It has been demonstrated that the non-invasive evaluation of aortic blood pressure has a prognostic value but limited by the inaccuracy linked to technical errors and a differences in the pressure wave analysis.
The aim of this study was to compare two methods used to validate the non-invasively central blood pressure waveforms obtained with an oscillometic device, with those recorded by intra-arterial measurements at the aortic level.
In this study were included 20 subjects, 10 males (68 ± 12-years-old, BMI: 27.4 ± 4.6 Kg/m2) and 10 females (77 ± 8-years-old, BMI: 28.5 ± 5.3 Kg/m2). The analysed cohort was composed of patients with diagnosis of coronary artery disease. Invasive and non-invasive data used in this research were previously analysed using a widely reported methodology and published by our group. The invasive aortic pressure recording was synchronically acquired with an oscillometric brachial acquisition and, then a reconstruction of central pressure wave was performed. In this research a correlation analysis using the entire aortic pressure cycle was performed.
Coefficient values found of the whole population, using the entire aortic pressure cycle, were similar to those obtained using the mean value of the cBP cardiac cycle (0.88 versus 0.89; respectively). On the contrary, the slope of the regression line determined by invasive versus non-invasive cBP loops (n = 20) using the entire cBP cycle exhibit a remarkable decrease with respect to that obtained using the mean aortic pressure cycle (0.98 versus 0.77).
In a first step, applying an interpolation procedure by means of oversampling and digital low pass filter, we found a high correlation between invasive and non-invasive instantaneous aortic pressure waveforms in: Men, women and the whole population, In a second step, results in terms of correlation coefficient and the slope derived from the regression analysis of invasive and non-invasive using a new data analysis allow to confirm high correlation coefficients and a more realistic slope value of the invasive versus non-invasive pressure wave relationship.
Central blood pressure, Mobil-O-Graph, brachial blood pressure, Aortic blood pressure
The use of reliable methodology to evaluate central blood pressure (cBP) is essential in several clinical situations, particularly in the field of systemic hypertension. Indeed, it has been reported that patients with normal brachial systolic blood pressure (< 120 mmHg) showed central systolic blood pressure values similar to patients with higher values of brachial systolic blood pressure (130-139 mmHg). These differences, and others, introduce a bias and certainly adversely influences correct risk stratification [1,2]. These increments of cBP expose the cardiac and brain structures to pulsatile hemodynamic stress rather than organs localized in peripheral territories [3]. Therefore, it has been proposed that cBP, could be a very important predictor of cardiovascular events, cardiovascular and non-cardiovascular mortality and a better estimator of left ventricular afterload, coronary and cerebral circulation, compared to peripheral blood pressure (pBP) [4-7]. Furthermore, the use of cBP provides a better guidance of hypertension management resulting in significantly different therapeutic interventions than those derived from brachial blood pressure; for instance, when drug titration is based on pBP there may be a risk of overtreatment [8].
During the last decades, the above-mentioned reports and many others allow to visualize that cBP should be considered as a marker of disease, since it was associated with organ damage, cardiovascular disease, and events in the general population [9]. Moreover, changes in the diagnosis of systemic hypertension have been proposed, found in the fact that current guidelines are based on pBP and, on the other hand, cBP of 130/90 was pointed out as the frontier of normality showing a high discriminatory power [10]. Considering that the clinical value of cBP is above and beyond the traditional pBP evaluation, there is consensus about the need of new and reliable technology that ensures the accurate non-invasive estimation of Cbp [11].
The automated oscillometric cBP measurement devices are widely employed in the clinical practice, however the accuracy of the devices is currently under investigations, which includes the use of invasive aortic measurements to appropriately validate new and old devices [11-14]. Currently, to calculate cBP using pBP measurements, the following procedure is described. Considering that pressure waves in brachial artery are compose of harmonics which are mathematically related whit those of similar frequencies obtained in aorta, a generalized transfer function could be calculated for each harmonic constituent. So, differences among peripheral and central harmonics, in terms of amplifications and phase spreading, allow to obtain a generalized transfer function. The reverse application of a generalized transfer function is what the mostly commercial equipment does: Get the peripheral wave, break it down into harmonics, and then apply a generalized transfer function (obtained from population studies), to obtain the aortic harmonics and after integrating them to obtain the cBP wave [13,15].
The technical procedure above described is applied in a non-uniform modality and the device validation is currently performed using more than one way of calibration and different generalized transfer functions. Consequently, many attempts were performed to improve the accuracy of every device destined to provide data relating to cBP, particularly in the field of the modes of calibration and the different mathematical transfer function employed in each research [11,12,16]. With respect to the transfer function used to calculate cBP considering peripheral measurement, they are subject to criticism since it is not possible to simulate the high number of changes determined by different hemodynamic conditions and pharmacological interventions [8,9]. Taking into account the large number of devices developed to measure pBP to calculate cBP, herculean efforts should be carried out in the future to overcome this challenge.
Finally, it important to comment that, despite many scientific demonstrations about the accuracy of different devices used to estimate cBP based on pBP, the prognostic value of this non-invasive evaluation of cBP seems to be underestimated due to the inaccuracy linked technical errors and a different pulse wave analysis has been proposed [13].
The aim of this study was to compare two methods used to validate the non-invasively central blood pressure waveforms obtained with a Mobil-O-Graph device, with those recorded by intra-arterial measurements at the aortic level. Invasive and non-invasive data used in this research were previously analysed using a widely reported methodology and published by our group [14].
In this study were included 20 subjects, 10 males (68 ± 12-years-old, BMI: 27.4 ± 4.6 Kg/m2) and 10 females (77 ± 8-years-old, BMI: 28.5 ± 5.3 Kg/m2). The analysed cohort was composed of patients with diagnosis of coronary artery disease. In Table 1, anthropometric and biochemical parameters of the subjects included in this research are shown. Cardiovascular risk factors associated were: systemic hypertension (n = 10), diabetes mellitus (n = 6) and dyslipidaemia (n = 15). All volunteers were submitted to a programmed percutaneous coronary intervention in the hemodynamic laboratory of our Institution. In any patient the pharmacological treatment was previously withdrawn. In all cases a specialized nurse practitioner provides a general guidance on the hemodynamic procedure to be performed, explained about the pressure measurement procedure and requested a written consent to be signed by the patients for: a) Cardiovascular catheterization including coronary angiography, b) Non-invasive pressure measurements using an oscillometric device (Mobil-O-Graph, Model PWA, IEM GmbH, Stolberg, Germany) and c) cBP invasive measurements. This research was approved by Institutional Ethic Committee. All procedures included in the investigation agreed with the Declaration of Helsinki (1975; reviewed in 1983).
Table 1: Anthropometric, biochemical, and hemodynamic parameter. View Table 1
Once a vessel (radial, ulnar or femoral artery) was chosen, a standard asepsis was performed in the area to be used for a standard endovascular procedure and a soft anesthesia (midazolam 1.5 mg and fentanyl 0.025 mg) was induced. Following, a pressure connector (AcistCV, i®, Medical System Inc., Germany) was flushed with saline solution and calibrated adjusting the baseline to zero (that is to say, atmospheric pressure). All patients remained in a supine position during the entire procedure.
After local anesthesia was applied in the vessel access area, a 5 or 6 French introducer sheath was positioned in the arterial lumen. Following, heparin (5.000 units) was administered through the arterial catheter. A 0.035-inch guide wire was positioned in the ascending aorta and a 5 French pig tail catheter (Cordis, Miami, USA), was placed 40 mm away from the aortic valve. Afterwards, the correct position of the catheter was confirmed, and the guide wire was removed and the pressure connector (AcistCV, i®, Medical System Inc., Germany) was positioned. During the procedure, the intra-arterial catheter was flushed with saline solution. Thereafter, multiple recording of aortic blood pressure were performed synchronized with the Mobil-O-Graph measurements. Non-invasive measurements were performed in the left or right brachial region in the contralateral position with respect to that used for arterial catheterization. Following, the pig tail catheter was removed and an angiographic diagnostic was carried out. In all patients coronary artery disease was confirmed and a percutaneous coronary intervention was carried out. Once all procedures were finished, the catheter was removed, and each patient returned to the outpatient area and was discharged from the institution.
No technical mistakes of collateral damages were observed during data acquisition and the percutaneous intervention.
In all patients included in this research pressure waveform were non-invasively obtained in the brachial artery using the oscillometic device (Mobil-O-Graph) and recorded for an offline analysis. The oscillometric technology used in this research consists of a brachial cuff-based central blood pressure estimating device, which is positioned in the upper limb contralateral to that used for the invasive arterial access. In all patients a properly sized cuff was fitted around the free arm, in accordance with the Manufacturer's Instruction Manual. The brachial pressure waveforms obtained with the oscillometric device were properly calibrated with the cuff-measured brachial systolic and diastolic blood pressure, respectively, and the central aortic waveforms were therefore calculated by the device's software.
Data acquisition was carried out in each patient by trained investigators and three blood pressure recordings were obtained in all cases. These blood pressure recordings were averaged to obtain the non-invasively measured systolic, diastolic, mean and pulse pressure values. To ensure a time-reference signal, all pressure waveforms were synchronically analysed using the QRS complex of the surface electrocardiogram.
Invasive and non-invasive central pressure waves were analysed using specific software manufactured in our laboratory. Central non-invasive pulse pressure was obtained by the oscillometric device. The electrocardiographic signals and the invasive central pressure waves were visualized in a Philips Allura Clarity FD20 monitor images. Invasive aortic pressure waves were converted to one-dimension pressure wave. Central pressure waves and electrocardiographic signals were interpolated in time in order to obtain the same number of data points, allowing to calculate an averaged cardiac cycle. The analysed pressure waveforms were in steady stated and no significantly variability was detected. Each Central pressure waveform was digitized at 100 Hz, for 30-60 seconds. In each analysed waveform the invasive systolic, diastolic, mean and pulse pressure values were calculated.
Finally, once the invasive and non-invasive central pressures from a single beat were obtained, an interpolation procedure was developed to compare them, and an analysis was carried out to calculate the blood pressure parameters during the 30-60-s recording period in each case [14].
Data reported in this research are mean ± SD. Unpaired Student t-test and Bland & Altman analyses were used to compare invasive and non-invasive central pressure values. Statistical analysis was carried out using an IBM-SPSS software (IBM Corp. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp; United States). In the statistical analyses p < 0.05 was considered as a limit of statistical signification.
This research was carried out in accordance with the ethical principles of the Declaration of Helsinki and the US Code of Federal Regulation (part 46, protection of human subjects) and within the principles outlined by the International Conference on Harmonisation Guidelines for Good Clinical Practice. Data acquisition began after the research protocol was reviewed and approved by the Institutional Committee for Human Investigations of the University Hospital, Favaloro Foundation. The approval resolution was identified as: DDI (1351) 2616 CBE 630/16.
Before the admission in the hemodynamic laboratory, the brachial pressure, anthropometric and biochemical parameters were recorded in all subjects included in this research (n = 20). As seen in Table 1 the female cohort was significantly older than male subjects (p < 0.05). On the other hand, values of weight and height in male cohort were significantly higher than female cohort (p < 0.01). Total cholesterol and LDL cholesterol mean values obtained in the female cohort showed higher values than those found in males (p < 0.05 and p < 0.01; respectively). Values of brachial systolic and pulse blood pressure recorded before the hemodynamic laboratory admittance in the female cohort were significantly higher than those measured in the male cohort (p < 0.05 and p < 0.01; respectively).
Invasive and non-invasive pressure signals obtained in every subject included in this research were appropriately recorded and digitized for off-line analysis.
Invasive mean values of cBP recorded in the whole population showed non-significant differences with respect to those obtained using the oscillometric device (Table 1). Mean invasive value of central systolic blood pressure measured in the male cohort, was significantly higher than that non-invasively obtained in the same subjects (p < 0.05); however, mean central diastolic blood pressure invasively measured in the male cohort was lower than that non-invasively obtained (p < 0.05). Mean values of invasive central systolic and pulse blood pressure observed in the female cohort, were higher than those non-invasively obtained (p < 0.01 and p < 0.001; respectively); while invasive central diastolic blood pressure values were lower than those non-invasively obtained (p < 0.001) (Table 1).
Comparison of male and female cohort showed differences in terms of invasive and non-invasive pressure values. Mean invasive values of central systolic blood pressure and pulse pressure obtained in females, were higher than those observed in males (p < 0.01 and p < 0.001; respectively). Significant differences were also observed when analysing non-invasive values obtained in the female cohort that showed higher systolic, mean and pulse pressure values than those calculated in males (p < 0.01, p < 0.05 and p < 0.01; respectively) (Table 1).
Invasive and non-invasive pressure waves measured and calculated (respectively) in ascending aorta were used in a correlation analysis using all point of each digitized cycle. This procedure was applied to the whole population and in the male and female cohort. As can be seen in Figure 1A, Figure 2A and Figure 3A, invasive and non-invasive pressure waves generated loops, whose analysis is described in the following paragraphs.
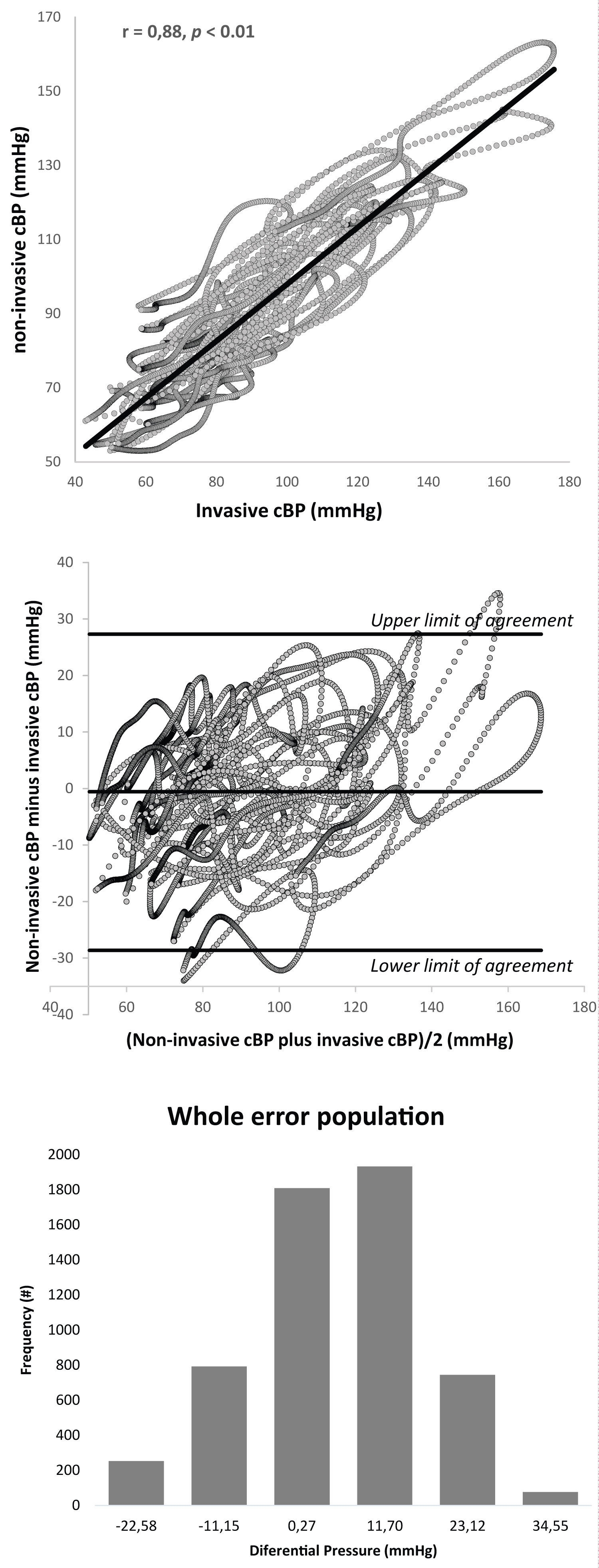 Figure 1: In the upper panel, instantaneous central blood pressure (cBP) values invasively obtained in the whole population are correlated with those obtained in the same population using the oscillometric device. Loops were obtained in the 20 analysed patients (males and females) and the regression line (in black) was calculated. Middle panel: Bland-Altman plots of differences between non-invasive instantaneous central blood pressure and invasive values obtained in males and females are shown. Lower panel: Mean differences between non-invasive instantaneous central blood pressure and invasive values corresponding to the entire population were in the 95% confidence interval, showing a normal distribution.
View Figure 1
Figure 1: In the upper panel, instantaneous central blood pressure (cBP) values invasively obtained in the whole population are correlated with those obtained in the same population using the oscillometric device. Loops were obtained in the 20 analysed patients (males and females) and the regression line (in black) was calculated. Middle panel: Bland-Altman plots of differences between non-invasive instantaneous central blood pressure and invasive values obtained in males and females are shown. Lower panel: Mean differences between non-invasive instantaneous central blood pressure and invasive values corresponding to the entire population were in the 95% confidence interval, showing a normal distribution.
View Figure 1
In the whole population (n = 20), correlation between instantaneous invasively and non-invasively cBP values showed a significant correlation (0.88; p < 0.01), as seen in Figure 1 upper panel. The regression analysis carried out using 20 invasive and non-invasive cycles (loops) showed that the slope was 0.77, showing that cBP values non-invasively obtained were lower with respect to those obtained with the intra-aortic catheter (Table 2). Once the underestimation of non-invasive approaches was confirmed, a Bland & Altman analysis was carried out, showing that mean differences (invasive minus non-invasive central aortic pressure values) were distributed in-between the 95% confidence interval (Figure 1 middle panel) and exhibit a normal error distribution (Figure 1 lower panel).
Table 2: Comparison between two approaches used to validate cBP assesses. View Table 2
In the male population (n = 10), correlation between instantaneous invasively and non-invasively cBP values showed also a significant correlation (0.89; p < 0.01), which are seen as loops in Figure 2 upper panel. The regression analysis carried out using 10 invasive and non-invasive cycles (loops) showed that the slope was 0.77, demonstrating that cBP values non-invasively obtained were lower with respect to those obtained with the intra-aortic catheter (Table 2, upper panel). The Bland & Altman analysis showed that the mean differences (invasive minus non-invasive central aortic pressure values) were distributed in-between the 95% confidence interval (Figure 2 middle panel) and exhibits a normal error distribution (Figure 2 lower panel).
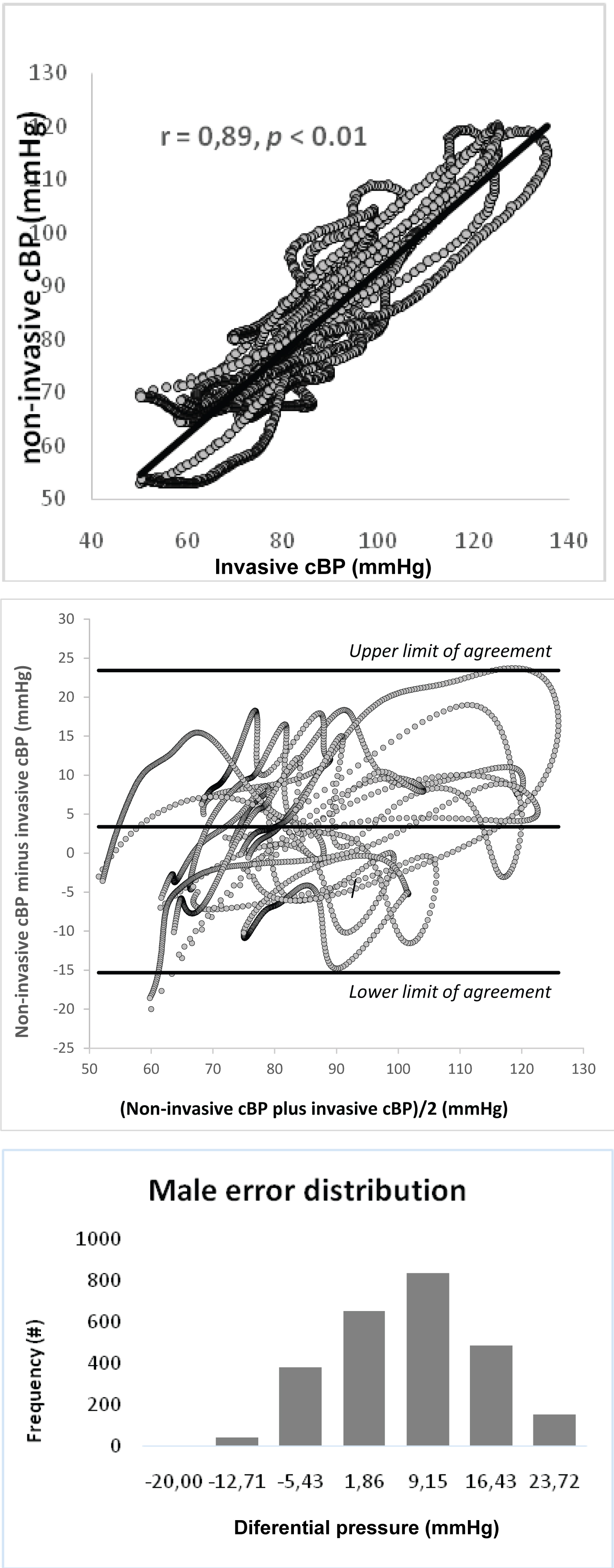 Figure 2: In the upper panel, instantaneous central blood pressure (cBP) values invasively obtained in males are correlated with those obtained in the same population using the oscillometric device. Loops were obtained in 10 analysed patients (males) and the regression line (in black) was calculated. Middle panel: Bland-Altman plots of differences between non-invasive instantaneous central blood pressure and invasive values obtained in males are shown. Lower panel: Mean differences between non-invasive instantaneous central blood pressure and invasive values obtained in the male cohort (n = 10) were in the 95% confidence interval, showing a normal distribution.
View Figure 2
Figure 2: In the upper panel, instantaneous central blood pressure (cBP) values invasively obtained in males are correlated with those obtained in the same population using the oscillometric device. Loops were obtained in 10 analysed patients (males) and the regression line (in black) was calculated. Middle panel: Bland-Altman plots of differences between non-invasive instantaneous central blood pressure and invasive values obtained in males are shown. Lower panel: Mean differences between non-invasive instantaneous central blood pressure and invasive values obtained in the male cohort (n = 10) were in the 95% confidence interval, showing a normal distribution.
View Figure 2
In the female cohort (n = 10), correlation between instantaneous invasively and non-invasively cBP values showed also a significant correlation (0.92; p < 0.01), as seen in Figure 3 upper panel. The regression analysis carried out using 10 invasive and non-invasive cycles (loops) showed that the slope was 0.79, showing that cBP values non-invasively obtained were lower with respect to those obtained with the intra-aortic catheter (Table 2). The Bland & Altman analysis showed that mean differences (invasive minus non-invasive central aortic pressure values) were distributed in-between the 95% confidence interval (Figure 3 middle panel) and exhibit a normal error distribution (Figure 3 lower panel).
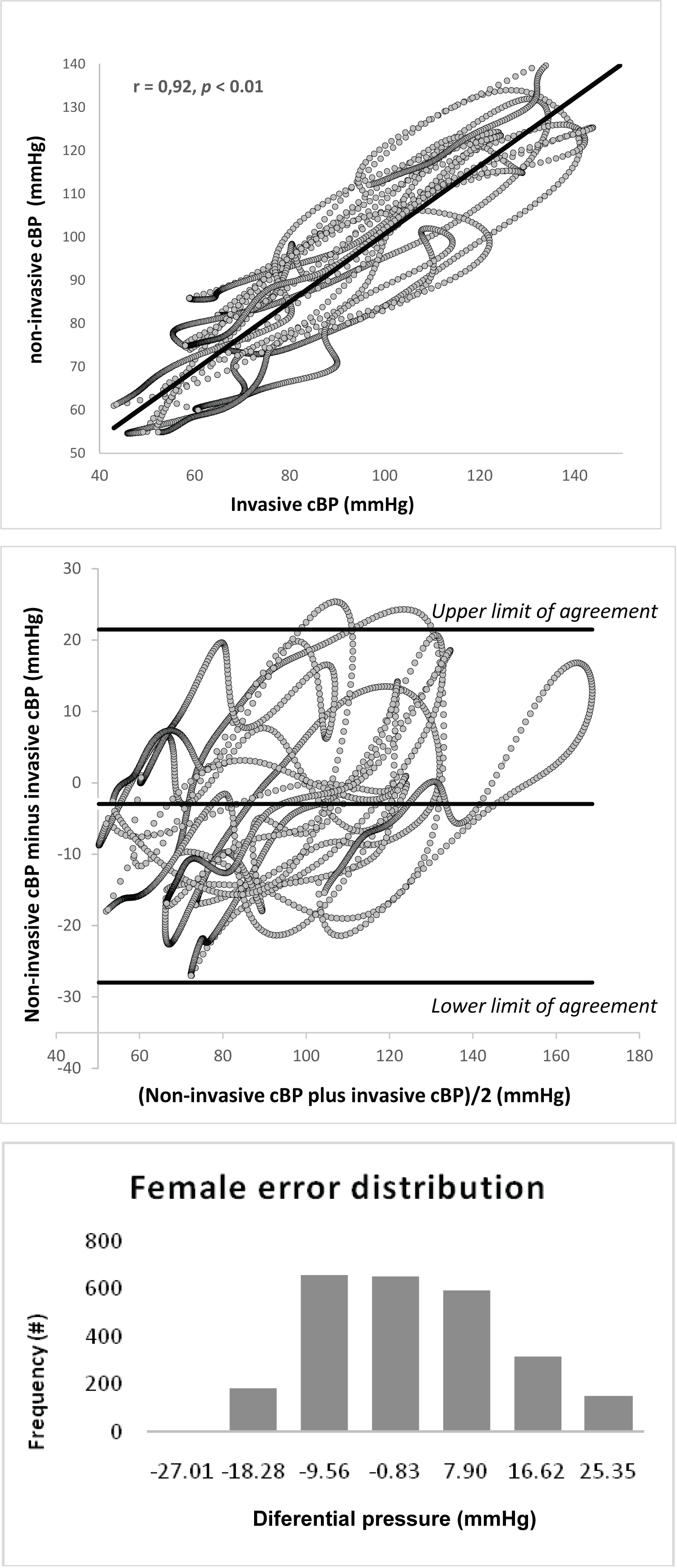 Figure 3: In the upper panel, instantaneous central blood pressure (cBP) values invasively obtained in females are correlated with those obtained in the same population using the oscillometric device. Loops were obtained in 10 analysed patients (females) and the regression line (in black) was calculated. Middle panel: Bland-Altman plots of differences between non-invasive instantaneous central blood pressure and invasive values obtained in females are shown. Lower panel: Mean differences between non-invasive instantaneous central blood pressure and invasive values obtained in the female cohort (n = 10) were in the 95% confidence interval, showing a normal distribution.
View Figure 3
Figure 3: In the upper panel, instantaneous central blood pressure (cBP) values invasively obtained in females are correlated with those obtained in the same population using the oscillometric device. Loops were obtained in 10 analysed patients (females) and the regression line (in black) was calculated. Middle panel: Bland-Altman plots of differences between non-invasive instantaneous central blood pressure and invasive values obtained in females are shown. Lower panel: Mean differences between non-invasive instantaneous central blood pressure and invasive values obtained in the female cohort (n = 10) were in the 95% confidence interval, showing a normal distribution.
View Figure 3
In a previous research we used an approach currently employed to assess cBP to study data obtained in the same subjects included in this research. In the reported investigation data analysis was carried out using the mean cBP value of each aortic cycle (invasively measured and no-invasively calculated). The results obtained in terms of correlation coefficient and the regression analysis of invasive versus non-invasive cBP slope are partially reproduced in Table 2, lower panel [14]. In the new research here presented, correlation coefficient values found in the whole population, using the entire aortic pressure cycle (instead of the mean value), were like those obtained when the mean value of the cBP cardiac cycle was analysed (0.88 versus 0.89; respectively), as can be seen in Table 2. On the contrary, the slope of the regression line determined by invasive versus non-invasive cBP loops of the whole population (n = 20) using the entire cBP cycle were significantly lower with respect to that obtained using the mean aortic pressure cycle (0.77 versus 0.98; p < 0.05). This difference was also observed in the female cohort in which the value of the slope calculated using the entire cBP cycle was significantly lower than that obtained using the mean value of cBP cycle (0.79 versus 0.98; p < 0.05). Interestingly, as can be seen in Table 2, this remarkable and significative difference between two different approaches used to analyse de invasive versus non-invasive cBP relationship, was obtained in a cohort of females with similar correlation coefficient. Indeed, in this research, the correlation coefficient of the female population in which we used the entire aortic pressure cycle was 0.92, which is very similar to that obtained using the mean value of the cBP cycle (slope = 0.93). See Table 2.
Non-invasive assessment of cBP is traditionally obtained using a calibration technique based on systolic and diastolic pBP values, however, it is accepted that available devices underestimate systolic and overestimate diastolic cBP [12]. The mentioned inaccuracy has been attributed to the calibration method and different approaches were developed to improve the ability of each device to provide reliable cBP evaluations. In 2015, Wassertheurer reported that cBP estimation based on oscillometric brachial blood pressure measurements using a common cuff independently predicted mortality and provided a high prognostic value when non-invasive mean and diastolic pressure were used to calibrate an oscillometic device [17]. Unfortunately, the device calibration is not the only source of error in the estimation of cBP; indeed, the generalized transfer function used to calculate cBP have been also subject to doubts about the ability to simulate hemodynamic changes determined by physiological and pharmacological modifications [15,18,19]. With respect to this bias in the cBP estimation, an interesting research was reported by Cheng and co-workers, in which they estimated the aortic pulse pressure using a generalized transfer function and new pulse wave analysis [13,20]. Interestingly, in the mentioned research using an oscillometic device, data acquisition was performed before and after nitroglycerin administration and the conclusion of the investigation was an improvement in the accuracy of the non-invasive central pulse pressure estimation using the new approach proposed by the authors [13].
As was described in the last paragraph, according to the specialized literature, error sources involve the calibration procedure and the generalized transfer function. In our research we proposed a new approach that focuses the attention in the analysis of the invasive aortic pressure wave and the non-invasive cBP wave obtained with an oscillometric device. The mentioned invasive and non-invasive data, used in this research, were previously analysed using a widely reported methodology and published by our group [14]. Briefly, in the mentioned report, invasive cBP waves were digitized at a sample time of 5msec, and approximately 10-15 consecutive beats were assessed in each subject. Instantaneous oscillometic brachial pressures waveforms were obtained and their central aortic waveforms were reconstructed by the device's software in one single beat. An interpolation procedure was made in invasive cBP signals for obtaining the same number of data points as in the non-invasive pressure wave in the same cycle. Therefore, comparisons between invasive averaged cardiac cycle and oscillometric single beat pressure signal were achieved for statistical analysis. Following a regression analysis between invasive and non-invasive data were carried out using only one value of each pressure cycle (beat). In other words, the regression line of twenty invasive measurements of cBP versus twenty no-invasive cBP estimations were carried out using singles points corresponding each of them to one cycle [14]. On the contrary, in this research invasive versus non-invasive waves of each cycle (showing a loop configuration) were used to obtain a regression line using every point each cycle (Figure 1A, Figure 2A and Figure 3A).
Results obtained in this research are similar to that reported in last years by different groups of clinical investigation. A recent validation study reported by Dörr, et al., in which an oscillometric device was used in 191 patients and an invasive validation was carried out of the Antares algorithm in the custo screen 400 (custo med GmbH, Ottobrunn, Germany). The Antares algorithm is used to calculate cBP and in the research of Dörr, et al., was compared with invasive aortic records. This research showed a level of agreement that faces the highest requirements defined as the mean value of differences within 5 mmHg and standard deviation of less than 8 mmHg [21]. Other research validated two new non-invasive technologies, the SphygmoC or XCEL device and the Mobil-O-Graph NG device, versus invasively data obtained in subjects who were recruited for coronary angiography [12] and the authors found that the mean differences was 5-6 mmHg in systolic and 1-4 mmHg in diastolic cBP, which are similar to our study.
The relevance of our research in not only to obtain levels of agreement between invasive and non-invasive cBP values using an original methodology but, the accuracy of the slope obtained in the regression analysis. As can be seen in Table 2, invasive versus non-invasive regression analysis showed slope values of 0.77, 0.77 and 0.79 in the whole population, in the male and female cohort; respectively. All these values were obtained after high correlation coefficients were found in the whole population (r = 0.88), the male cohort (0.89) and the female cohort (r = 0.92). These correlation coefficient values are very similar to that observed in the previous report of our group, in which the same data here used were analysed employing the traditional methodology (only one cBP value in each cycle) using the same data here analysed. However, values of the invasive versus non-invasive slopes were very different in the whole population and in the female cohort (p < 0.05 and p < 0.05; respectively). These findings suggest that the use of every point of the cBP loop to calculate the slope of the invasive versus non-invasive pressure relationship allow a more homogenous and reliable results. This is not a minor point, since the hemodynamic changes determined by physiological and pharmacological modifications have been considered the frontier of the reliability of the traditional method. Perhaps, the use of all points of the digitized cBP loop here analysed would be more adequate during transient hemodynamic states.
All patients included in this research were at recumbent position due to the characteristics of the invasive procedure performed in parallel with non-invasive pBP measurements. Moreover, the use of cuff-measured brachial systolic and diastolic pBP for calibration of the waveforms is another limitation of this research because this type of calibration introduces error because of the underestimation of intra-arterial brachial systolic blood pressure and overestimation of intra-arterial brachial diastolic blood pressure [22].
In a first step, the use of invasive aortic pressure waves obtained in this research allows to compare them with those provided by an oscillometric device at recumbent position. Digitized data of the whole wave in every cycle allowed to obtain, point by point, an aortic invasive versus non-invasive pressure loop and a comparison of central systolic, diastolic, mean and pulse pressure values invasively measured with those non-invasively recorded was carried out. Obtained data were similar to those reported in the specialized literature. Moreover, applying an interpolation procedure by means of oversampling and digital low pass filter, we found a high correlation between invasive and non-invasive instantaneous aortic pressure wave forms in: men, women and the whole population.
In a second step, results obtained in this research in terms of correlation coefficient and the slope derived from the regression analysis of invasive and non-invasive were compared with those previously reported by our group using the same population. The original data analysis procedure used in this research allow to confirm high correlation coefficients in both studies and the regression analysis provided a more realistic slope value of the invasive versus non-invasive pressure wave relationship when we used every point of the pressure waves in the confection of each loop.
Briefly, our findings allow an accurate calibration of analysed oscillometric devices and provides a more realistic aortic waveforms and central pressure parameters (systolic, diastolic, mean and pulse pressure), using the correlation analysis here reported.
Findings obtained in this research using a widely employed oscillometric device could allow a more precise detection of organ damage associate to high aortic blood pressure and a different approach to analyse hemodynamic changes determined by physiological and pharmacological modifications.
This work was supported by the RG favaloro University Foundation, Buenos Aires, Argentina.
No funding was received.
All authors have no conflicts of interest or financial ties to disclose.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and their later amendments or comparable ethical standards.