A 36-year-old woman with a history of benign refractory esophageal stricture from gastroesophageal reflux disease was treated with anesophageal stent and a gastrostomy tube 2 months prior to presenting with acute dysphagia and odynophagia. Esophagram and upper endoscopy revealed esophageal stent migration into the stomach and a pinpoint stricture of the distal third of the esophagus, which made retrograde extraction unfeasible. The stent was successfully extracted through the pre-existing gastrostomy site after dilating the site with a controlled radial expansion balloon. This is the first reported case of stent extraction through a gastrostomy site.
Esophageal stent, Esophageal stricture, Stent migration
Esophageal stent placement was historically used for palliative treatment of dysphagia caused by malignancy. Recently, its use has extended to treat benign refractory esophageal strictures (BRES) by providing continuous non-permanent dilation. Stent removal is routinely performed after a few weeks of treatment, or immediately performed when the stent has migrated [1,2]. However, traditional extraction methods are limited in patients who have severe esophageal strictures or obstructions. Therefore, unconventional methods need to be considered in these patients.
A 36-year-old female presented to the emergency room with the complaint of severe dysphagia to solids and liquids over the past 2 weeks. She had a pertinent history of an esophageal stent placed 2 months ago for longstanding BRES from gastroesophageal reflux disease at an outside hospital, and a previously placed gastrostomy tube (G-tube) for supplemental feedings secondary to her BRES. She noted the sensation of food lodging in her chest, voluminous regurgitation, nausea, vomiting, and chest pain that was worse with food intake.
Esophagography exhibited an esophageal stent in the stomach, a severe long segment distal esophagus stricture, and proximal thoracic esophageal dilation (Figure 1). Esophagogastroduodenoscopy (EGD) revealed a 5 cm long esophageal pinpoint stricture that could not be traversed with a neonatal scope (Figure 2). In order to pass the neonatal scope, the stricture was dilated up to 8 mm using a 35 inch biliary guide wire and Savary dilators under fluoroscopic guidance. A 23 mm × 12 cm fully covered self-expendable metal stent (FCSEMS) (WallFlexTM Esophageal stent Boston Scientific) and two through-the scope (TTS) endoclips were visualized in the stomach (Figure 2). Anterograde extraction was not attempted due to the severe degree of stricturing, which was deemed highly susceptible to perforation.
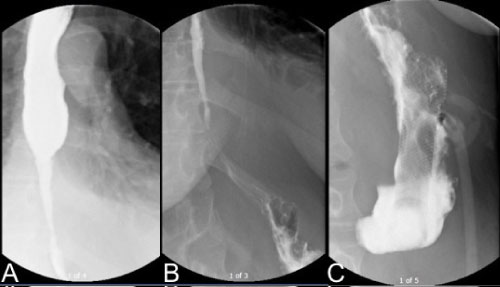 Figure 1: Esophagography showed (A) Proximal thoracic esophageal dilation, (B) A severe long segment distal third esophagus stricture and (C) A large bore metallic stent visible in the left upper quadrant overlying the stomach. View Figure 1
Figure 1: Esophagography showed (A) Proximal thoracic esophageal dilation, (B) A severe long segment distal third esophagus stricture and (C) A large bore metallic stent visible in the left upper quadrant overlying the stomach. View Figure 1
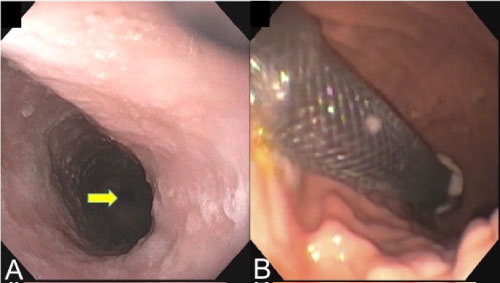 Figure 2: (A) The pinpoint stricture required dilations to pass the neonatal scope, and prevented retrograde extraction of (B) The stent through the esophageal tract. View Figure 2
Figure 2: (A) The pinpoint stricture required dilations to pass the neonatal scope, and prevented retrograde extraction of (B) The stent through the esophageal tract. View Figure 2
A first attempt was made to remove the stent through the gastronomy site with a GIF-XP190N Olympus neonatal scope. The G-tube was removed and a fully covered biliary stent was placed in the site. Rat tooth forceps were inserted, but could not be positioned to reach the microfilament of the stent despite multiple attempts. Due to the complicated hospital course related to hyperglycemia, a decision was made to attempt another EGD stent extraction before proceeding to any surgical intervention.
During the second attempt to remove the stent, the gastrostomy site was dilated up to 12 mm using a controlled radial expansion wire guided balloon dilatation catheter (CRETM Balloon Dilator Boston Scientific) under fluoroscopic guidance. An adult scope was inserted through the dilated site and the monofilament was grasped by rat tooth forceps leading to collapse of the proximal end of the stent (Figure 3). The stent was successfully extracted and the G-tube was replaced.
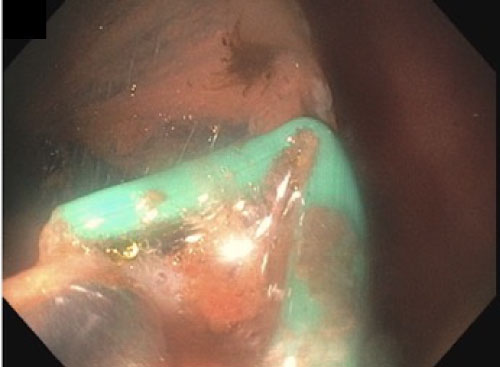 Figure 3: The green monofilament is being grasped to collapse the stent so it can be extracted from the stomach via the gastrostomy site. View Figure 3
Figure 3: The green monofilament is being grasped to collapse the stent so it can be extracted from the stomach via the gastrostomy site. View Figure 3
Mild leakage around the gastrostomy site ceased 48 hours post-dilation as the tract closed around the 20 Fr G-tube. The plan was to perform sequential esophageal dilations instead of placing a new stent due to the high risk of recurrent migration. However, the patient never returned for a follow up.
FCSEMS, self-expandable plastic stents, and biodegradable stents were introduced subsequent to partially covered self-expandable metal stents (PCSEMS) in order to be applicable in treating benign esophageal diseases including BRES, anastomotic leaks, perforations, and fistulae [3]. These stents reduce undesirable consequences of PCSEMS such as bleeding, fistulae, new strictures, and embedment leading to challenging stent removal [4]. Consequently, these stents have higher risk of migration due to limited tissue reaction (9%-31% PCSEMS vs. 26-36% FCSEMS) [5,6]. Despite the high migration rate, esophageal stents continue to be used due to their clinical success (24.4-40.5%) [2,7].
An esophageal stent migrates in one out of every four patients with benign esophageal disease, and known risk factors are FCSEMS, benign conditions, previous stent migration and distal location [5,8]. Therefore, FCSEMS are used in conjunction with stent fixation such as endoscopic suturing by anchoring to full thickness of the esophagus, over-the-scope clips (OTSCs), or TTS endoclips by securing to mucosa only. Recent studies have validated the effectiveness of endoscopic suturing and OTSCs in reducing migration rate [6,8,9]. However, TTS endoclips are reported to be inefficient due to limited opening widths, closure strength and depth of penetration [5,9]. Limited tissue reaction of FCSEMS, lack of mucosal penetration of TTS endoclip, distal location, bulky food bolus diet and intact peristalsis of the esophagus contributed to the stent migration in this patient [5,9,10].
Migration of an esophageal stent should not be considered an emergency. However, it is highly encouraged to remove migrated stents because they can cause small bowel obstruction and perforation [11]. Endoscopic removal of self-expendable stents is feasible and relatively safe with high success rate (97.2%) and low major adverse event rates (2.1%) [1].
The methods for extraction of migrated stents in the stomach described in the literature aim to minimize esophageal injury by reducing the size of the stent. The techniques often utilize combinations of endoloops, polypectomy snares, rat-tooth forceps, double-channel endoscopes, metallic sheaths from bile duct stone lithotripsy, biliary stent pushers, foreign body hood protectors, and overtubes [12-19]. All are performed anterograde through the upper gastrointestinal tract, and thus are not applicable in patients with severe esophageal strictures and/or tumors.
Similar to this case, there are two cases from a retrospective study where a mini-gastrostomy was performed surgically to allow distal access due to a tight esophageal stricture proximal to the stent [1]. However, the details of stents, indication, and intraoperative maneuvers are unknown. Also, retrograde dilation using gastronomy site has been performed to treat complete esophageal strictures in conjunction with anterograde dilation. The complications of retrograde EGD reported in patients are a dehiscence of the site into the peritoneal cavity and displaced G-tube with resultant free air [20].
The case demonstrates a novel method in removing a migrated esophageal stent that may be considered in patients who are poor surgical candidates, whose esophagus is severely obstructed, or predisposed to severe bleeding or perforation. The rationales for this method include, but are not limited to, severe esophageal strictures, tumors, esophagitis, previous history of perforation, and esophageal varices.