Obesity is now recognized to be a problem of public health importance with consequences for health and well-being. The aim of this study was to determine the prevalence and association of obesity and hypertension among primary school teachers in Port Harcourt metropolis in Rivers State, Nigeria. In this descriptive, cross-sectional study, using a cluster sampling method, 400 primary school teachers were selected from public and private primary schools. Their socio-demographic data was collected using a self-administered questionnaire and anthropometric measurements were also obtained. The data was summarized using descriptive statistics and analysed using the Statistical Package for Social Sciences (SPSS) version 23. The findings showed an extremely high prevalence of obesity as well as a high prevalence of hypertension among the teachers. The prevalence of general obesity using BMI was 80.8% and that of central (abdominal) obesity was 84.1%, 61.1% and 97.0% using waist circumference, waist-hip-ratio and waist-height-ratio respectively. The prevalence of hypertension was 27.4%. Using the chi-squared test of association, a statistically significant association was found only between waist-hip-ratio and hypertension. Both obesity and hypertension were prevalent among teachers in this study. Obesity especially central obesity was also associated with negative health outcomes like hypertension. Urgent health education of teachers on the risk factors of hypertension and obesity so that they can avoid them and take responsibility for improving their health indices in this regard was recommended. Another recommendation is the incorporation of weight reduction activities for teachers as part of the regular physical education programs.
Obesity, General obesity, Central obesity, Hypertension, Primary school teachers
Obesity is now recognized to be a problem of public health importance with consequences for health and well-being. Overtime, there has been a dramatic change in the definition of what is considered a beautiful body [1]. The perceptions of the ideal shape have changed over the past few decades and leanness is now often equated with self-control, fitness and beauty in today's society [2]. This paradigm shift in beauty standards has coincided with and is being enforced by the evidence-based complications associated with overweight/obesity which has raised global concern over obesity. Obesity has become a global pandemic with disastrous consequences for human health [3]. Obesity is defined as a chronic disease in which there is excess or abnormal fat accumulation in adipose tissue such that the health of the individual is impaired [4,5]. It is an important risk factor in the development of other chronic, non-communicable diseases. It affects both children and adults and is gradually replacing infectious diseases and under-nutrition as an important contributor to ill health in this century [4].
Obesity is a risk factor for several chronic diseases like diabetes, musculoskeletal disorders (e.g. osteoarthritis), certain cancers and cardiovascular diseases like coronary heart diseases, cerebrovascular accidents and hypertension [6]. Other health problems include breathing problems like sleep apnoea, skin problems as well as social and psychological problems amongst others [7]. Obesity has been shown to be associated with cardiovascular diseases like hypertension and other metabolic diseases though the mechanisms for these associations are still not properly or completely elucidated [8,9]. Obesity has been said to both predispose to hypertension as well as alter the pathway of the development of cardiac complications that are sequel to hypertension [10].
Teachers as a professional group have been shown to experience many risk factors that may predispose them to developing both obesity and hypertension [11]. Teaching is a mentally stressful occupation. Many teachers have a low level of physical activity and may indulge in unhealthy diets (especially those living in urban areas). These factors in addition to use of tobacco products and harmful use of alcohol predispose teachers to developing obesity, hypertension and other NCDs. There is however a paucity of information on the anthropometric indices of teachers or their non-communicable disease risk profile in Africa as a region and Nigeria in particular. In other countries professional cohorts like nurses and teachers have been studied with useful results [12]. The information provided by studying NCDs among teachers in Nigeria will be useful in evidence- based decisions to provide prevention or control strategies for this important group of workers.
The study sought to determine the prevalence of obesity and hypertension and the association between selected obesity indices and hypertension among teachers in public and private primary schools in Port Harcourt, Rivers State.
The study was a descriptive cross-sectional study among 400 primary school teachers aged between 18 and 70 years working in public and private primary schools in Port-Harcourt, Rivers State. The sample size was calculated using the Taro Yamane's formula for estimating sample size. A cluster sampling technique was used in the selection of (public and private) primary school teachers from a total of 34 school clusters (17 public and 17 private primary schools) and all eligible teachers who consented to the study were selected. A structured questionnaire was used to collect the data of participants. The questionnaire had two sections. Section one elicited socio-demographic details of the respondents and section two elicited the weight, height, waist circumference, hip circumference and blood pressure of the study participants. The questionnaire was pre-tested before the commencement of the study in a semi-urban local government area in Rivers State. The questionnaire was given to 3 consultants in the epidemiology/biostatistics unit of the Community Health department of the University of Port Harcourt Teaching Hospital to evaluate its appropriateness and completeness for the study.
Weight was measured with study participants in a standing position and measurement was taken to the nearest 0.01 kg with an Omron HN289 digital scale. Height was measured to the nearest 0.01 m using a locally made calibrated stadiometer. Waist circumference was measured using a non-extensible tape at the level of the narrowest point between the lowest coastal border and the iliac crest at the end of a normal exhalation. Hip circumference was measured with a non-extensible tape at the widest circumference of the participant's buttocks to the nearest 0.1 cm. The weight and height measurements were then used in the calculation of the body mass index (BMI) of the participants. BMI was therefore calculated in kg/m2 where kg is a person's weight in kilograms and m2 is their height in meters squared. Values were then converted to reference categories do determine Normal, overweight, and obese persons. WHO recommended cut off ranges for normal, overweight, and obese BMI categories as well as waist/hip ratios were used [13].
Blood pressure was measured with an Omron digital sphygmomanometer. Blood pressure measurements were taken while study participants were seated in a quiet room. An appropriate size cuff was used around the upper two-thirds of the arm while the digital sphygmomanometer was kept at the same level with the heart. The average of three blood pressure measurements taken five minutes apart was used as the blood pressure for each participant. The blood pressure was classified using the WHO/ISH criteria in which participants having a diastolic blood pressure of ≥ 90 mmHg and/or a systolic blood pressure of ≥ 140 mmHg were considered as hypertensive [14].
Ethical approval and permission for the study was sought from the Department of Public Health Ethical committee of the Imo State University. The details/scope of the research was made known to all the participants and their informed, written consent were obtained before their inclusion in the study. Their anonymity was maintained by using assigned serial numbers instead of their names. All primary school teachers who met the inclusion criteria and consented to participate in the study were recruited into the study and questionnaires were administered to them. Upon completion of the questionnaires, they were retrieved and anthropometric measurements were taken. The collected data was checked for completion and accuracy and was then entered into a Microsoft Excel template. The data was cross-checked for entry errors and then transferred to the Statistical Package for Social Sciences (SPSS) version 23 for analysis. The findings were summarized with descriptive statistics. Frequencies were generated and presented in tables and charts. Proportions were compared using the Chi-squared test which was used to test the association between them. The level of statistical significance was set at p < 0.05.
There were 325 (81.2%) females and 75 (18.8%) males in this study, most of who were within the age bracket of 31-40 years (46.1%) or less than 30 years (23.1%). Mean age of the respondents was 37.88 ± 8.94 years. The single and married respondents constituted 105 (27.3%) and 262 (68.1%) respectively. the respondents were more Christians than Muslims, constituting 375 (98.7%) and 4 (1.0%) respectively. The respondents that had obtained tertiary and post tertiary levels of education comprised 355 (89.6%) and 28 (7.1%) respectively. These are shown in Table 1.
Table 1: Socio-demographic features of respondents. View Table 1
Majority of the respondents had spent 1-5 years and 6-10 years in their teaching job, constituting 124 (31.6%) and 108 (27.5%) respectively. Most of the teachers taught mainly Primary 1 and Primary 5/6 classes; the classes with ≤ 20 pupils and between 21-40 pupils constituted 172 (43.9%) and 167 (42.6%). These can be seen in Table 2.
Table 2: Job History of study participants. View Table 2
As seen in Table 3, the body mass index of the respondents shows the prevalence of obesity and overweight to be 80.8% and 16.4% respectively. In Table 4, it is seen that abdominal obesity as categorized using waist circumference, waist-hip ratio and waist-Height ratio shows prevalence of 84.1%, 61.1%, and 97.0% respectively.
Table 3: Prevalence of Obesity among study participants. View Table 3
Table 4: Prevalence of abdominal obesity. View Table 4
The bar chart (Figure 1) shows the WHO/ISH blood pressure classification of respondents, with optimal, normal blood pressure classifications and mild hypertension (grade 1) having higher percentages. The prevalence of hypertension among respondents, using the WHO/ISH classification as seen in Table 5 was found to be 27.4%.
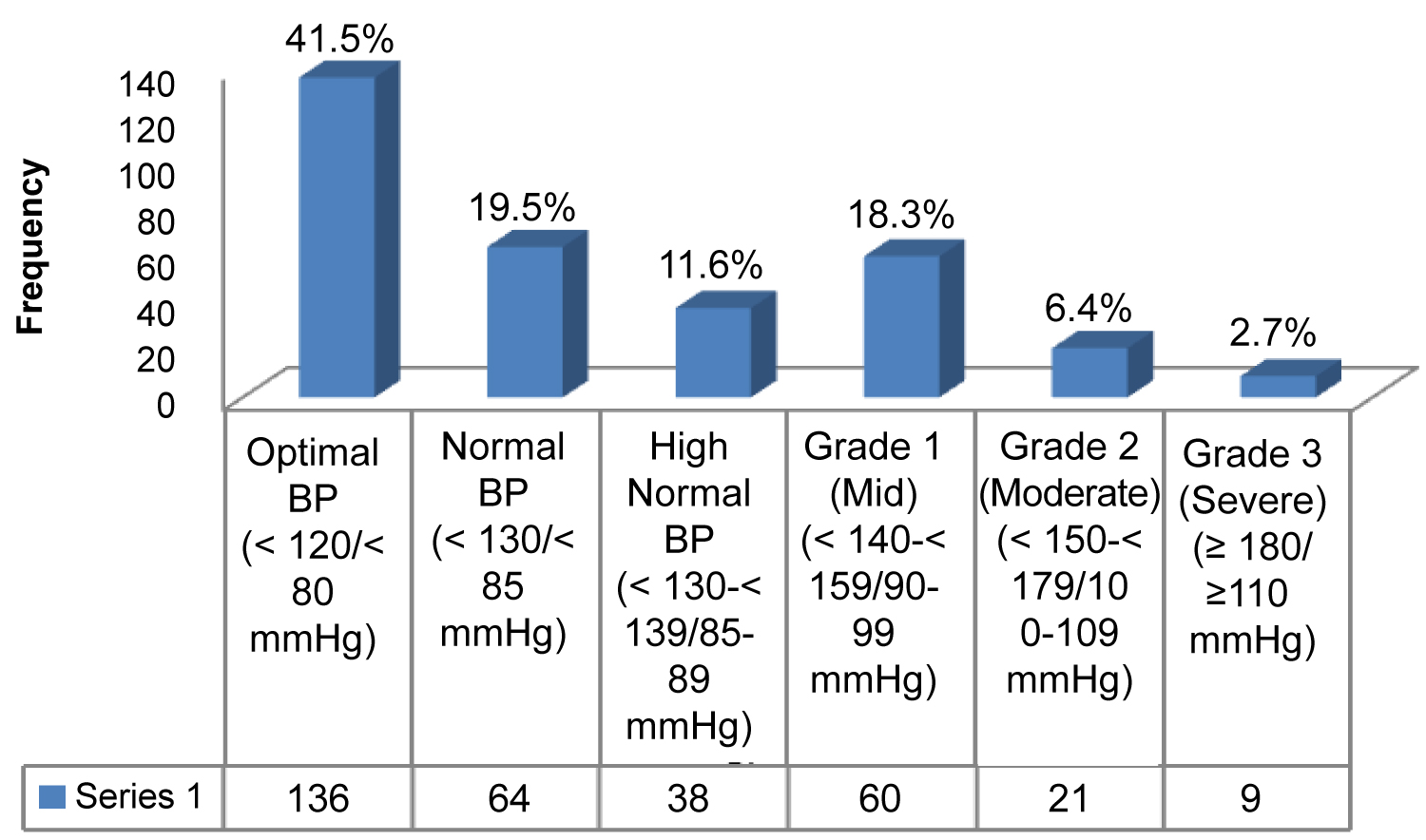 Figure 1: Prevalence of Hypertension using WHO/ISH classification.
View Figure 1
Figure 1: Prevalence of Hypertension using WHO/ISH classification.
View Figure 1
Table 5: Prevalence of Hypertension using WHO/ISH classification. View Table 5
As seen in Table 6, testing of the association between hypertension and the anthropometric indices of the study participants showed that only their waist-hip ratio was significantly associated with the occurrence of hypertension (p-value < 0.01). Other associations were not statistically significant.
Table 6: Relationship between obesity, abdominal obesity and hypertension (WHO/ISH classification). View Table 6
The only predictor of hypertension among the variables in the model in Table 7 after adjusting for confounding variables was waist-hip ratio. The odds of developing hypertension among persons who were obese according to the waist hip ratio was two times higher than those with normal waist hip ratio (Adjusted O.R = 2.03; 95% C.I = 1.1-3.7).
Table 7: Predictors of hypertension among study population. View Table 7
This study showed that irrespective of the anthropometric index of obesity used, the prevalence of obesity among the study participants was extremely high. Using BMI as an index of obesity, the prevalence of obesity was found to be much higher in this study than the WHO global and country prevalence estimates for obesity in 2010 and 2014. The WHO report showed that the prevalence of obesity was highest in Gulf countries with Kuwait, Bahrain, Saudi Arabia and United Arab Emirates topping the list but the prevalence of obesity by BMI in this study is very much higher than that recorded in all these countries [15]. The South African study among primary school educators found what was thought to be a very high prevalence of obesity but the findings of this study had a much higher prevalence [16]. The participants in this South African study were however drawn from both rural and urban areas while in the index study, participants were only drawn from the urban area and this could explain the higher prevalence. However, in another South African study done among urban teachers seven years ago, using BMI as an index, more than half of the study population was found to be obese in comparison to this study where more than three-quarters of the study participants were obese [12]. This could reflect increasing trends in prevalence of the obesity epidemic as is being globally reported. It has been shown that no country, in the past 33 years, has been able to effect a downward reversal in the prevalence of overweight and obesity [17]. The prevalence of obesity by BMI found in this study is higher than that found in several studies in Nigeria including studies among health service providers in Lagos, urban adults in Abuja, urban/rural adults in Abia as well rural adults in a Niger Delta community [18-20]. Based on the findings in several studies, the prevalence of obesity in Nigeria is said to have reached epidemic proportions but none of the previous studies in the country has determined any prevalence that is comparable to that found in this study [20]. This could be because the above studies were not done among teachers who have been shown to work in an obesogenic environment where many risk factors of obesity exist including unhealthy diet and reduced physical activity.
The prevalence of central obesity, as assessed by waist circumference alone, in this study was higher than that found in several studies done in US, Bangladesh and South Africa [12,21,22].
This is surprising given that the advent of the global obesity pandemic has been linked to the adoption of western diets and fast foods that are found in abundance in countries like the USA which are now being overtaken in terms of prevalence by developing countries. Globalisation of western lifestyles and diets has induced a corresponding change in dietary habits and patterns in Nigeria and other low and middle income countries especially in the urban areas where the impact of this transition is now being experienced as shown by the findings in this study. Port-Harcourt, the city where the study took place is considered the treasure base of the Nigerian nation because it is where most oil exploration companies (both indigenous ones and multinationals) established either their corporate head offices and/or their operational bases. As a result of this, the city is populated with people from different parts of the world; therefore globalisation of lifestyles, diets and food choices has been rapid. There is a preponderance of fast-food outlets in the city that make it easy for the urban populace to choose energy-dense high-fat-low-fibre foods over the traditional low-fat-high-fibre foods. These may have contributed to the extremely high prevalence of obesity among these teachers.
Furthermore, because oil company workers earn salaries that are above average, they are able to afford a few more commodities and services, therefore teachers are able to also make additional income from them through private tutoring of their children after their regular day jobs. Most of these teachers are therefore probably able to afford the costly urban lifestyle and food which together with reduced activity levels may have led to the extremely high obesity levels found among them. This is similar to what was reported in Gulf countries (in the Middle East) where the prevalence of obesity is said to have increased at a very alarming rate over the past two decades [23].
In this study, the prevalence of hypertension among the participants was found to be high. It was higher than the global prevalence of hypertension but was lower than WHO's regional prevalence for hypertension for the African region [15]. The prevalence in this study was also higher than that found among teachers in California, USA; and in Mexico [24,25]. This is not surprising, as according to the WHO, the African region had the highest prevalence of hypertension among the six WHO regions [26]. The prevalence in this study was however lower than that among teachers in Dhaka, Bangladesh and South Africa whose prevalence exceeded both the values recorded by WHO for low and middle income countries [12,16,21]. However, low and middle income countries like Nigeria and other African countries as well as Indo-Asian countries like Bangladesh have been shown to bear the highest burden of hypertension globally. The findings of this study further support the WHO global summary [27].
Conversely, the prevalence of hypertension in this study is higher than that among urban adults in Maiduguri, urbanized workers in Kano, rural community adults in Edo and among medical school lecturers in Port Harcourt, all in Nigeria [28-31]. The higher result in this study may be a reflection of the increasing trends in disease prevalence of hypertension as the most recent of these studies was done several years ago. The findings of this study were however comparable to those of the rural population in the Health Behaviour Monitor among Adult Nigerian Population [32].
The association of central obesity using waist-hip-ratio was found to be statistically significant in this study and from the logistic regression model; waist-hip-ratio was found to be the only predictor of hypertension among the different variables studied. The odds of developing hypertension among teachers who had central obesity were two times higher than those who did not have central obesity. This study finding is like a study in India, which also found the waist hip ratio to be the one most strongly associated with hypertension. However, in contrast to the present study, the other anthropometric indices were also associated with hypertension [24]. This finding is also comparable to the findings in some other studies conducted in Nigeria [33,34]. A WHO expert committee agrees that body mass index, waist circumference and waist hip ratio are all predictive of chronic disease and that waist circumference or waist hip ratio can be used either alone or together with body mass index for anthropometric assessments [35].
These findings indicate a burgeoning epidemic of obesity and hypertension among urban middle-class citizen who hold jobs that expose to sedentary behaviour and unhealthy eating habits. The pressure to deliver lesson notes, teaching outlines and grade scripts and assignments may also be leading to the adoption of easily available unhealthy diets. There is therefore a critical need for school-based policy changes to promote physical activity and healthy eating among teachers. The limitation of this study is the cross-sectional design which makes causal inferences a challenge. However, the recruitment of a good sample size and the use of regression analysis makes the study findings worthy of consideration for the implementation of needed interventions.
Obesity and hypertension are problems of great magnitude. The findings of this study further support this and show that among primary school teachers in Port Harcourt metropolis, the prevalence of hypertension is high. The prevalence of general obesity as measured by BMI and the prevalence of central obesity as shown by the obesity indices of waist circumference, waist hip ratio and waist-height-ratio were also high. However, among the participants in this study, waist-hip ratio was the only anthropometric index that was found to be associated with hypertension.