Angiolipoma is a histological variant of the more common lipoma that may occur superficially throughout the body. After review of recent literature, different cases of angiolipomas were reported within various areas, more so in the upper extremity and truncal regions [1,2]. Our clinical case demonstrates an extremely rare presentation of a non-infiltrating angiolipoma lesion growing within a hamstrings autograft after anterior cruciate ligament (ACL) reconstruction. There have been a few prior reports of lower extremity intraarticular angiolipomas inside the knee, but to the best of our knowledge, none have been identified specifically within an ACL hamstrings autograft. This clinical case is of particular interest to orthopaedic surgeons and sports medicine specialists as a potential differential diagnosis for knee joint pain and disability without an obvious source.
Angiolipoma is an uncommon, benign tumor involving mainly subcutaneous tissues of mainly younger patients in their twenties or thirties [1,2]. This histological variant of the more commonly encountered lipoma makes up 5-17% of all lipomas [1-3]. This soft tissue lesion was first described in 1912 then was established as its own separate pathological diagnosis in 1960 [4,5]. The nomenclature angiolipoma depicts two named histologic constituents, i.e. it is a neoplasm consisting of scattered blood vessels within an encapsulated fatty tissue mass that develops beneath the skin [1-3]. The exact cause of angiolipomas is largely unknown. The etiology of angiolipoma is a matter of debate, though post-pubertal hormonal influence and repetitive microtrauma have been theorized to play a role in its origin [1,2]. These subcutaneous masses can occur anywhere on the body but are most often found on the neck, trunk, and extremities, with up to two-thirds occurring on the forearm. Intraarticular knee lesions are very rare, only a few clinical cases have been cited in the English literature in the last decade. Angiolipomas within joints have been known to cause pain, swelling, hemarthrosis, and knee dysfunction [1,3]. These reports of angiolipomas which occur within the knee joints include: One extending outside of the capsule [1], the second within the posterior cruciate ligament [3], and the third localized in the suprapatellar pouch [6]. However, to our knowledge, this is the first reported case of angiolipoma within an ACL hamstrings autograft. The purpose of this paper is to discuss our unique clinical case along with review of the literature about angiolipoma.
The patient is a 32-year-old healthy prior military, active Caucasian male: height 177.8 cm; weight 83.91 kg; body mass index (BMI) 26.54 kg/cm-2 with only a history of light tobacco use and occasional alcohol consumption, who underwent right knee ACL reconstruction with a hamstrings autograft in 2014 at another surgical facility. He did well for almost 3 years, but then developed recurrent right knee pain and was referred to our Orthopaedic Sports clinic in September of 2017. He complained of right knee pain with deep squatting, particularly while he was at work as an automotive mechanic. He denied any repeat injury or other related symptoms. His knee was stable to Lachman test, also varus and valgus stress. The McMurray's test was found to be negative as well, thus no meniscal or ligamentous pathology was suspected clinically. Subsequently, magnetic resonance imaging (MRI) demonstrated findings suggestive of posterior horn medial meniscal tear, appropriate tibial and femoral tunnel placements, intact ACL graft, and an intercondylar cystic lesion, which was read by the radiologist as a "loose body" (Figure 1, Figure 2 and Figure 3).
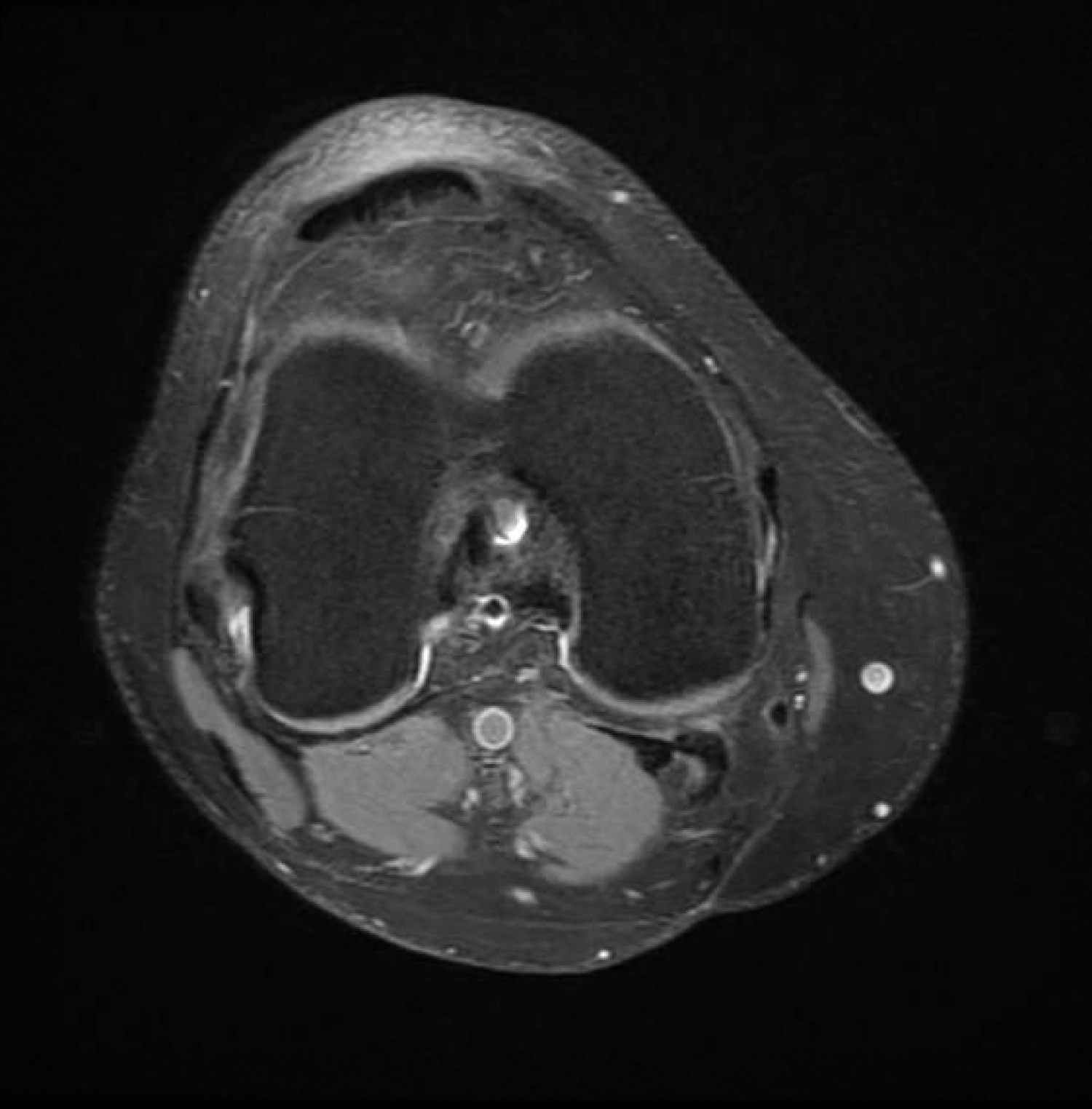 Figure 1: In this axial cut of a T2 weighted MRI, there is a notable intercondylar cystic fluid collection and fibers of the ACL graft appear heterogenous but intact.
View Figure 1
Figure 1: In this axial cut of a T2 weighted MRI, there is a notable intercondylar cystic fluid collection and fibers of the ACL graft appear heterogenous but intact.
View Figure 1
 Figure 2: The intercondylar cystic lesion is again demonstrated on the T2 weighted coronal MRI cut, appearing within the fibers of the ACL graft. The ACL graft fibers appear intact.
View Figure 2
Figure 2: The intercondylar cystic lesion is again demonstrated on the T2 weighted coronal MRI cut, appearing within the fibers of the ACL graft. The ACL graft fibers appear intact.
View Figure 2
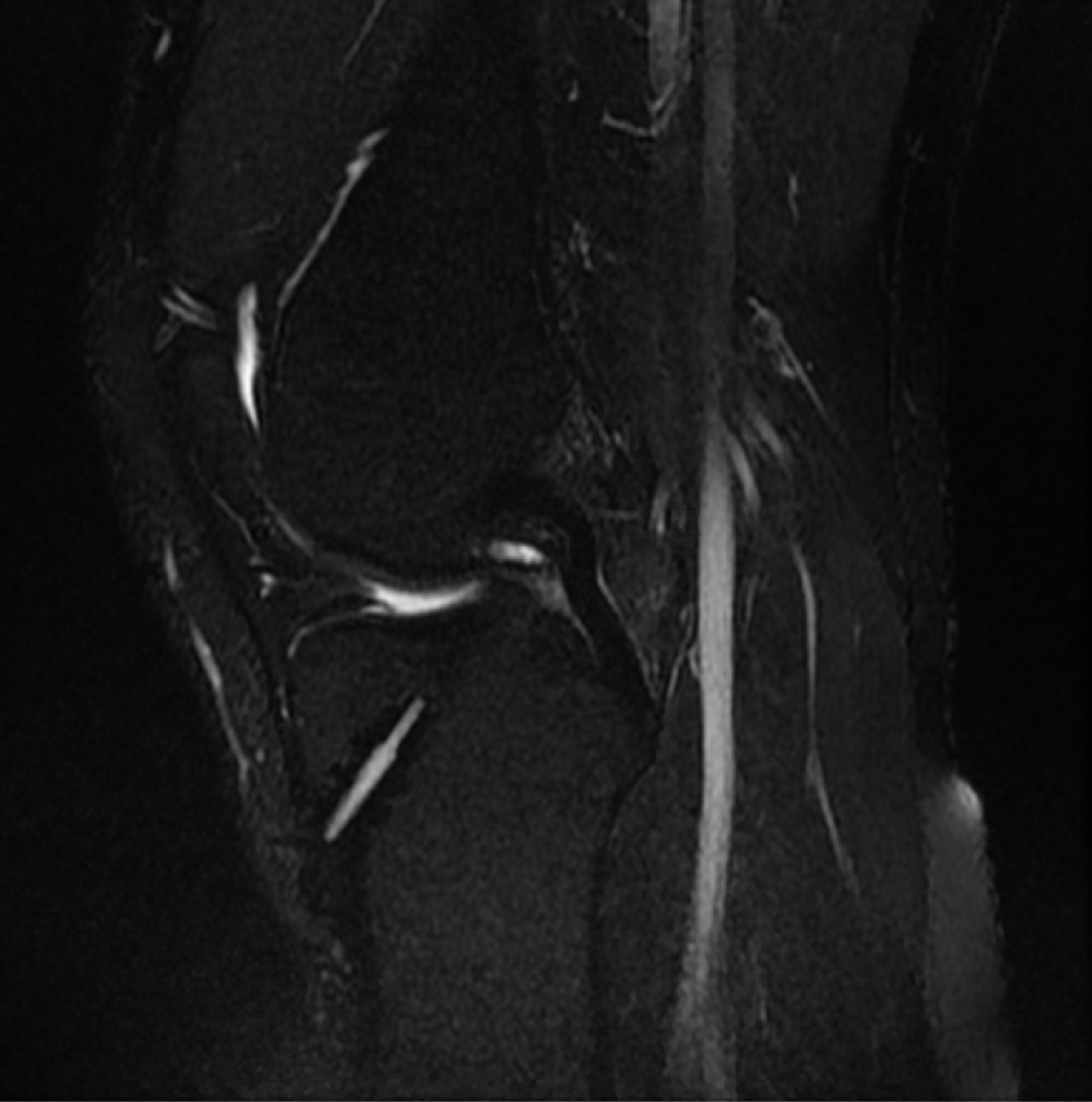 Figure 3: The T2 weighted MRI sagittal cut demonstrates previous tibial tunnel placement with cystic fluid collection demonstrated in the notch.
View Figure 3
Figure 3: The T2 weighted MRI sagittal cut demonstrates previous tibial tunnel placement with cystic fluid collection demonstrated in the notch.
View Figure 3
He was given a prescription for physical therapy (PT), instructed to weight bear as tolerated while avoiding exacerbating maneuvers. He returned to clinic one month later with continued activity related right knee pain despite completing his PT regimen. He had developed more swelling, popping, and catching of his knee, along with frequent buckling episodes. He denied constitutional and other systemic symptoms. He began having pain at the extremes of knee range of motion (ROM), and painful McMurray's maneuver now consistent with meniscal pathology. The knee remained stable to all ligamentous stressing. Since conservative measures were not helpful, he desired to proceed with repeat surgical procedure for his symptomatic right knee. He continued to perform PT and home rehab exercises preoperatively.
In January of 2018, he underwent right knee arthroscopy, about 4 months after his initial presentation. Intraoperatively, his knee joint was found to have diffuse hypertrophic synovitis, chondromalacia, hypertrophic medial plica, and a 5 mm by 7.5 mm fatty soft tissue mass within the structure of the ACL graft (Figure 4, Figure 5 and Figure 6). Chondroplasty and plica excision were performed, as well as an excisional biopsy of the fatty ACL graft lesion. The intraarticular knee mass was completely excised at the time of arthroscopy. After mass excision, the remaining ACL graft fibers were found to be stable upon probing. Postoperatively, he was instructed to gradually increase weight bearing as tolerated over the following weeks and restart formal physical therapy exercises. He went on to recover uneventfully and returned to his usual level of physical activity symptom free after a few months post-surgery.
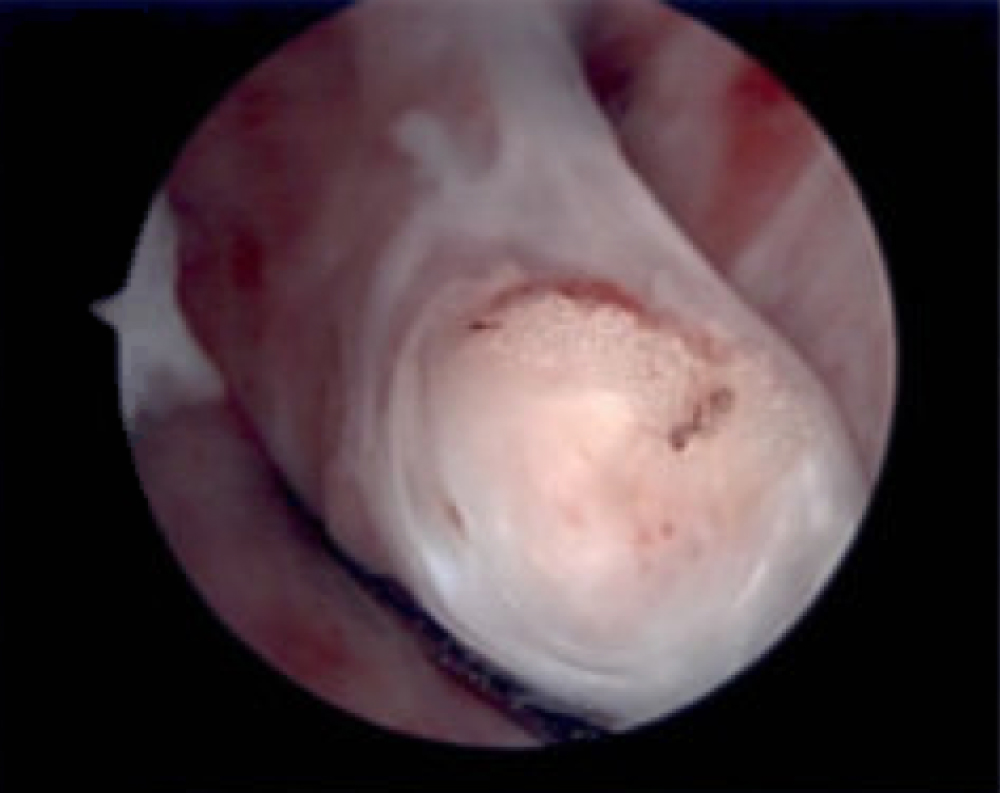 Figure 4: In this arthroscopic view of the intercondylar notch, there is a fatty lesion in the midsubstance of the ACL graft fibers.
View Figure 4
Figure 4: In this arthroscopic view of the intercondylar notch, there is a fatty lesion in the midsubstance of the ACL graft fibers.
View Figure 4
 Figure 5: The lesion was probed and noted to be a soft, largely fatty tissue within the ACL graft. The ACL graft fibers were noted to be stable with probing.
View Figure 5
Figure 5: The lesion was probed and noted to be a soft, largely fatty tissue within the ACL graft. The ACL graft fibers were noted to be stable with probing.
View Figure 5
 Figure 6: The ACL graft lesion was excised and again the graft fibers were noted to be stable with probing. The soft tissue mass was sent as an excisional biopsy for histological preparation.
View Figure 6
Figure 6: The ACL graft lesion was excised and again the graft fibers were noted to be stable with probing. The soft tissue mass was sent as an excisional biopsy for histological preparation.
View Figure 6
This clinical case is presented as a unique manifestation of an angiolipoma within the knee joint. The patient originally underwent hamstrings allograft ACL reconstruction without complications. Due to recurrence of knee pain and mechanical symptoms that did not resolve with conservative measures, a cystic lesion was identified upon MR imaging. Differentials included synovial lipoma, small locus of pigmented villonodular synovitis, myxoma, hemangioma, and more concerning, but less likely, various soft tissue sarcomas. These differential diagnoses were much lower on our list, however, this unusual manifestation of a cystic lesion within a previously operated knee joint led us to broaden our list of possible pathologic tumors. Histopathology from arthroscopic excision of the intraarticular mass demonstrated two types of tissue present consistent with angiolipoma.
In Figure 7, Figure 8 and Figure 9, small blood vessels were present within the soft tissue mass, identified by their smooth muscle walls. The arteries, arterioles, and disorganized capillaries were interspersed through a field of mature adipose cells. These images, taken from histological slides of the intraoperative specimen, were conclusive for angiolipoma of the ACL hamstrings autograft.
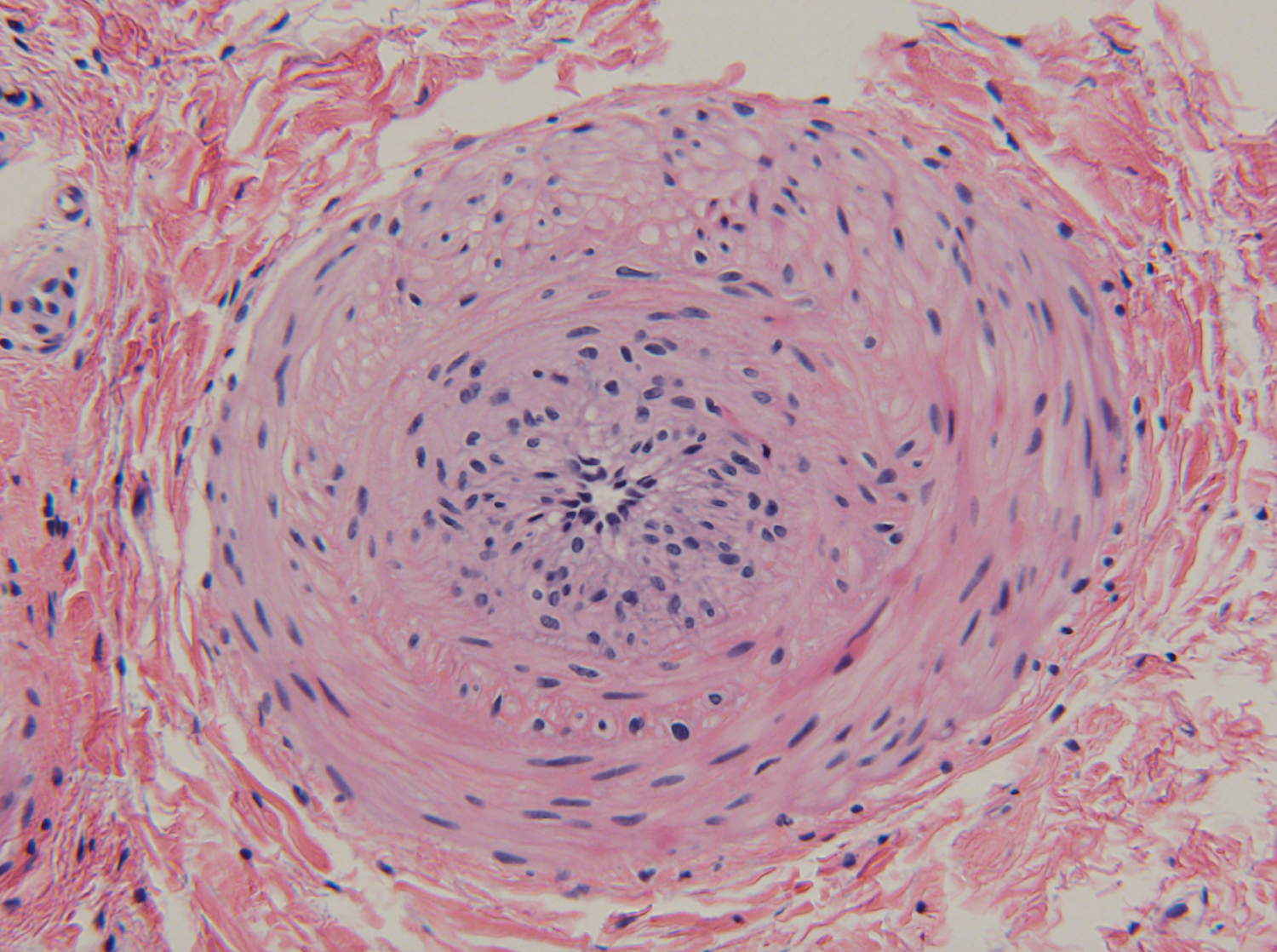 Figure 7: Within the specimen, there were small arteries and arterioles noted. This particular vessel has a thin layer of surrounding smooth muscle and was one of the larger blood vessels within the biopsy sample.
View Figure 7
Figure 7: Within the specimen, there were small arteries and arterioles noted. This particular vessel has a thin layer of surrounding smooth muscle and was one of the larger blood vessels within the biopsy sample.
View Figure 7
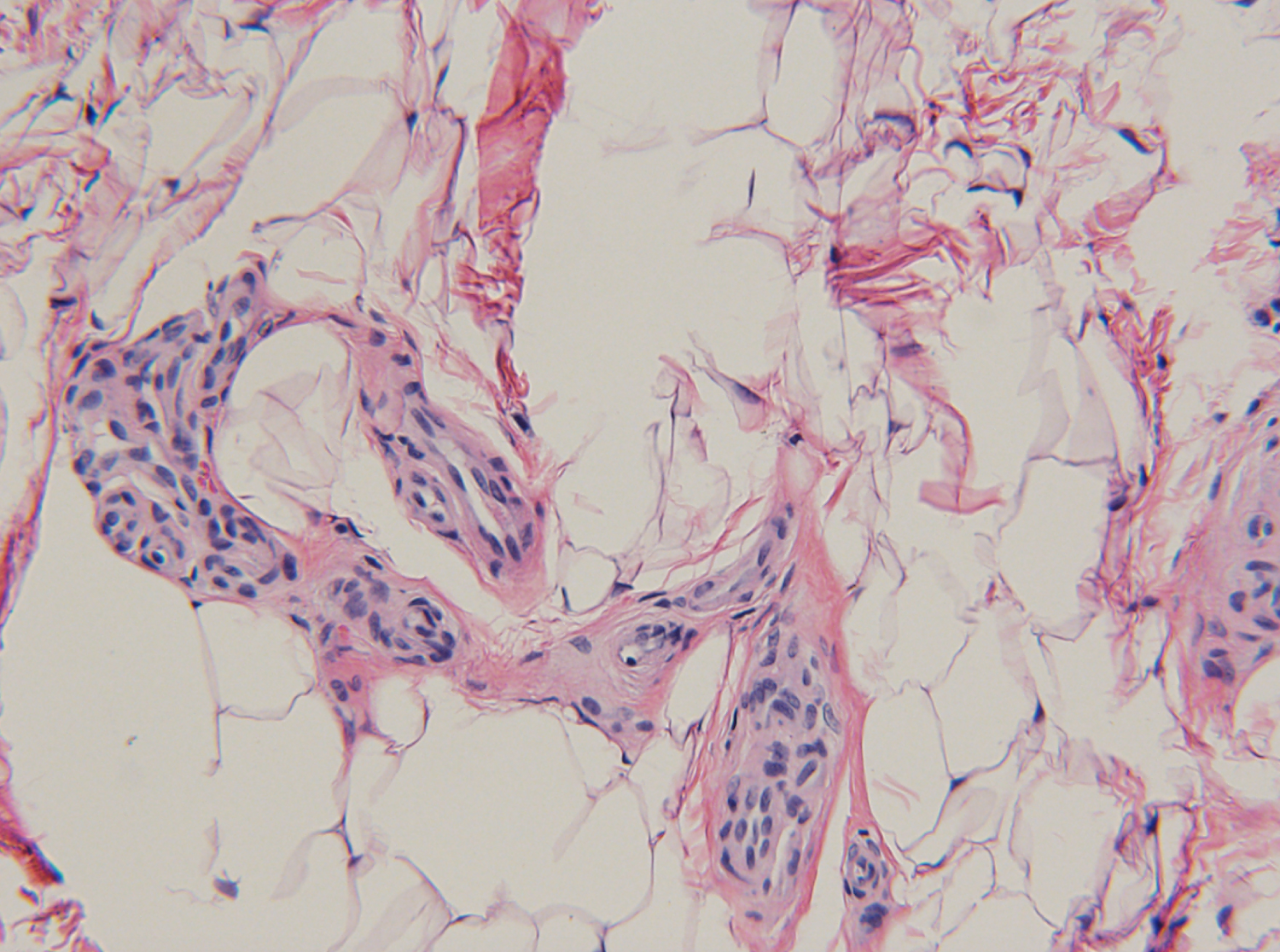 Figure 8: Small arterioles were observed within an adipose stroma indicative of angiolipoma. This disorganized hypervascularity within mature adipose cells was noted on multiple fields.
View Figure 8
Figure 8: Small arterioles were observed within an adipose stroma indicative of angiolipoma. This disorganized hypervascularity within mature adipose cells was noted on multiple fields.
View Figure 8
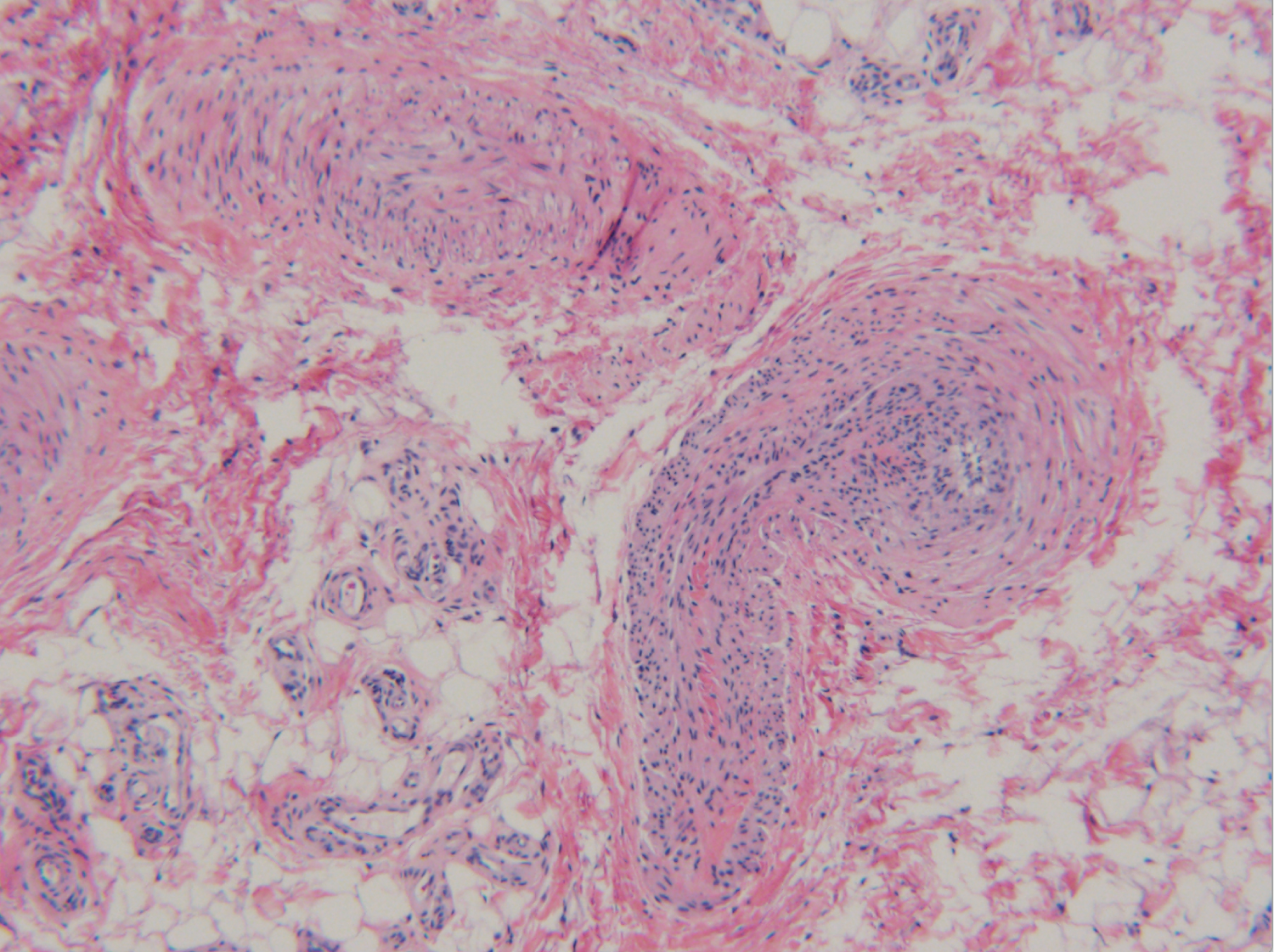 Figure 9: Small disorganized arteries and arterioles are interspersed within a field of adipose tissue, reinforcing the diagnosis of angiolipoma rather than hemangioma.
View Figure 9
Figure 9: Small disorganized arteries and arterioles are interspersed within a field of adipose tissue, reinforcing the diagnosis of angiolipoma rather than hemangioma.
View Figure 9
Non infiltrating angiolipomas are soft, encapsulated nodular lesions consisting of mature adipose cells (yellow-tinged) and multiple vascular channels (red-tinged) [2,3,6]. No sex predilection exists though case reports have identified more in males. They tend to occur more commonly around the 2nd to 4th decades of life [6]. These superficial nodules are located in the subcutaneous layer and involve the neck, back, thighs, and arms [1-3]. Among the various types of lipomas, typically angiolipomas tend to be more painful on palpation [1,3], not dissimilar to our patient's complaint though his knee symptoms were more nonspecific. Histologically, the blood vessels often contain fibrin microthrombi [1-3,6], thought to be an artifact of preservation. Often, the tiny aggregates of capillaries are complex but poorly formed and not well organized [3]. The presence of adipose tissue distinguishes this lesion from a hemangioma, which is more hypervascular and lacks adipose cells [3]. Angiolipomas can have a diameter from 1 cm to about 15 cm [1,3,6]. Angiolipomas were previously classified as non-infiltrating or infiltrating-an even more rare entity [2]. Non-infiltrating angiolipomas do not penetrate surrounding soft tissues. The more invasive form, infiltrating angiolipomas are now identified as intramuscular hemangiomas [2,3].
On MR imaging, angiolipomas typically appear fairly well demarcated, much like our patient's intra-articular knee mass, though the radiologist's read was potential "loose body" in the intercondylar notch [6]. These soft tissue lesions also tend to have high signal intensity on both T1 and T2 weighted images due to their fat and blood content [3,6] (Figure 1, Figure 2 and Figure 3).
Our young male patient in his early thirties presenting with an intraarticular angiolipoma involving the previously reconstructed ACL hamstrings autograft fits the age profile but not the usual locale for this type of benign soft tissue tumor. His mass was within the knee joint so diagnosis was not confirmed until after the pathologist viewed the surgical specimen. He was successfully treated with arthroscopic excision alone, and has since returned to his daily activity without restrictions. In this case, diagnostic arthroscopy with excisional biopsy for histologic identification also proved to be therapeutic. Local recurrence of this lesion is thought to be nonexistent, although metaplasia into osteochondral tissue has been known to occur, along with mucoid degeneration [6]. However, no local invasion, distant metastases, nor malignant transformation has been reported [2,6]. To our knowledge, this particular manifestation of knee angiolipoma or other soft tissue masses within ACL autografts has not been previously documented. As such, we feel that this case provides new insight when presented with a diagnostic dilemma for a traumatic knee pain in a patient who has previously undergone ACL reconstruction, without an obvious source or cause to explain recurrence of joint symptoms.
Informed consent was obtained from the patient for publication of this case report and any accompanying images.
The authors declare that they have no competing interests.
AV and KK did literature search, wrote preliminary abstract and background sections; AP reviewed literature, wrote, and revised the paper; MZ reviewed, researched current literature and edited the write-up. All authors approved the final transcript.
We appreciate the help of Kimberly Burbank, MD candidate, for her assistance with collecting patient information. We also thank Dr. Ruc Tran for providing pathology slides.