Distance learning has the potential to aide those in remote communities who have infrequent contact with traditional health services. This study used videoconferencing to deliver educational and support interventions to rural hypertensive adults who received care at an outpatient clinic in the Central Valley of California to develop understanding of high blood pressure management. Based on recommendations from the American Heart Association, topics of discussion included daily salt intake, dietary modifications, exercise frequency, alcohol limitations, tobacco cessation, and the importance of medication adherence. Hypertension complications were also reviewed. The measure employed to assess blood pressure management behaviors was the Likert-based H-SCALE. Analysis of the data was based on comparisons between pre and post-intervention hypertension management behaviors. Data showed significant hypertension self-management behavior improvement among subjects as a result of the distance learning intervention. The positive outcomes of the study provide a foundation for distance learning health education programs in rural communities.
Remote or Rural healthcare in the United States, Distance learning, Videoconferencing in healthcare, Hypertension health behaviors
In a rural area, such as the Central Valley of California, hypertension is pervasive [1]. Hypertension is a chronic medical condition that negatively affects many parts of the body [2]. Making lifestyle modifications daily is beneficial to reduce blood pressure and the risk of complications related to hypertension [2]. These modifications include eating a healthier diet, reducing alcohol intake, avoiding tobacco products, exercising, and adhering to medication regimens [2]. Due to a shortage of medical resources in the Central Valley, educational information regarding hypertension management is not readily available [1,3].
Patients in rural locations, such as the Central Valley of California, may benefit from technologies that support health education for people who live a significant distance from clinics and hospitals [4]. Such patients experienced less than optimal care due to the inability to access needed healthcare information and services [1]. Distance learning via virtual or phone-based communication is a means to provide medical care and information regardless of proximity to medical facilities and healthcare workers [5,6]. This investigation focused on the effect of videoconference-based hypertension health education on personal healthcare management. Rural clients with hypertension were recruited to participate in videoconference-based meetings with a nurse practitioner to discuss personal healthcare management behaviors as related to hypertension. Effectiveness of the intervention on personal healthcare management of hypertension supports the ongoing implementation of distance learning in medical care for rural communities [7].
Convenience sampling was utilized to incorporate individuals from the population of Fresno, a large agricultural community located in the Central Valley of California. Post IRB approval, hypertensive subjects from a primary care clinic in Fresno were recruited via informational fliers to participate in the study. In order to improve power or prevent Type 2 errors, which involved falsely accepting the null hypothesis, and improved alpha or prevent Type 1 errors, which involve falsely rejecting the null hypothesis, a minimum of thirty participants was required [8]. A power level close to one and an alpha level close to zero ensured avoidance of falsely detecting incorrect information [8]. Using the G*power analysis program, with an effected power of 0.95, indicating significant difference between the two tests, an alpha of 0.05, and a power of 0.95, the calculated sample size was thirty [8].
A pre-intervention questionnaire was sent to each consenting individual as an email attachment prior to the virtual meeting and collected for pre-intervention analysis. The questionnaire, Hypertension Self-Care Activity Level Effects Scale (H-SCALE) developed by Dr. Warren-Findlow, is a 33-question Likert-scale based measurement tool of self-care regarding blood pressure management [9]. According to studies on the psychometrics of the H-SCALE in relation to diet, hypertension, and blood pressure control, reliability and validity measurement showed H-SCALE correlation with changes to all factors [9,10]. An H-SCALE score exemplifying good health maintenance was seen in those with normal blood pressures, healthy habits, and healthy diets [9,10].
The distance learning interventions included a one-on-one guided educational meeting held between the nurse practitioner and each of the subjects for an average of 35 minutes. The meetings were held via Zoom videoconferencing software through smart phone devices in the comfort of personally chosen locations. The information presented to each participant was pre-written and uniformly explained. All information discussed was evidence-based and derived from the American Heart Association [2]. Participants were encouraged to ask questions about the material, which promoted active involvement [11]. Personal medical care was not discussed. Approximately thirty-five days after the session, each subject's personal healthcare management behaviors as related to hypertension were- assessed via the H-SCALE questionnaire as a post-intervention measurement of behavior change.
In order to access participants, permission was granted from a local primary/urgent care clinic and an affiliated site, both located in Fresno County, where patients were recruited for the study. The clinic managed physical exams, immunizations, sick visits, minor surgical procedures, and blood tests [12]. Each site was staffed with a provider, a medical assistant, a laboratory technician, a radiology technician, and a front desk administrator and sees approximately thirty patients daily, six days a week [12].
After IRB approval by Regis College, recruitment of research study participants commenced in January 2020. During checkout from the medical clinics, fliers were given to each adult patient over the age of 18-years-old asking for individuals with specific characteristics to contact this researcher if interested in taking part in the study. No incentive aside from a one-on-one education session with this researcher about hypertension was offered. Interested patients were asked to contact the researcher on a password-protected email. Informed consent was obtained per Regis College IRB guidelines. Based on preliminary demographic information provided and the data's compliance to inclusion criteria, thirty specific subjects were chosen for the study.
Criteria to determine inclusion of clients were the following: aged over 18-years-old, English-speaking proficiency, diagnosis of hypertension by a clinician, access to a computer or smart phone, ability to download the Zoom videoconferencing application, and ability to meet for one hour for the educational session. Exclusion criteria included the following: aged under 18-years-old, non-English speaking, pre-hypertension or normal blood pressure, inability to access a smart phone or use the Zoom application, and inability to meet for one hour. Vulnerable groups such as pregnant women, homeless people, incarcerated individuals, and mentally challenged individuals were also excluded from the study.
This study assessed the usefulness of a distance learning intervention through pre and post-educational intervention questionnaires, both of which were e-mailed to participants. No identifying information was asked. Basic demographic data, such as gender, age, education level, distance of home from medical providers, experience with technology, and compliance to current medical care were also collected. Hypertension management behaviors, including salt, tobacco, and alcohol intake, exercise frequency, medication adherence, and diet healthfulness were self-reported by each subject as guided by the H-SCALE [9].
After the initial questionnaire videoconference-based educational meeting took place over electronic devices via the application Zoom. The program, Doodle, was used to schedule sessions based on client preferences. A link to a Doodle scheduler as well as instructions on Zoom application's use was sent to each participant via e-mail. Educational meetings lasted from thirty minutes to one hour, and covered American Heart Association approved personal healthcare management behaviors of hypertension [2]. An average of thirty-five days after the meeting, the same questionnaire was sent to subjects to re-assess personal healthcare management behaviors of hypertension. The differences between the pre and post-questionnaires reported changes in personal healthcare management of hypertension, thereby determining the effect of the distance-learning program on varying facets of hypertension self care. As no personal information was discussed, including hypertension medication management, there were no changes to the subjects' medical care.
The independent variable, the hypertension care educational program, and the dependent variable, the H-SCALE answers, were the factors of interest [13]. As the study observed for differences between a pre-test and a post-test, a paired t-test analysis was performed [8]. A paired t-test was used to assess for significance of the result difference between the two tests due to the educational intervention [8]. No significant changes between the two tests would support the null hypothesis that the intervention had no effect [8,13,14]. Use of the statistical analysis program, Intellectus Statistics, ensured reliability of the data analysis. Reliability referred to the consistency of results produced [15]. Through the use of Cronbach's method of split half reliability, wherein programmers code programs that produce equivalent results when the data is halved in every possible way and separately analyzed, reliability of the programs from Intellectus Statistics is assured [15].
Out of the thirty-two recruited participants, thirty completed the pre and post-tests, an adequate number of subjects needed for type 1 and type 2 error prevention [8]. Demographics of the thirty participants were 80% male and 77% college educated or higher. The mean age group was between 60 and 70-years-old. On average, subjects have had a diagnosis of hypertension for over 6 months and lived within 20 miles of the primary care provider.
Rated on a scale from one to five, where one represented "excellent" or "easy", two represented "very good" or "moderately easy", three represented "good" or "moderately difficult", four represented "fair" or "very difficult" and five represented "poor" or "unable to access", subjects were also asked questions pertaining to health habits and healthcare access. On average, participants felt "fair" in regard to comfort with technology and personal hypertension knowledge, found access to medical sites moderately easy, easily attended most medical appointments, have good health habits, and were in good health in general. After the intervention, most participants found distance learning to be an excellent supplement to regular in-person medical visits, and noted distance learning with a nurse practitioner to be an easy way to address health issues.
Patient blood pressures were assessed prior to and after the educational meetings. The average subject's pre-intervention blood pressure was 145.7/87, with a range of 138-158 mmHg for systole and 78-95 mmHg for diastole. After the intervention, the subjects' average blood pressure was 144.33/82.93, with a range of 138-160 mmHg for systole and 72-92 mmHg for diastole. According to a paired t-test, the measure of the changes in blood pressure between the two tests was found to be insignificant, with p equaling 0.2933. This means that rejection of the correct hypothesis, which is the null hypothesis that blood pressure will not be affected by the educational intervention, leads to a chance of a type I error at 29.33%.
Participants answered 33 H-SCALE questions pre and post the educational intervention. Table 1 lists the questions asked, with topic-based groupings of questions to assess hypertension self-care management. Questions 1-3 discussed medication adherence, questions 4-14 and 21-30 reviewed dietary habits, questions 15-18 reviewed physical activity, questions 19-20 discussed tobacco exposure, and 31-33 discussed alcohol consumption. According to a paired t-test of the 30 pre- and post-tests, the changes in health habits approximately 35 days after the educational session were found to be significantly improved with a p value of 0.0117. This meant that the chance of type 1 error, or rejecting the null hypothesis of no changes in behavior after the intervention when true, was small at 1.17%.
Table 1: Pre- and Post-test answer averages. View Table 1
Demographically, 74% of the subjects were found to be males between the ages of 60 and 70. Eighty-five percent of the subjects were college-educated, and self-reported as moderately healthy with good health habits and a fair amount of knowledge on hypertension. Each subject had a diagnosis of hypertension for over 6 months. On average, most self-reported as diligent patients who attended a moderate number of appointments and lived within 20 miles of their primary care providers. The subjects reported feeling fair in relation to comfort with technology and showed enthusiasm for the opportunity to learn more about hypertension self-management from a nurse practitioner that could answer health-related questions. Many of the subjects also discussed personal feelings regarding distance learning by reporting the intervention to be a useful supplement to hypertension management, provided that the service was free and easy to schedule.
According to the answers given by participants before and thirty-five days after the intervention, personal healthcare management behaviors improved with a statistically significant p value of 0.0117. The improved behaviors included diet improvement by 0.13%, increased physical activity by 36.90%, increased medication adherence by 11.65%, and reduced alcohol ingestion by 4.75%. Among dietary habits, the greatest differences after the educational intervention was an improvement in fruit and vegetable intake, and an increased likelihood to eat smaller portions and to buy and choose healthy food options. According to the physical activity questions, participants were more likely to increase day-to-day activities to improve physical fitness rather than to formally exercise. Additionally, subjects who confirmed alcohol intake noted a reduction in the number of alcoholic drinks consumed on a daily basis. Medication adherence improved as well, though not considerably. The two individuals who regularly used nicotine products did not lessen tobacco use and exposure after the intervention (Figure 1, Figure 2, Figure 3, Figure 4 and Figure 5).
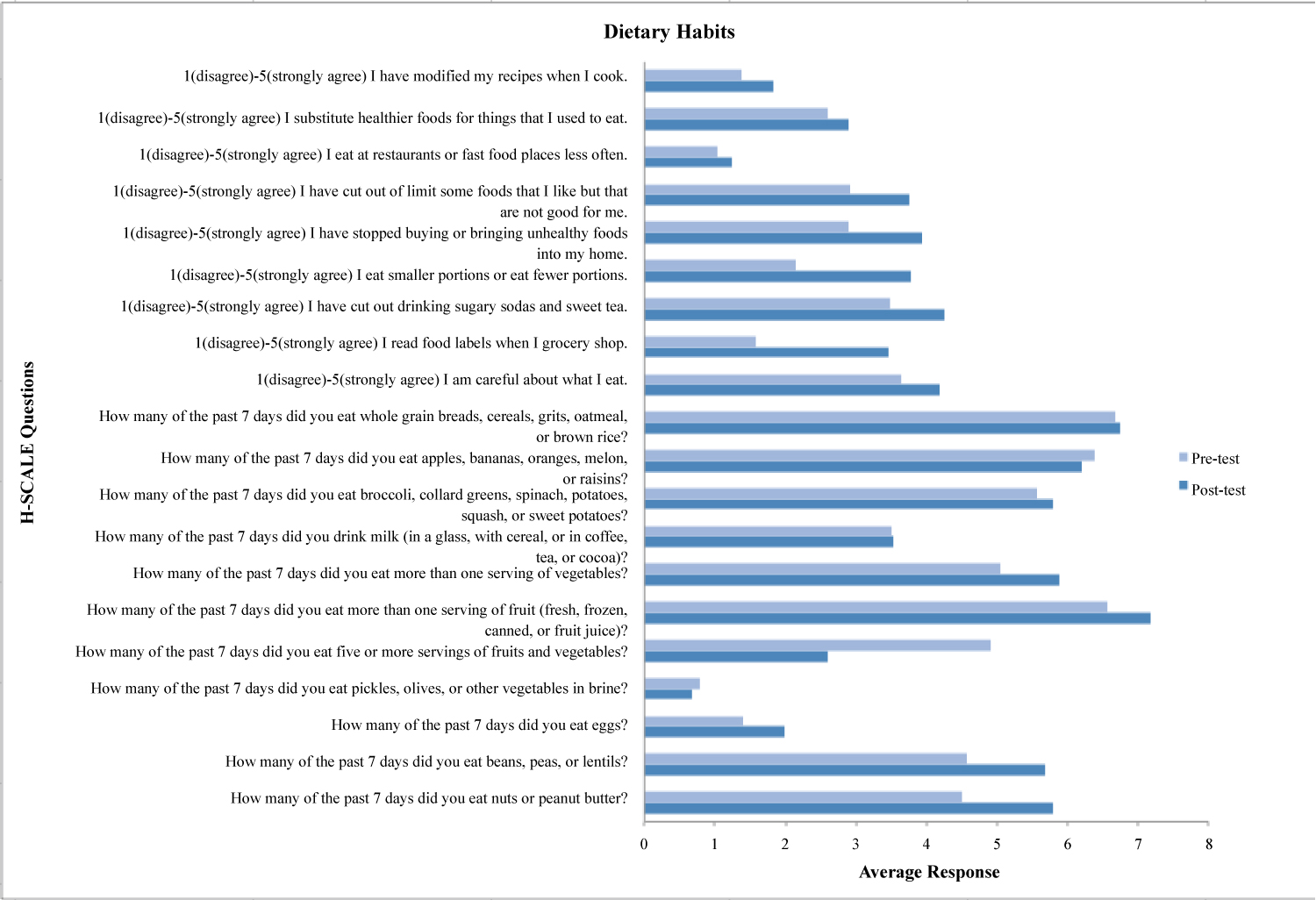 Figure 1: Dietary habits.
View Figure 1
Figure 1: Dietary habits.
View Figure 1
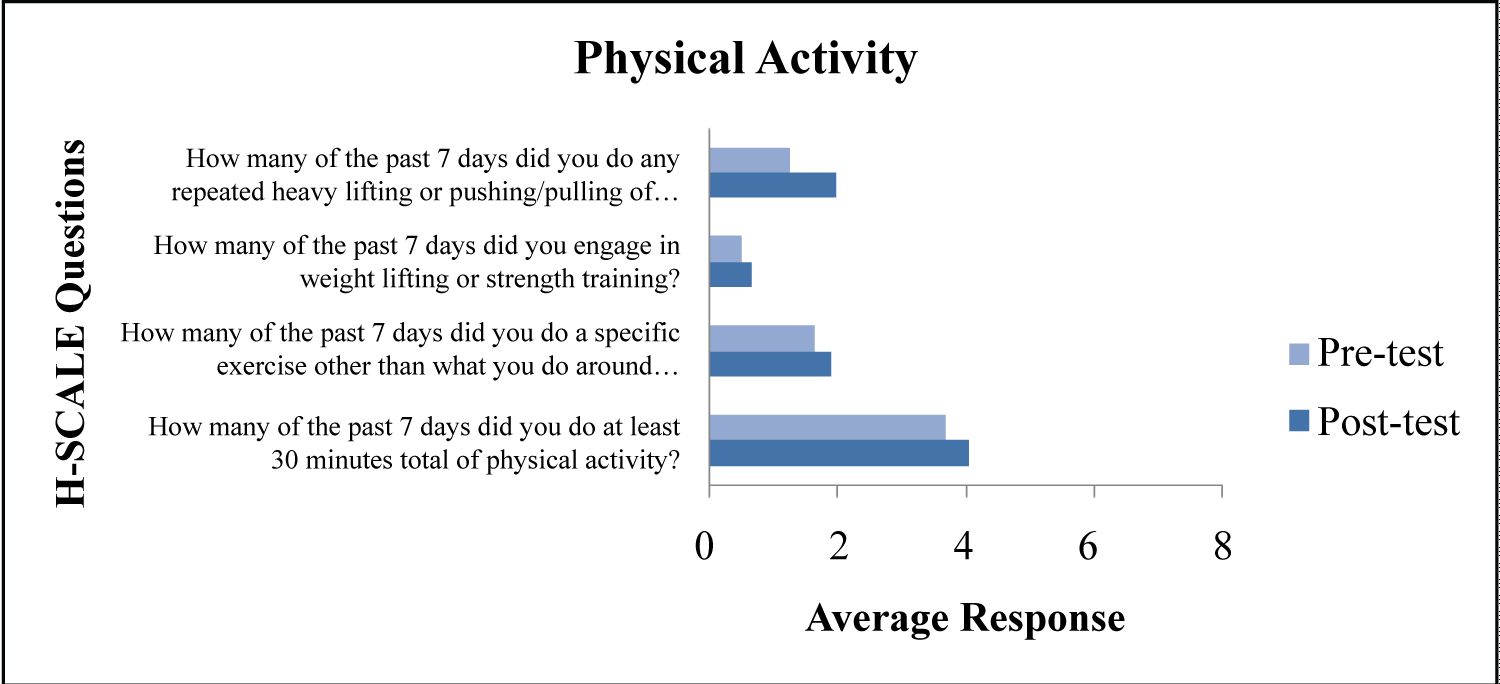 Figure 2: Physical activity.
View Figure 2
Figure 2: Physical activity.
View Figure 2
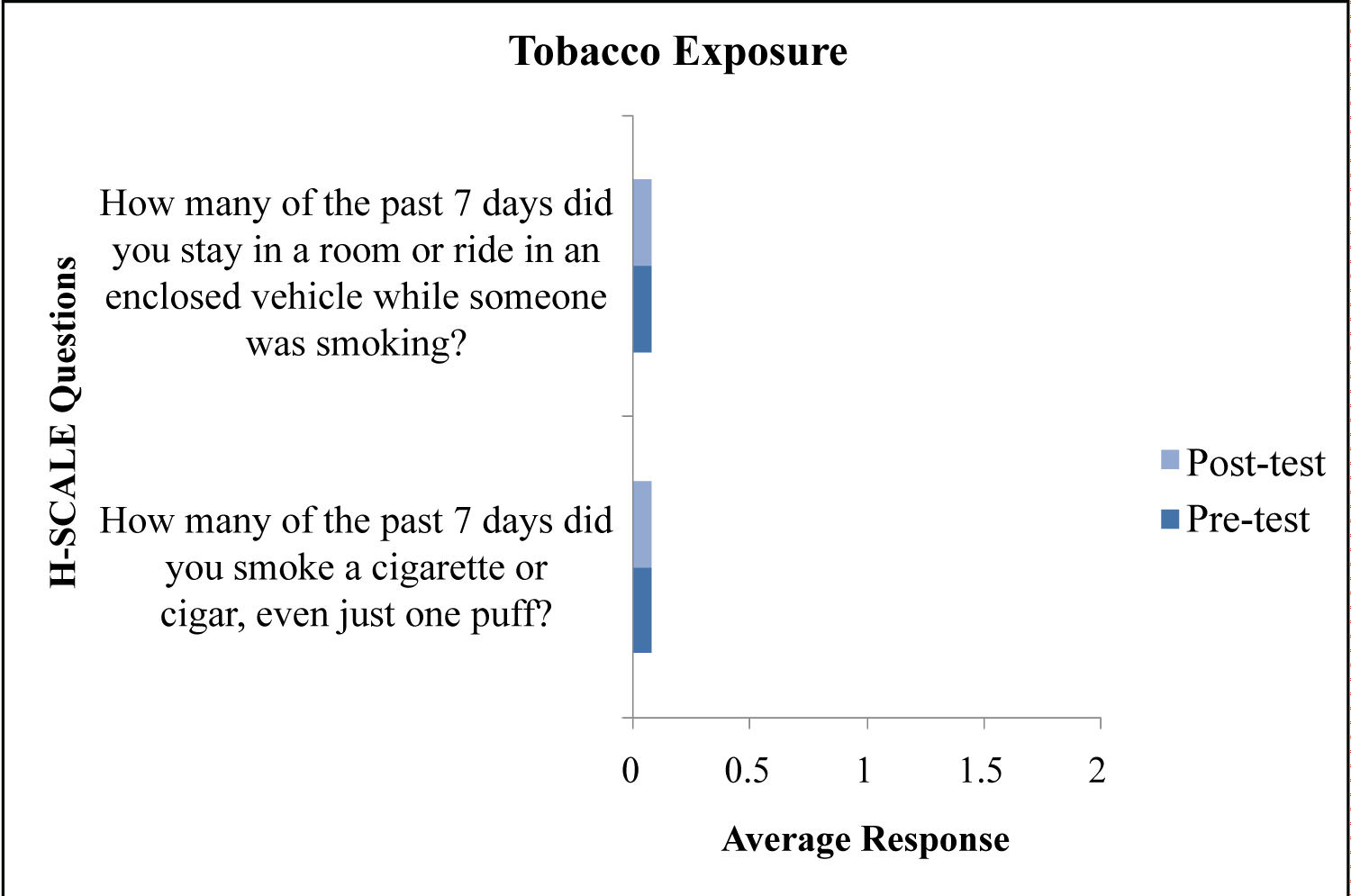 Figure 3: Tobacco exposure.
View Figure 3
Figure 3: Tobacco exposure.
View Figure 3
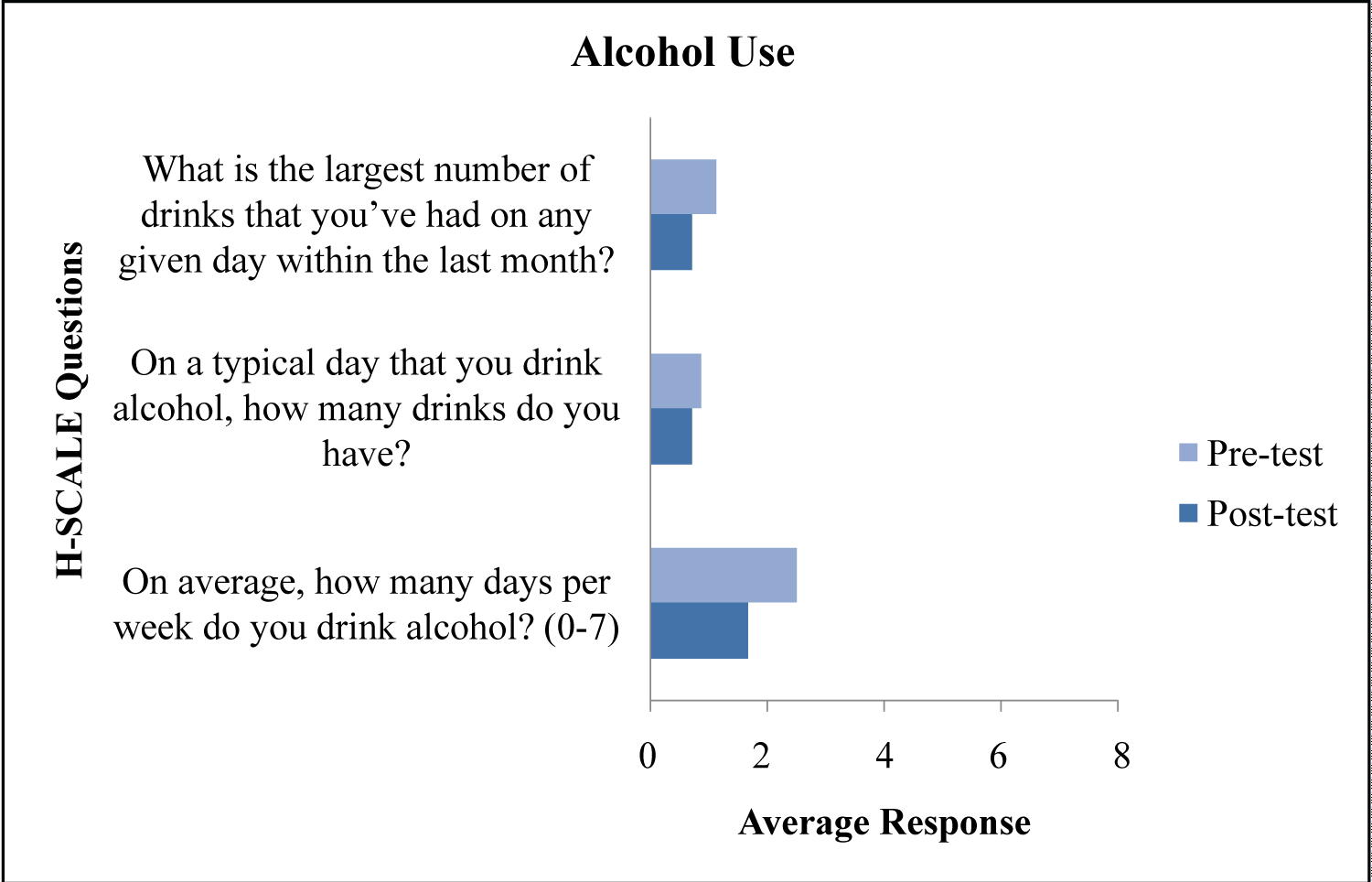 Figure 4: Alcohol use.
View Figure 4
Figure 4: Alcohol use.
View Figure 4
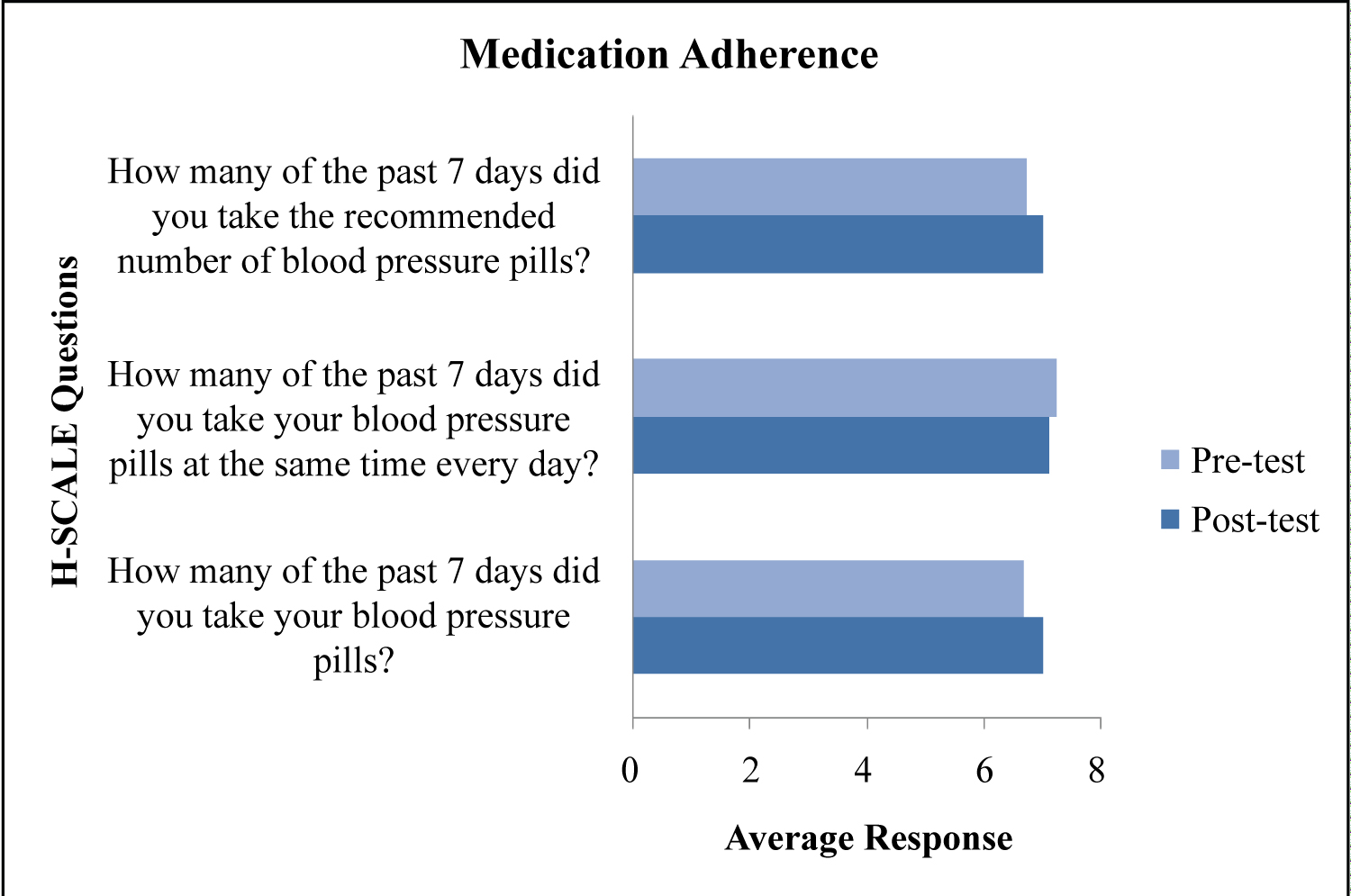 Figure 5: Medication adherence.
View Figure 5
Figure 5: Medication adherence.
View Figure 5
In addition to lifestyle changes, the average blood pressure improved after the intervention. The systolic blood pressure reduced by approximately 1.4 mmHg and the diastolic blood pressure reduced by approximately 4 mmHg. Despite the improvement in average blood pressure, this finding was not calculated to be statistically significant, with p equaling 0.2933. Though changes in blood pressure measurements were not a focus of the study's hypothesis, the values provided valuable insight into the possible physical changes related to improvement in hypertension health behavior management.
Though the study resulted in valuable information, outside variables may have also contributed to each subject's success. Influencing factors that may have improved patient health habits included advice from each subjects' primary care provider, family, friends, or media advertisements, or personal feelings or fears regarding health separate from the intervention. Other possible bias concerns are a lack of insight the subjects may have had regarding personal health habits or an incorrect recall of specific facts as asked on the pre-test and post-test.
This study poses limitations in sample size and data collection method. With a cohort of thirty participants, it is difficult to extrapolate the results on a larger scale [16]. The data collected may be specific to the participating population only, characteristics that included being an older hypertensive male in a rural part of America, factors that do not include other genders, chronic diseases, age groups, or non-rural parts of America. Additionally, there is no way to ensure that only the recruited subjects completed the pre and post-tests. If a relative or friend were to complete the tests for the subject, the data may represent incorrect conclusions. If the study were repeated, a larger sample size with subjects recruited from varying clinical site may be utilized to better represent a wider variety of individuals. Measures, such as verification of identity prior to completing the pre and post-tests, could also be implemented to ensure validity of the data.
The statistically significant data noted from this study supported the use of distance learning as a supplement to personal hypertension management. With the addition of supportive measures, such as a synchronous educational meeting with a nurse practitioner, patients suffering from a disease, such as hypertension, may learn information that adequately manages the disease if practiced. Providers may consider implementation of distance learning into clinical practices, and include scheduled one-on-one videoconference-based options for interested patients. Further studies should consider other medical illnesses and different demographics to assess the effectiveness of distance-based health education on differing health conditions.
Changes in health habits among hypertensive patients have been proven to lead to enhanced personal care and healthier blood pressure measurements [17-19]. Educational information on habit improvement to manage hypertension effectively was shared with thirty rural hypertensive patients via a distance learning-based teaching intervention with a nurse practitioner. Personal management of hypertension was assessed before and after the intervention in order to measure the effect of the educational program on health behaviors. Due to the overall positive outcome of the intervention on hypertension self-care habits, knowledge of the use of distance learning for rural communities may lead to a future of fully accessible provider-based medical information in areas of need.