Background: Elderly stroke outpatients, without aphasia, hemiplegia, or spatial neglect in their post-acute phase, are typically monitored on a quarterly, or fewer, physician-visit schedule. Thus, the patient's status goes unreported between visits unless a remarkable untoward event occurs.
Methods: We devised an electronic diary (e-diary) to serve as an adjunct to physician visit-to-visit management of BP in elderly stroke patients. In phase 1 implementation, the e-diary was used by eight adults up to three times per day to monitor BP (via Bluetooth), to report biopsychological factors, and then to coach BP self-management. In phase 2, the e-diary supported BP self-management.
Results: E-diary monitoring provided earlier detection of four, otherwise undetected, spikes in SBP and HR that generated prompter referrals in three patients. E-diary-mediated coaching of improved health practices produced BP self-management gains: 5/6 patients showed statistically significant reductions in BP. The statistically significant reductions in SBP were into the 120-129 mm Hg range in three and were below 120 in a fourth. In a sixth patient, self-management reduced the number of SBP spikes (i.e., SBP ≥ 130). The data of a seventh patient revealed that their frequent, undiagnosed episodes of altered consciousness - i.e., feeling "not-with-it" - were correlated with variations in their lower, but broad-ranged SBP.
Conclusion: Our findings illustrate the efficacy of our e-diary-based adjunct for elderly stroke patient BP self-management and for facilitating differential diagnosis involving SBP. They also suggest the feasibility of using a customized diary remotely, for chronic diseases more broadly in an aging population.
Hypertension, Electronic monitoring, Post Stroke Intervention, Self-management, Digital Diagnostics and Biomarkers
BP: Blood Pressure; SBP: Systolic Blood Pressure; DBP: Diastolic Blood Pressure; EBP: Elevated Blood Pressure; WM: White Matter; SDH: Subdural Hematoma; MCA: Middle Cerebral Artery; HTN: Hypertension; PFO: Patent Foramen Ovale
Elevated blood pressure (EBP) is the leading modifiable risk factor for stroke [1,2]. Lowering BP has been shown to reduce the risk of recurrent stroke by 25-30% [3]. The risk of EBP and the need for its reduction is also broader. It extends to patients with EBP-related Transient Ischemic Attack (TIA) [4] who, after the initial symptoms have resolved, show compromises in energy, mental health, and executive functioning in psychometric testing [5]. In addition, EBP in mid-life is associated with vascular dementia in later years [6].
Despite this relationship between EBP and stroke, BP remains insufficiently controlled in 46% of US adults [7]. Previous research has demonstrated that electronic self-monitoring of BP and education facilitates the reduction of BP [8-10] when they are used as an adjunct to physician visit-to-visit care.
Our NIH-funded, feasibility study demonstrated that elderly stroke patients can be coached to improve their BP management through the daily use of a patient e-communication system that is an adjunct to physician visit-to-visit care. Our study, however, added a new feature to the methodology of BP management via e-communication adjuncts. Besides recording BP and HR, we asked patients to report simultaneously the status of three biopsychological factors in an e-diary. They rated feelings (e.g., sad/happy, anxious/secure, angry/calm) three times/day. They also made morning sleep reports and checked off the day's activities at bedtime. These biopsychological data enabled us to create an individualized, e-diary, coaching adjunct. Significant correlations of biopsychological data with SBP revealed which of these factors had the greatest influence on the patient's SBP. These influences in turn were targeted with improved health practices to reduce the patient's SBP. For example, if exercise was correlated with SBP, then self-management involved improved exercise practices.
We implemented the use of this individualized diary adjunct in two phases. In phase 1 we attempted to identify the biopsychological factors that exerted the greatest influence on a patient's BP level. We also provided patients feedback about their recordings and reports via telephone, which we augmented with graphics of the patient's data. Based upon these individual data we coached patients to adopt specific healthier practices that would reduce BP.
In phase 2 we monitored a patient's ability to follow our coaching recommendations. We also monitored how well a patient was able to reduce BP with our recommendations. We attempted to reduce BP with this individualized, e-diary-mediated, coaching adjunct. Accordingly, we present the results of these intensive discrete efforts in a detailed series of longitudinal follow-ups. We also report how one patient's SBP variability was analyzed to determine if, and how, SBP variability may be related to a puzzling symptom expression pattern.
This was a prospective study of eight patients, seven of whom had experienced a mild stroke and one with a moderate stroke, who were referred for blood pressure management with an e-diary system.
All were referred by the two neurologist authors. Inclusion criteria were: having experienced a stroke with no paresis, aphasia, or field cuts; living in the community, requiring blood pressure management; and being current users of either a smartphone or computer with access to the internet.
Patients were evaluated by a neurologist and a neuropsychologist. An assistant evaluated: balance with the Berg Balance Test [11], fatigue with the Fatigue Severity Scale [12], quality of life with the PROMIS Scale v21.2 Global Health [13], and functional activities with the Late Life Function and Disability Instrument [14].
Patients were monitored as follows. Patients made reports three times/day: morning, midday, and bedtime in an electronic diary (e-diary) that was connected to the SymTrend e-diary system [15]. Each patient's e-diary was individually tailored to the patient's characteristics and circumstances. They reported sleep adequacy (hours of sleep, sleep impairments), activity level (type, hours, activity demands), and stress intensity (none to very severe). They also reported feeling states (e.g., happy/sad, anxious/secure, angry/peaceful, calm/tense, energetic/tired, alert/sleepy, and in control/overwhelmed) on bidirectional, nine-point, Likert-like rating scales. For example, the energy/tired scale ranged from Very Tired (-4) to Very Energetic (+4) with one intermediate level. Co-morbidities, when present, were variously reported on a rating scale (e.g., headache (HA), 0 to 10), or a checklist (e.g., anatomical HA sites). Finally, patients used Bluetooth-enabled devices to report blood pressure and pulse (Qardio Arm blood pressure cuff), steps (AmazFit Blip step tracker), weight (Qardio Base 2 scale), as well as blood sugar (One Drop glucose monitor) in one patient with Type 2 Diabetes. The diary and device data were aggregated by the patient's iPhone in six of seven patients. One patient keyboarded data directly into the SymTrend website.
Patients were monitored for two 12-week pre-post phases. In the pre-phase, "phase 1," we monitored a patient's SBP. We also monitored several biopsychological factors that served as indices of unhealthy practices (i.e., unhealthy situations and behaviors). Correlating SBP with the biopsychological factors enabled us to identify those practices that were significant influences on the patient's SBP elevation. In phase 1 we also coached the patient to adopt healthier practices, the selection of which was made based on our identification of the unhealthy influences that were correlated with the patient's SBP. In the post-phase, phase 2, patients switched to the self-management of healthier practices to reduce SBP. During phase 2 patients received minimal assistance from the researchers. They received updates every other week. If a patient's progress was desultory, the patient received a weekly advisory about how to upgrade health practices in the coming week. A patient's progress from phase 1 to phase 2 was assessed by comparing the patient's phase 2 SBP average with the patient's phase 1 SBP average using a t-test comparison at the p < 0.05 level of statistical significance.
Patients who spiked SBP or HR levels during phase 1 were identified from their e-diary data for prompt medical attention. A PDF of SBP and HR graphics was emailed to the patient for review with his/her prescribing physician.
We recruited 7 elderly patients (≥ 65 yrs.) with a goal of recruiting 10. Four individuals with BP management needs were unable to participate because they did not own a smartphone or did not have access to the internet. Unfortunately, the COVID pandemic interfered as well. We added an 8th patient who was ≤ 65 yrs. at the request of one of the participating neurologists. Table 1 displays the patient demographics and relevant medical history (gender, age, stroke type, time post stroke at first data recording, and cardiac status). Seven patients completed the study. P8 found the technology too challenging to master during phase 1, despite three training sessions-all other patients learned in a single session.
Table 1: Patient demographics and relevant cardiac and neurological status. View Table 1
Adherence to recording protocol during phase 1 met the recommended rate of 80% [16] for six of seven participants; some tapered off in phase 2. Patients recorded a median of 93% of the days in Phase 1 (Range: 76%-99%). They recorded a median of 96% of days in phase 2 (Range: 30%-100%). Two patients showed a considerable adherence rate taper in phase 2 relative to phase 1, but still provided adequate data (P4: 67 to 43 days, 80% vs. 51%; P5: 64 to 27 days, 76% vs. 30%).
Overview: During the phase 1 period, three patients demonstrated signs of an event that required prompt medical attention. These events included a marked BP spike (3 patients) and a dramatic resting HR increase (1/3).
Patient P1 developed pneumonia. P1 was prescribed a steroid that spiked their blood pressure unbeknownst to their PCP prescriber. When P1 forwarded her SBP monitoring data to their PCP, P1 discontinued the steroid, which reduced their BP.
Patient P2 had a family history of stroke-related morbidity. In addition to BP monitoring which was part of this study, P2 also monitored their cardiac rhythm electronically. P2 had two event detections during the phase 1 period. The first event was a spike in SBP that led to a report to the cardiologist who increased his antihypertensive medication. The second event was a marked elevation in resting HR (180s) which led to a two-day hospital admission for surveillance and management.
Patient P3 was undergoing medication adjustment to lower their SBP before entering our study for adjunctive e-diary-mediated SBP management. P3 had taken a combination of amlodipine, 5 mg, and losartan, 50 mg, both at bedtime. Inauguration of this medication regimen was associated with the start of morning headaches, believed to be associated with low morning BP. P3 was instructed to take their BP when they got morning headaches. If their BP was low, P3 was instructed to split the losartan dose between the morning and bedtime. This dosage split reduced morning headaches. Unbeknownst to P3's caregivers, however, the losartan split elevated their bedtime SBP because P3 failed to take the losartan as instructed. P3 forgot to take the morning losartan dose when they did not have a headache which led to a marked BP elevation at bedtime, which was not detected until P3 began BP monitoring in our study.
Overview: Six patients who completed the study had been referred for adjunctive BP reduction management. Patient, P7, was referred for evaluation of their low-range SBP to determine whether SBP variation was correlated with episodes of puzzling, intermittent symptoms.
BP reduction: BP reduction data for P1 to P6 are presented in separate figures and focus on average SBP reduction. The healthier practice changes that had the strongest associations with average SBP reduction in each patient are listed in an adjacent table on the right. The latter changes include improvements in feelings (e.g., feeling more secure, feeling more in control), in sleep (e.g., more sleep hours or better morning alertness), and in exercise (e.g., more steps, more time exercising). Patient tables are presented in pairs to highlight similarities and differences across patient outcomes. The direction and statistical significance of DBP changes for all patients, except P6, were parallel to those of their SBP changes. P6's DBP results are discussed below.
Comment P1 and P2 (Figure 1) P1 and P2 both showed a statistically significant reduction in SBP from the pre-phase (phase 1) to the post-phase (phase 2) in both the AM and PM periods. P1's average reductions were small in both the AM and PM periods, 4.4, and 2.7 points, respectively. The reductions did not reach our target level of below 120 mm Hg. They were, however, lowered into, or were lower within, the 120 to 129 mm Hg target zone (AM and PM respectively). The average reductions were associated with significant improvements in energy and sleep as well as a significant reduction in headache pain.
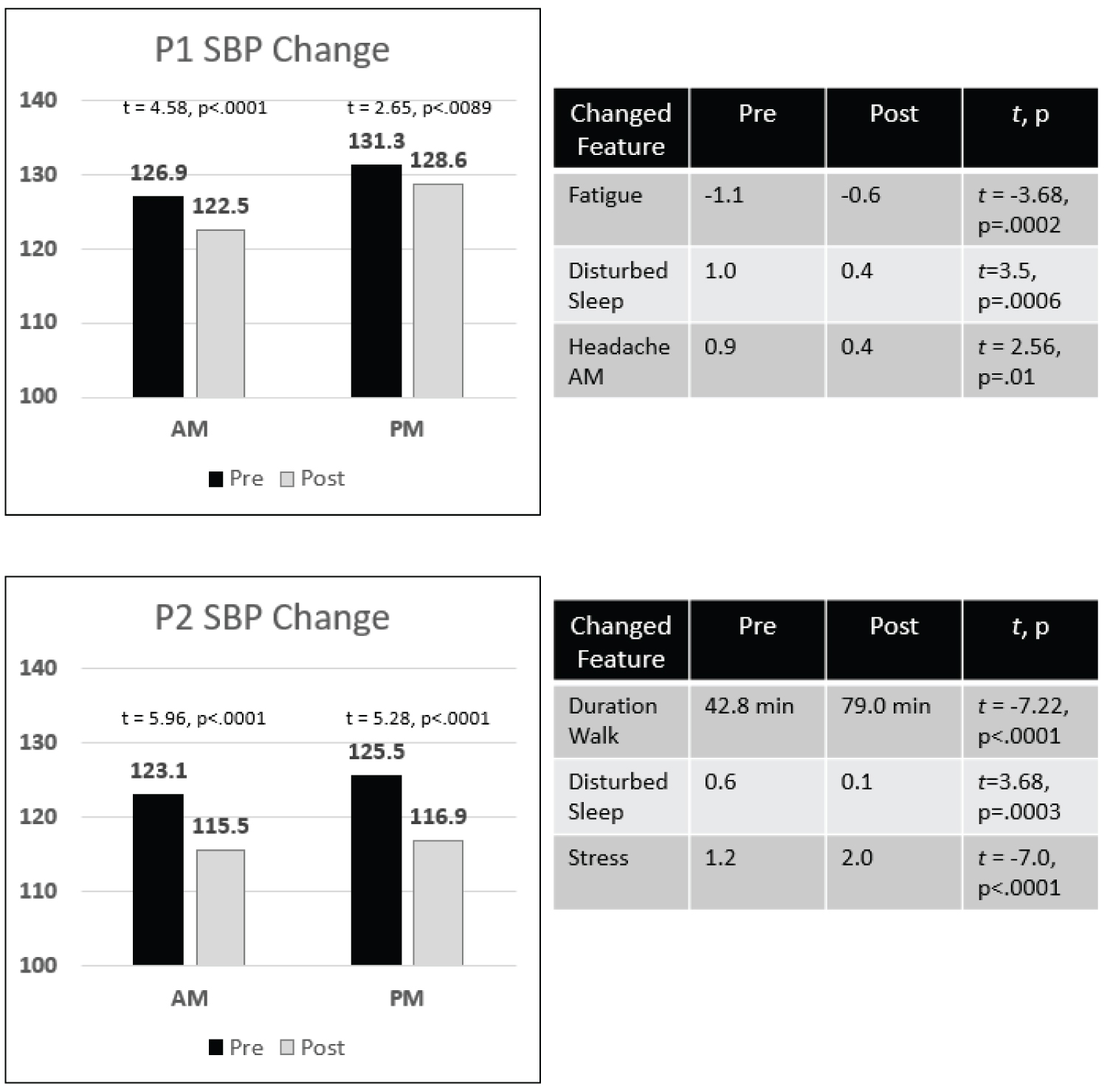 Figure 1: P1 and P2: Significant SBP reduction in AM & PM. View Figure 1
Figure 1: P1 and P2: Significant SBP reduction in AM & PM. View Figure 1
P2's average reductions were substantial: 7.6 mm Hg AM and 8.6 mm Hg PM. Both reductions reached our below 120-target level: 115.5 and 116.9 points respectively. These reductions were associated with a significant increase in exercise duration. They were achieved despite small, but significant, increases in sleep disturbance and stress.
Comment P3 and P4 (Figure 2) P3 had already achieved a lowered SBP in the AM through medication management. P3's phase 1 and phase 2 average AM SBPs were 119.8 and 120.8 mm Hg, respectively. P3's problem was a SBP of 138 mm Hg in the PM of phase 1. E-diary-based monitoring and coaching produced an 8.6-point average SBP reduction to 129.5 mm Hg (just above the 120 to 129 mm Hg target range). This sizable reduction was associated with several significant biopsychological improvements: reductions in discomfort (body aches/pains), gait unsteadiness, and headache pain, with an accompanying increase in step count.
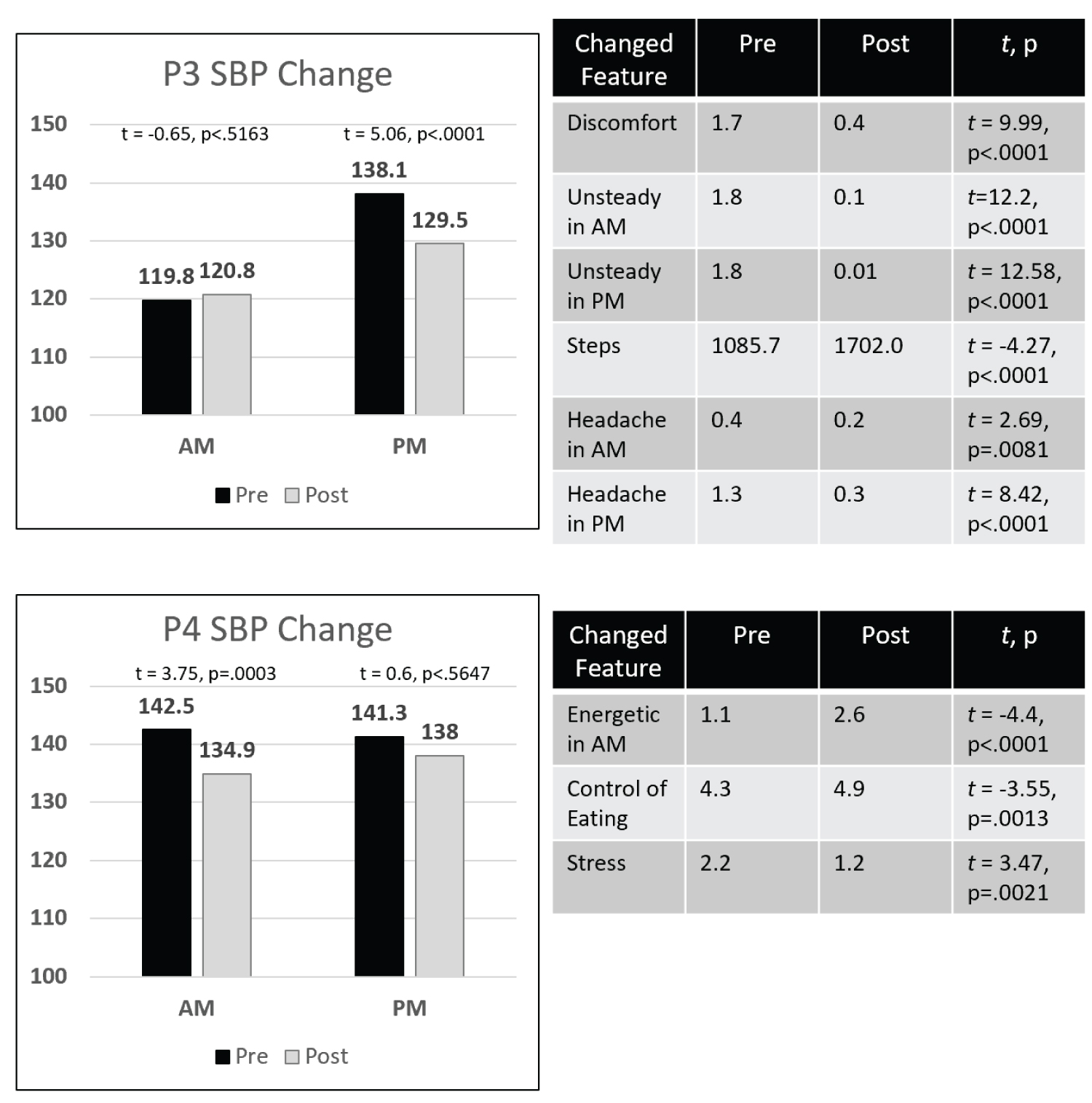 Figure 2: P3 and P4: SBP reductions at one time of day. View Figure 2
Figure 2: P3 and P4: SBP reductions at one time of day. View Figure 2
P4's goal was to reduce both his AM and PM SBP. P4 decreased their average AM SBP by 7.6 points from 142.5 to 134.9 mm Hg which was statistically significant, but did not reach our target range, 120 to 129 mm Hg. P4's average PM reduction was small (3.3 points) and not significant. P4's AM SBP reduction was associated with significant improvements in AM energy, improved eating between meals, and stress reduction.
Comment P5 and P6 (Figure 3): In phase 2, P5 showed a statistically significant, 5.6 mm Hg increase in average AM SBP. P5 showed no phase difference in average PM SBP, however. During phase 2, P5 was promoted to a department head position. The added stress of this promotion is the likely reason for P5's increased AM SBP and their increased use of compensatory strategies. Although P5 is under 65, P5's neurologist had lobbied for P5's inclusion in our study because he felt that P5 was not following BP management recommendations as specified. He expected P5's BP to rise if there were an increase in home, or work, stress. Work stress occurred and induced a persisting AM SBP elevation, despite our adjunctive, e-diary-mediated coaching. Both of P5's phase 2 SBP averages were, however, within the target region: 120 to 129, despite the stress-related increase in compensatory strategy use.
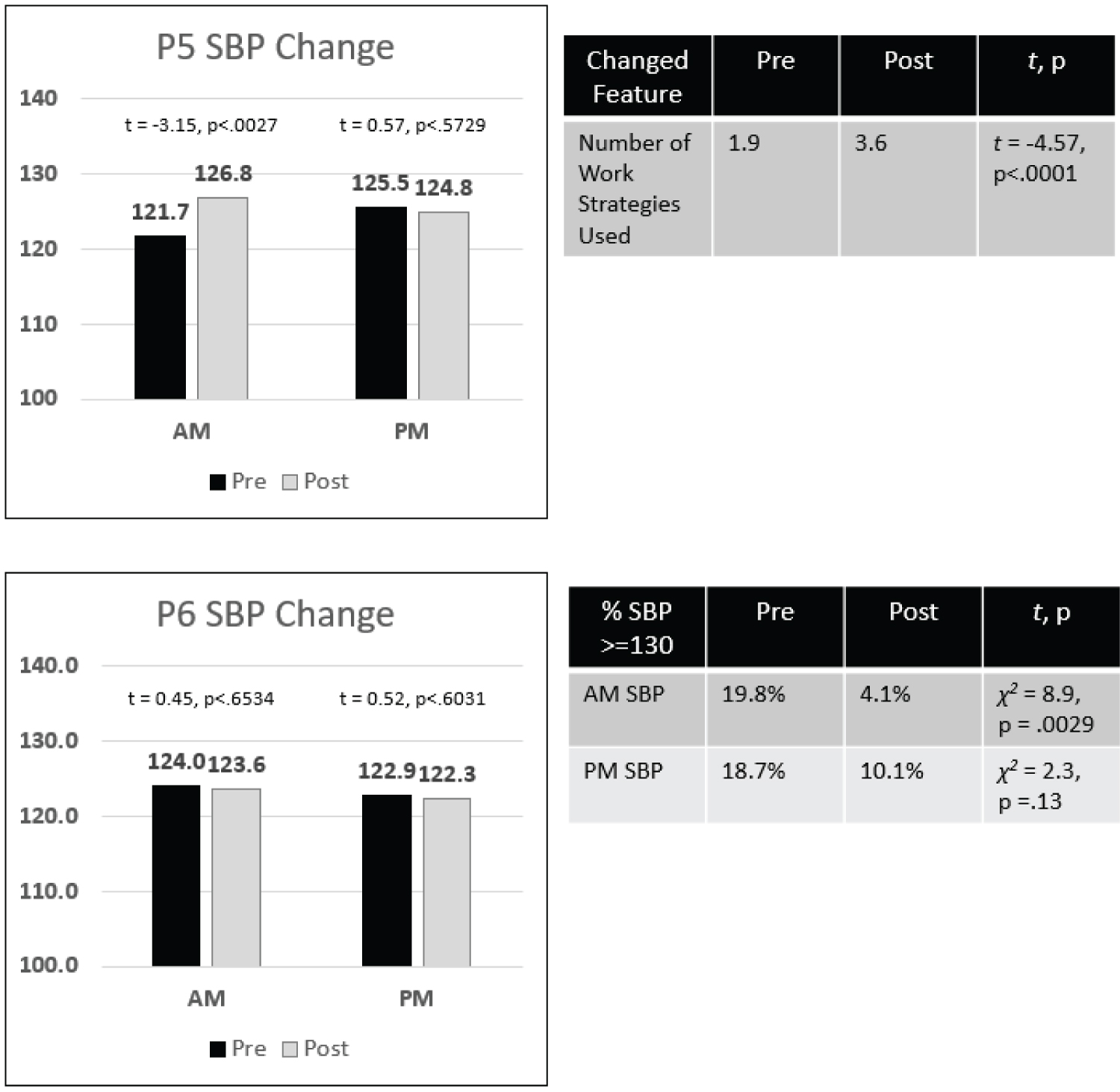 Figure 3: P5 and P6: Increase or No Change in SBP. View Figure 3
Figure 3: P5 and P6: Increase or No Change in SBP. View Figure 3
P6's BP reduction goal was more circumscribed than those of patients 1 to 5. P6's phase 1 SBP averages were both at the lower end of our target 120 to 129 mm Hg SBP range: i.e., AM SBP = 124 and PM SBP = 123.6. The phase 2 SBP reduction target for P6 was instead to reduce the number of SBP "spike" episodes: i.e., SBPs above 129 mm Hg. The results of our attempt to prune these spikes and reduce their number are depicted in P6's right-side table. The AM peak reduction from 19.8% of SBPs in phase 1 down to only 4.1% in phase 2 was statistically significant (χ2 = 8.9, p = 0.0029). The PM reduction from 18.7% to 10.1% was not statistically significant.
Summary: P1 to P6 SBP reduction: The preceding figures reveal a statistically significant average SBP reduction (4 patients), or SBP peak episodes reduction (1 patient) in 5/6 (83%) patients. These reductions occurred in 9/11 (81%) patients in AM and PM phase 1-phase 2 comparisons (P3's AM reduction was chiefly medication mediated and not included in the % calculation). The average reductions were to the 120-129 mm Hg range in 3/4 patients, and below 120 mm Hg in only 1/4 patients. The median average AM reduction was 6 points, and the median average PM reduction was 3 points. P6's SBP peak episode reductions were from 84% to 16% (significant) in the AM and 64% to 36% in the PM (not significant).
The average AM and PM phase 1 and phase 2 DBP values for all seven patients were below the recommended cutoff of 80 mm Hg. The changes in DBP in the AM and PM mirrored those of SBP for 6/7 patients. P6, however, had a different pattern. P6, who had no significant SBP changes, showed a significant PM decrease in average DBP (64.5 to 62.4 mm Hg, t = 3.11, p = 0.002).
P7's SBP was in the normal range and stable from phase 1 to phase 2. Despite this BP normalcy, P7 exhibited a symptom that can be BP associated with lower range BP. P7 complained that, at times, they did not feel "with-it". This complaint meant that they could no longer engage in work or social activities because they felt at a "distance" from their information environment. Such feelings occur, in our experience, in the prodrome of syncope. Apropos, P7 had reported syncope with falling as recently as two years before the study's onset, but not since. We tested two very different hypotheses that might explain a relationship between feeling less with-it and SBP.
The first hypothesis is cardiac event-related: viz., that a cardiac pre-syncopal state occurs during P7's lower SBP levels, but this state does not progress to syncope. The testable hypothesis is that P7 will report feeling more not-with-it when SBP is in the lower range, which is a positive correlation. During phase 1, P7's SBP range was lower in the PM than AM-average 107.3 (91-123) vs. 112.8 (98-127), respectively-implying that feeling less with-it would occur more often later in the day.
The second hypothesis is work-stress related. That is, feeling less with-it will be inversely correlated with higher SBP levels at the end of the day, secondary to the accumulated work stress over the day.
We tested these contrasting hypotheses over a period that encompassed the Christmas Holiday season during which P7 managed the family business (11-17 to 01-06). Consistent with both hypotheses, Table 2 reveals no statistically significant correlations in the AM. Table 2, however, shows several statistically significant correlations in the PM table. The pattern of these correlations coincides with the stress hypothesis. First, less with-it reports and SBP levels are inversely correlated: -0.49. Second, both measures show similar correlations with the number of PM cognitive issues: More cognitive issues are associated with higher SBP levels (+ 0.35, p < 0.05), and with lower with-it ratings (-0.61). In addition, a more negative affect (irritability) is correlated with higher SBP levels (-0.43) and with lower with-it reports (+0.66).
Table 2: Data for Differential Diagnosis: Relationship of SBP and Being "With-it". View Table 2
We have found that day-to-day e-diary-based coaching can be a useful adjunct to physician visit-to-visit management of elderly stroke outpatients in post-acute care. The adjunct utility was demonstrated with three major findings: 1) Earlier detection of anomalous cardiac events that require prompt medical attention, 2) Effective reduction of SBP, and 3) Providing empirical data to resolve a differential diagnosis involving SBP. Following the discussion of these findings, we conclude with a consideration of how patient engagement-e.g., patient adherence to, and diligence in, making reports, as well as interest in outcomes-was addressed in our study as well as earlier studies.
The detection of anomalous vascular events was demonstrated for three patients in phase 1 of our trial. The events detected were SBP spikes in three patients and one alarming HR elevation in one of the three patients. All events were first noted in the patient's e-diary data and then promptly brought to the attention of a physician. In addition, anomalous vascular events did not occur in any patient during phase 2 of our study. This absence of anomalous vascular events in phase 2 is likely attributable to the deterrence achieved through the coaching and monitoring of better patient health practices.
We set three different SBP reduction goals of increasing challenge: 1) A statistically significant reduction, 2) A reduction to the range 120 to 129, and 3) A reduction below 120. Four of six patients showed statistically significant SBP reductions of their AM or PM SBP averages from phase 1 to phase 2. The median average reduction was 7.6 points with a range of 2.7 to 8.6 points. Of these four patients, 2/4 achieved reductions to the 120 to 129 range, and 1/4 reached our ultimate goal of below 120. These reductions were associated with multiple statistically significant health practice improvements. One of the 6 patients had a more circumscribed SBP reduction goal: to reduce the number of spiked SBP episodes (i.e., SBP > 129). This patient showed a statistically significant reduction in the percent of AM episodes from phase 1 to phase 2: 19.8% to 4.1% and demonstrated a similar reduction of PM episodes: 18.7% to 10.1%, that barely missed statistical significance.
Our third success was to demonstrate that our e- diary adjunct methodology could also be used to compile empirical data to resolve a differential diagnosis involving SBP. The interpretation of P7's episodic alterations in consciousness-feeling not-with-it-was baffling until the e-diary data was analyzed. The e-diary data clearly showed that not-with-it episodes were associated with elevated SBP, and not with lowered SBP, at the end of the day.
Our study expanded upon the methodologies used in previous studies of SBP self-management. We attempted to increase our study's success by boosting patient engagement as defined above and as recommended by [17]. In their systematic review of smartphone apps and cardiovascular risk factor outcomes, Spaulding, et al. [17] suggested that an important ingredient in the successful use of smartphone apps in treatment is patient engagement. They concluded that the challenge was operationalizing and stimulating engagement. We agree and believe that our three expanded design features enhanced patient engagement and thereby boosted patient outcomes. Our e-diary system featured 1) Patient-customized data collection up to three times per day; 2) Biopsychological factor monitoring (i.e., monitoring of activities, stresses, and emotions); and 3) Customized patient consulting based upon the results of the biopsychological factor monitoring.
In particular, we enhanced engagement with a greater frequency of e-diary use (i.e., uses/day for a duration of weeks). The contact frequency we required, and achieved, was higher than that of other studies of e-communication adjunct use. Our patients made at least 2 recordings/day for a median of 24 weeks with a range between 18 and 25 weeks [8] gave patients BP monitors to use at home that could transmit BP back to the study; the patients measured BP 3-7/week for 9 months at the same time each day. Bengtsson, et al. [9] developed an interactive mobile phone support system to improve BP control. They reported the effect of the daily use of a mobile-phone-based self-management support system for hypertension. Patients used the system to self-report once daily for 8 weeks. Moore, et al. [10] evaluated an education and technology-supported hypertension management system that was used by patients for 12 weeks.
In addition, we enhanced engagement by tracking patient well-being with a broader range of health status probes. The patients in our study made more status reports in each e-diary recording than did patients in the studies cited. Unlike these studies, we added the collection of biopsychological status reports to our Bluetooth recording of BP and HR. This addition enabled us to individualize our coaching adjunct by correlating biopsychological factors with BP in each patient. Significant correlations identified the more influential biopsychological factors on BP in each patient. Patients were often not aware of the impact of these factors as influences on their SBP. They appreciated learning about the relationships. Engagement was maintained by offering an "information connection" to the study.
Finally, we enhanced engagement with a patient benefit. It is axiomatic that task engagement is enhanced by adding an opportunity for a reward. Strategic use of patient feedback was a design feature of our study. We showed patients the relationship between their health practices and their SBP. This feedback demonstrated how the adoption of healthier practices leads to a reduction in BP. Feedback in other studies was more limited and less patient-centered. Ciemins, et al. [8] asked about feelings of well-being, suggested lifestyle changes, and notified providers about issues in adherence and out-of-range values. They did not track well-being per se or lifestyle changes, however, so the participants did not get consistent feedback about those aspects of life. The Bengtsson, et al. [9] protocol also did not capture activity, stress, or co-morbidity information about their participants over time. Their education material instructed about the interplay of life and SBP, but many of the motivational messages were not specific to individual biopsychological factors. The graphical feedback provided was just about SBP. Moore, et al. [10] also taught about lifestyle changes, but the charts did not contain and hence demonstrate the impact of biopsychological factors on SBP.
In summary, the incorporation of these three engagement features into our e-diary study enabled us to formulate individualized monitoring and coaching adjuncts to improve health practices and reduce BP. This individualization also promoted patient engagement which enhanced management success. This individualized adjunct approach differs from the more common practice of using a standard, common adjunct [18].
Our e-diary adjunctive use with elderly stroke patients can be easily expanded to incorporate other forms of ambulatory physiological recording - e.g., recording cardiac rhythm - via Bluetooth connectivity. Our adjunctive e-diary use can also be extended to elderly patients with other chronic illnesses: e.g., cardiac disease, orthopedic conditions, and respiratory ailments. There have been a few studies that imply this broader application, although the examples do not include a test of the impact of use on care.
An extension to patients with cardiac illness is an obvious one, given that adjunctive use would essentially be a replication of methods described here for stroke patients. Jean, et al. [19] tested the feasibility and validity of a methodology like our own (i.e., Ecological Momentary Assessment) with acute coronary syndrome patients and reported good adherence but did not investigate its impact on self-management.
An extension to patients with orthopedic conditions has precedents with a rehabilitation focus. Patients who have undergone knee replacements must undertake daily exercise regimens to optimize the success of the surgery. E-diary and telephone-based exercise instruction and exercise recording have proved to be effective in increasing exercise adherence [20].
Symptoms of chronic obstructive pulmonary disease (COPD) have also been monitored with e-diaries [21]. Ratings of the severity of shortness of breath were associated with a reduction of activities and feelings of well-being after treatment with QVA149, but they did not provide suggestions of clinical applications for non-pharmaceutical treatment.
E-diary use for symptom management as an adjunct to visit-to-visit care of elderly patients with chronic illnesses takes on an added benefit in the COVID pandemic era. E-diary adjuncts can be combined with virtual visits to curtail exposure to COVID at a clinic visit or on route to a clinic. The combination of the two e-technologies is a great boon to elderly patients with chronic illnesses who are the most vulnerable to COVID morbidity and mortality [22].
Despite our successful interventions with 5 patients, we failed to achieve SBP reductions in a sixth patient, P5. This patient had a significant life-changing event in their phase 2 period that elevated their SBP, thereby thwarting our attempts to reduce their SBP.
P5 did not show a SBP reduction in both the AM or PM. Indeed, P5 showed a statistically significant AM SBP increase in phase 2. P5 received a major promotion during our study. New work associated with this change elevated the cognitive demand of P5's work (they had to use more compensatory work strategies during phase 2). These events likely generated their SBP elevation as well.
The reason for our failure with P5 exposes a limitation due to insufficient time of follow-up. Our study was funded for a one-year feasibility investigation by the National Institute of Aging. In addition to the interruption by the COVID pandemic, there was not enough time to restart P5's case study with a new phase 1 baseline that would accommodate the dramatic life event change and SBP elevation.
For this reason, we recommend taking more detailed patient histories to anticipate life-altering changes that may elevate BP. We also recommend a provision to restart a coaching protocol with a new phase 1 baseline when a major phase 2 lifestyle challenge occurs with demonstrable BP elevations.
In summary, we find that a combination of two methodologies to be most impactful for post stroke blood pressure management in aging patients. These are 1) longitudinal digital monitoring of 2) iterative interventions.
This work was supported by a small business innovation research grant from the NIH Institute of Aging awarded to SymTrend, Inc. (1R43 AG060851-01). Dr. Levine is a majority stockholder and an officer of SymTrend, Inc. and was the principal investigator of the grant. Dr. Goldstein has a small share of equity in SymTrend. The authors thank all study participants for persisting with electronic monitoring for approximately six months.
National Institute of Aging 1R43 AG060851-01.