to their nationalities is shown in Table 2. There were a total of 315 (92.9%) Saudi nationals, out of which 49 (14.5%) were males and 266 (78.5%) were females, respectively. This was followed by Sudanese who numbered 6 (1.8%) in total, with 2 females and 4 males, respectively. The remaining nationalities, consisting of Indians, Pakistanis, Sri Lankans, Bangladeshis, Filipinos, Egyptians, and Indonesians, made up less than 1% each of the total population, respectively. The distribution of thyroid pathologies is illustrated in Table 3. There were 138 (40.7%) cases of multinodular goiters, 82 (24.2%) cases of colloid goiter, 8 cases of diffuse goiters (2.4%), there were 40 (11%) solitary thyroid nodules, 10 cases of thyroid nodules (2.9), and 14 cases of thyroid cysts (4.1%). Cases of inflammatory thyroid lesions consisted of 20 cases of Hashimoto's thyroiditis (5.9%) and two cases of de Quervain's thyroiditis (0.6%). There were a total of 65 neoplasms (19.17%), of which there were 36 (10.6%) benign and 29 (8.55%) malignant lesions. Benign thyroid neoplasms presented as follicular adenomas in 25 (7.4%) cases and Hürthle cell adenomas in 11 (3.2%) cases. Of the malignant thyroid disorders, papillary thyroid cancer occurred in 18 (5.3%) cases, mixed papillary/follicular thyroid cancers in 7 (2.1%) cases, mixed follicular/papillary thyroid cancers occurred in one (0.3%) case, and follicular thyroid cancers occurred in three (0.9%) cases, respectively. A total of 287 (84.7%) patients were euthyroid, 15 (4.4%) had toxic goiter and 37 (10.9%) had hypothyroidism. Multinodular goiter patients presented with most of the symptoms of toxicity, 10 (2.9%), and hypothyroidism, 12 (3.5%). Other clinical features were obstruction in 10 (2.9%) patients, and pain in seven (2.1%) patients as illustrated in Table 4. The operation rate in the cohort was 63.1% (214 patients) as can be seen in Table 5. Of these, 128 (37.1%) had total thyroidectomy, 70 (20.6%) had hemithyroidectomy, 10 (2.9%) had subtotal thyroidectomy and finally, and 5 (1.5%) had near-total thyroidectomy. The remaining 125 (36.9%) of the patients had no surgery. The overall complication rate was 14.5%. Complications after subtotal and hemi-thyroidectomies for benign thyroid diseases included seven recurrences (11.43%), three incidental thyroid cancers (0.9%), four unilateral recurrent laryngeal nerve palsies (1.9%), and complications following total thyroidectomies were 16 hypocalcemia (7.5%) cases and one case of loss of voice or aphonia (0.5%) as shown in Table 6.
Table 1: Gender distribution according to age group. View Table 1
Table 2: Distribution by nationality and gender. View Table 2
Table 3: Pathologic type of goiter and thyroid status distribution. View Table 3
Table 4: Distribution of Clinical features of goiters seen in Bisha. View Table 4
Table 5: Type of operative management. View Table 5
Table 6: Complications following thyroidectomy. View Table 6
Thyroid diseases can be described as either neoplastic or non-neoplastic, benign, or malignant lesions. They may present clinically as diffuse, multinodular, or solitary thyroid nodule, functionally as euthyroid, hypothyroid or hyperthyroid disorders. Their evaluation is important because most can be managed surgically or medically. Al Ghamdi, et al. studied 100 cases following thyroidectomy in Bisha, and classified the disease based on post-operative histology [19]. Their study highlighted the specific types of thyroid disorders that were frequent indications for thyroidectomy in the Bisha region. In this review, we studied the data of all patients that presented with thyroid disorder. Our aim was to analyze the histological pattern of thyroid diseases managed in Bisha region and to discuss the current guidelines of surgical management in the literature.
The highest incidence of thyroid disorders occurred in females aged between 31 and 40 (28.3%). This correlates with findings in other studies within and outside Saudi Arabia [20-23]. Male to female ratio varies widely from country to country and region to region. The Male: Female ratio in our study was 1:4.75, similar to 1:4.5 reported by Ghafoor, et al. from Pakistan [24] and 1:4.74 from Bangladesh, Rahman, et al. [25] Ratios have been reported from 1:2.5 in Pakistan, Fahim, et al. [26] or 1:2.7 in Madinah, Albasri, et al. [23] to 1:7.9 in Zambia, Mirzakarimov, et al. [27].
The most frequent thyroid disorder was multinodular goiter (40.7%). This was followed by colloid goiter (24.1%). In the study by Al Ghamdi, et al. multinodular goiter (MNG) made up 31% of the bulk of indications for thyroidectomy in Bisha [19]. Our finding correlates with reports of higher incidence of MNG from other studies, namely 43% from Asir, Abu-Eshy, et al. [28], 80% from Riyadh, Raddaoui, et al. [20], 76.1% from Jeddah, Qureshi, et al. [22], 31.4% to 45.0% in a Malaysian study, Othman [29], 36.8% in Western KSA, Salama, et al. [30], 62.8% from Yemen, Al-Hureibi, et al. [31], from Turkey 42%, Aydin, et al. [32] and, from Poland 57%, Marcinkowska, et al. [33]. Nodules in a thyroid gland may represent growth and fusion of colloid filled follicles, which may be felt by palpation when they are up to 1 cm in diameter or located on the surface of the gland. They may also be discreet adenomatous growths or cysts. The prevalence of nodular goiter is directly proportional to the degree of iodine deficiency in a community [34]. As conceptualized by David Marine, the thyroid, in response to decreased iodine deficiency or increased TSH stimulation goes into a period of hyperplasia but eventually because of iodide repletion, enters into a resting phase characterized by storage of colloid giving rise to a colloid goiter; this cycle repeats itself many times giving rise to a non-toxic multinodular goiter [35]. Figure 2 illustrates the relationship of TSH and thyroid weight (g) in patients with clinically euthyroid multinodular goiter.
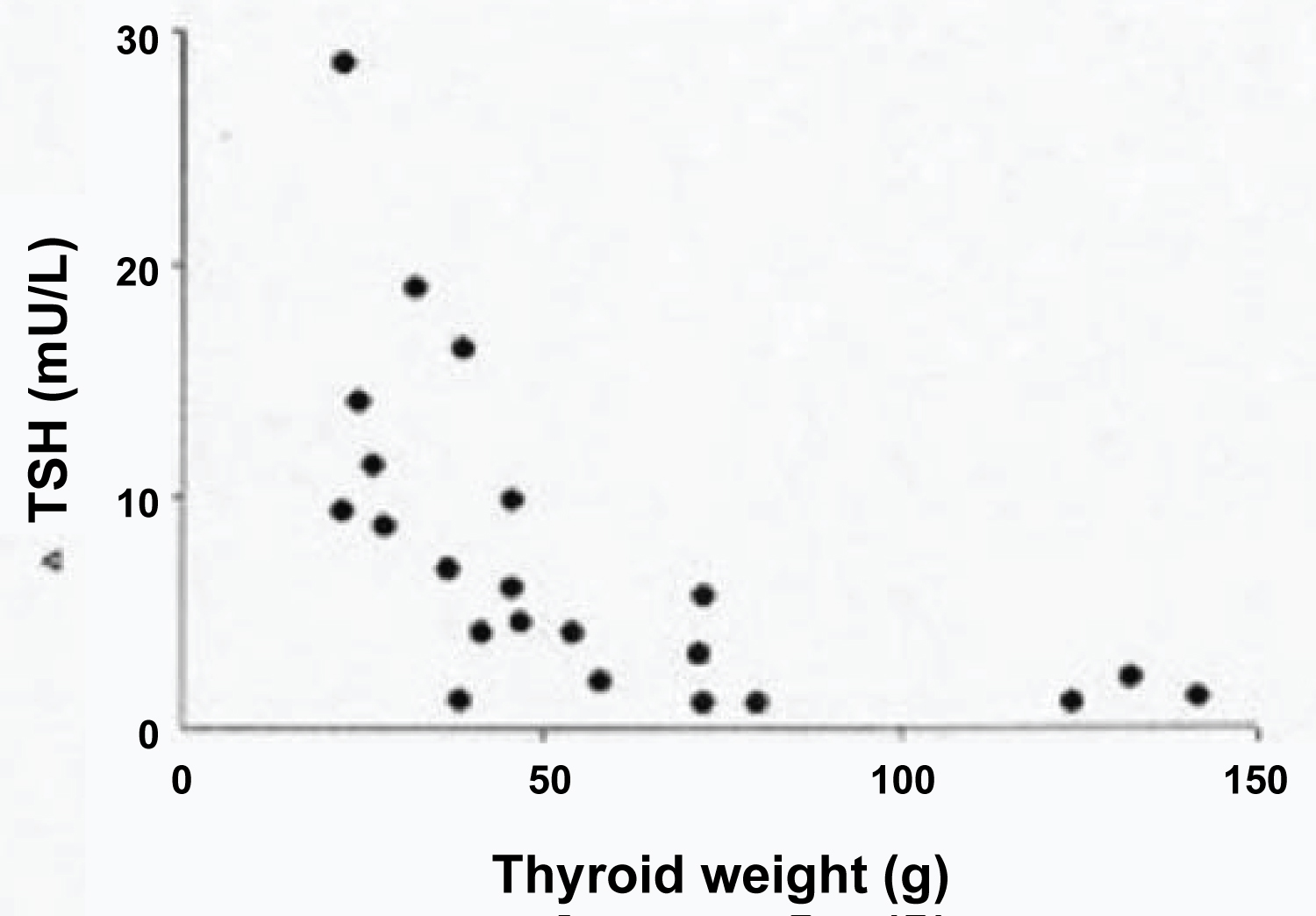 Figure 2: The relationship of TSH and thyroid weight (g) in patients with clinically euthyroid multinodular goiter.
View Figure 2
Figure 2: The relationship of TSH and thyroid weight (g) in patients with clinically euthyroid multinodular goiter.
View Figure 2
Other studies reported a reverse pattern of incidence between colloid goiter and multinodular goiter. Albasry, et al. reported that colloid goiter was more prevalent (58.2%) than multinodular goiter in their series in Al-Madina region [23]. Ngadda, et al. reported a similar high prevalence (75%) of colloid goiter in Nigeria [36]. The reason for the variation in prevalence between MNG and colloid goiter may be multifactorial. Shao, et al. reported a significant increase of non-toxic MNG prevalence in Shandong, a littoral region where there is high dietary/salt iodine content [37]. Similarly, Multiple studies have reported higher incidences of toxic adenoma in iodine-deficient areas and non-toxic multinodular goiter in iodine-excess or iodine sufficient areas [38-41].
The overall incidence of toxic goiter in our study was 7.09% (24/339). There were 16 cases of toxic MNG (4.72%) and eight cases of diffuse toxic goiter (2.36%). We did not record any case of toxic adenoma in this study. A similar rate (7.7%) was recorded by Abu-Eshy, et al. in Asir region [28]. Iodine supplementation was shown to reduce the prevalence of thyrotoxicosis in six European countries, Reinwein, et al. [42]. Areas of iodine deficiency without dietary supplementation, on the other hand, have been shown to have high incidences of hyperthyroidism. Mengistu, et al. reported a 43.7% incidence of thyrotoxicosis in their study of 373 patients with thyroid disorders [43]. The thyroid gland tends to acquire autonomy in an environment of sustained iodine deficiency. Other factors may increase the predisposition of such promotion, including duration of exposure, age, and functional demand like number of childbirths, smoking and increased body mass index. On the other hand, hypothyroidism constituted 14.45% of our patients.
The incidence of malignancy was 8.55% which is lower than what was reported by many studies in Saudi Arabia, namely Kona & Al-Mohareb (25%) [44], Mofti, et al. (29%) [45], Al-Tameem (21%) [46], Nasr (14.5%) [47] and Abu-Eshy (13.0%) [28]. Papillary thyroid cancer predominated the malignant lesions in this study which is similar to findings in most other studies [12]. However, we did not record any cases of medullary, anaplastic and Hürthle cell cancers or lymphoma in our series. Al Ghamdi [19] (Bisha, 2002) and Al Amri [48] (Eastern Province, KSA, 2012) similarly did not report any cases of medullary thyroid carcinoma (MTC) in their series. This could be due to underdiagnosis, relative low prevalence of malignancy in Bisha or genetic differences compared to other populations. It is most likely due to its rarity in Saudi Arabia. Alzahrani and co-workers studied 629 cases of thyroid cancer in Saudi Arabia and found only 14 (2.2%) cases of MTC [49].
The overall complication rate in our study was 14.5%. The recurrence rate following subtotal thyroidectomy and hemithyroidectomy/lobectomy was 11.43%. A recurrence rate of 43% has been reported after a 30 year follow up [50]. There were three cases of completion thyroidectomy in our study (Table 6), after the surgical specimens were reported to contain cancer, thus, giving an incidental cancer rate of 0.9%. In a retrospective study involving 2592 patients, comparing total thyroidectomy and subtotal thyroidectomy, Tezelman, et al. found a significant increase incidence of completion thyroidectomy in the latter with no difference in permanent complications between the two procedures [51]. The incidental thyroid carcinoma rate was 7.2% in the two groups. Maturo, et al. in Italy, studied 1793 post-thyroidectomy specimens and found a 4.6% incidental thyroid cancer rate [52]. Pezzola, et al. also found an incidental thyroid cancer rate of 18.2% out of 165 patients operated for benign disease [53]. Wang, et al. report that 147 (20.7%) of 709 thyroid cancer specimens were incidentally diagnosed intraoperatively or on postoperative pathological examination [54]. Pagni, et al. found that 45.2% of 287 papillary thyroid cancer cases were incidentally diagnosed following thyroidectomy [54]. For Woolner, et al. it was 59% [55]. In a randomized clinical trial spanning 10 years, and involving 526 patients, recurrent goiter was found in 0.6% total thyroidectomy compared to 8.6% in Dunhill operation and 22.4% in bilateral subtotal thyroidectomy (p < 0.001), and completion thyroidectomy was necessary in 0.6% total thyroidectomy compared to 2.8% in Dunhill operation and 8.0% in bilateral subtotal thyroidectomy patients (p < 0.001) [56,57]. Any permanent morbidity present at 10 years showed no significant difference in that study.
There was a long-drawn debate concerning the extent of thyroid tissue removed during thyroidectomy, regardless of whether the surgery was done for benign or malignant condition. Lobectomy and subtotal thyroidectomy were traditionally favored over total thyroidectomy because it was believed that the incidence of recurrent laryngeal paralysis and inadvertent parathyroid injury were less in the former procedures. However, the possibility of recurrence and the need for a completion thyroidectomy if the final histology is cancer, are important considerations. For these reasons, the 2016 guidelines and meta-analysis recommended total thyroidectomy for both toxic and non-toxic benign multinodular goiter [58,59]. Total thyroidectomy can now be performed as safely as lobectomy and subtotal thyroidectomy are performed, because of improved surgical techniques and experience [50,60]. The aim is to perform a safe total thyroidectomy, abolish risk of recurrence and future need for completion thyroidectomy if the final diagnosis was thyroid cancer.
While many surgeons reported similar complication rates for both total thyroidectomy and lobectomy/subtotal thyroidectomy [61-64], others reported finding increased complication rates with total thyroidectomy [65-67]. This has recently raised questions over the preferred practice of total thyroidectomy [65]. Moreover, there is evidence that the true incidence of hypothyroidism following total thyroidectomy is underestimated [68]. Lorente-Poch and colleagues have outlined in detail, the reasons behind underestimation of the incidence of hypothyroidism in many studies [69]. Some of the reasons they adduced included a variety of laboratory ranges for normocalcemia and reference values, timing of blood sampling in the postoperative period and short/incomplete follow up. In a recent systematic review and meta-analysis, the reported incidence of hypothyroidism following total thyroidectomy is 19-38% and 0-3% respectively [70]. As a result, the updated American Thyroid Association guidelines on thyroid nodules and differentiated thyroid cancer has suggested lobectomy or subtotal thyroidectomy as alternatives to total thyroidectomy [71,72]. In their review, Dralle, et al. as far back as 2011, made a plea for individualizing extent of thyroid tissue resected, instead of making total thyroidectomy a routine procedure, even for experienced surgeons for bilateral thyroid diseases [73].
In conclusion, the prevalence of thyroid diseases remains high in Bisha despite years of dietary iodination likely due to other factors. Complications of thyroidectomy remain significant. There is little evidence for recommending total thyroidectomy over subtotal thyroidectomy on overall consideration. Total thyroidectomy has reduced recurrence rate but may result in more frequent adverse events. There is need for more extensive randomized controlled trials focusing on surgeons' experience, volume of surgery and details of surgical techniques used.
None.
No potential conflict of interest relevant to this article was reported.
Conceptualization: Dauda Bawa, Saleem Khan, Yasser M Khalifa; Formal Analysis: Dauda Bawa; Investigation: Dauda Bawa, Saleem Khan; Methodology: Dauda Bawa, Saleem Khan, Yasser M Khalifa, Shahi S Prabha, Amal Alghamdi; Project Administration: Amal Alghamdi, Hanan Albishi, Nasser Al Tufail; Writing-Original Draft: Dauda Bawa, Yasser M Khalifa and Shashi S Prabha; Writing-Review & Editing Saleem Khan, Amal Alghamdi, Hanan Albishi, Nasser Al Tufail.