Background: Lateral epicondylitis (LE) is a common cause of elbow pain. Besides conservative treatments, ozone therapy is getting attention due to its safety and effectiveness. This study aimed to assess the effectiveness of ozone therapy in lowering pain and tenderness and improving joint function.
Methods: Patients clinically diagnosed with LE were included in our study. Baseline assessments including age, gender, involved elbow, tenderness, pain, and function scores were done. All the patients underwent up to ten sessions of ozone injection in the pain site. Each injection was between six to ten ml of 30 μg/ml ozone gas into the lateral epicondyle. After the treatment regimen, tenderness, pain, and function scores were assessed.
Results: Of the 28 patients with LE, 16 and 12 were female and male, respectively. More than 80% had high physical activities with their involved elbow. Comparing the pain, tenderness, and function before and after the treatment, all parameters were statistically improved (P < 0.05). These results were consistent in both men and women subgroups.
Conclusion: Ozone therapy is a safe and effective procedure in patients with LE to reduce pain and tenderness, in addition to improving performance. However, large clinical trials are warranted to compare ozone injection with routinely used treatments by clinicians.
The most common cause of pain in the lateral elbow is lateral epicondylitis (LE), also known as tennis elbow. Overuse of the wrist in gripping and extension is the accepted etiology for LE [1]. This condition is not only a causes of pain, but it also plays a key role to loss of function at the elbow joint. As the result, reduction of normal activity and absence from work is possible. Conservative treatments such as non-steroidal anti-inflammatory drugs (NSAIDs), ice, rest, and reducing motion are required for settling the pain and inflammation [2]. A systematic review conducted by Bateman, et al. showed that surgical interventions in LE patients are not more effective than nonsurgical treatments [3].
Local corticosteroid injection is a safe way to manage pain in LE. Smidt, et al. found a significant short-term reduction in pain and grip strength after corticosteroid injection compared to placebo, local anesthetics, or conservative treatments [4], however, long-term changes were not significant. In addition, corticosteroid injection was significantly better than placebo and naproxen in a clinical trial [5]. On the other hand, a study compared corticosteroid and ozone injection in a clinical trial and found better outcomes following ozone injection [6]. The safety of ozone therapy in LE is not established yet in the literature, however, there is no strong evidence of harm in this treatment method [7]. In this communication, we aimed to compare the severity of pain, tenderness, and involved elbow before and after the ozone injection treatment regimen in LE.
This cross-sectional study was conducted between April through September 2017 in patients referred to the Physical Medicine and Rehabilitation Clinic at Firouzgar hospital, Tehran, Iran who were diagnosed with lateral epicondylitis. Patients with persistent pain and local tenderness in the lateral epicondyle of the elbow for less than four weeks, pain in forearm supination when the elbow is flexed, and pain in dorsiflexion of the hand were included. We excluded patients with a history of trauma to the elbow, having symptoms for more than four weeks, having interventional pain treatment such as corticosteroid injection, history of connective tissue disease or diffuse pain syndrome (such as fibromyalgia, or chronic pain syndrome), inflammatory arthropathy, previous treatments, the impossibility of reducing heavy work with the hand, radiculopathy, complete rupture of Extensor Carpi Radialis Brevis tendon, elbow effusion, anti-coagulant consumption, and contra-indications for injection.
A checklist including information about age, gender, involved elbow (left, right, or both), high physical activity, pain intensity and joint dysfunction before a treatment based on the visual analog scale (VAS), and the intensity of tenderness (1 for mild, 2 for moderate, and 3 for severe) before the treatment based on the examination of the registered physician.
The ozone-oxygen mixture was produced in real time by a medical ozone generator converting oxygen gas (O2) into ozone (O3). High-pressure pure medical oxygen cylinders were used to transform O2 in O3, and a Millipore bacteriological filter was placed between the 10 ml syringe and the generator. Depending on the patient's limb size, between six to ten ml of ozone gas (30 μg/ml) was injected into the external epicondyle in each session. No corticosteroids or local anaesthetic were injected into the external epicondyle during the procedure. The mean time to complete the procedure was approximately 20 min. After injection, patients were kept for 30 min in clinic for observation and discharged if no red flags included either systemic symptoms (hypotension, tachycardia) or local symptoms (skin redness) were noticed. Return to work was permitted after discharge. Prophylactic antibiotics, opioid medications and antihistamine were not prescribed to patients. They were advised to take Acetaminophen if it is needed.
The interval between sessions was between three to five days. We repeated the procedure up to a maximum of 10 sessions.
After receiving the treatment based on the number of sessions required, the follow-up program of the patients was carried out according to the routine of the clinic depends on the condition of the patients. Out of 28 patients, 23 of them were followed up after 12 weeks, 3 after 14 weeks, and 2 after 15 weeks from the last dose of ozone therapy. We were following the follow-up period of the disease, the continuation of the prepared checklist included pain intensity and joint dysfunction after treatment based on the VAS and the intensity of tenderness (1 for mild, 2 for moderate, and 3 for severe) after treatment based on the physician's examination was recorded.
All the data were interpreted using the Statistical Package for the Social Sciences (SPSS), version 26 (IBM Corp., Armonk, NY, USA). Categorical variables are presented as number/total cases (%) and continuous variables as mean ± standard deviation (SD). The significance of changes after treatment was evaluated using the paired t-test. In the subgroup analyses, we subdivided the data based on sex. A two-sided p-value of < 0.05 was considered significant.
Twenty-eight patients (16 female and 12 male) with an average age of 39.89 ± 10.20 who underwent ozone therapy were included in the study. Most of them had right-elbow epicondylitis (57.14%) and 85.71% reported high physical activity with the involved limb. Each patient underwent between 5 to 10 sessions (mean = 6.5) of ozone therapy based on the physician's decision. Table 1 summarizes the baseline characteristics of patients included in our study.
Table 1: Baseline characteristics. View Table 1
A significant decrease in the pain score was seen among patients (7.89 ± 0.33 vs. 5.07 ± 0.58; p-value < 0.001). In addition, the dysfunction score mentioned by patients significantly reduced after the therapy (8.39 ± 0.40 vs. 4.68 ± 0.68; p-value < 0.001). Figure 1 represents tenderness before and after the treatment. Before the treatment, 10.71%, 53.57%, and 35.71% had mild, moderate, and severe tenderness, respectively. In the post-treatment assessment, 57.14%, 39.29%, and 3.57% had mild, moderate, and severe tenderness, respectively. Finally, there was a significantly lower tenderness score in patients after the treatment (2.25 ± 0.65 vs. 1.46 ± 0.58; p-value < 0.001). All the pre- and post-treatment details are available in Table 2.
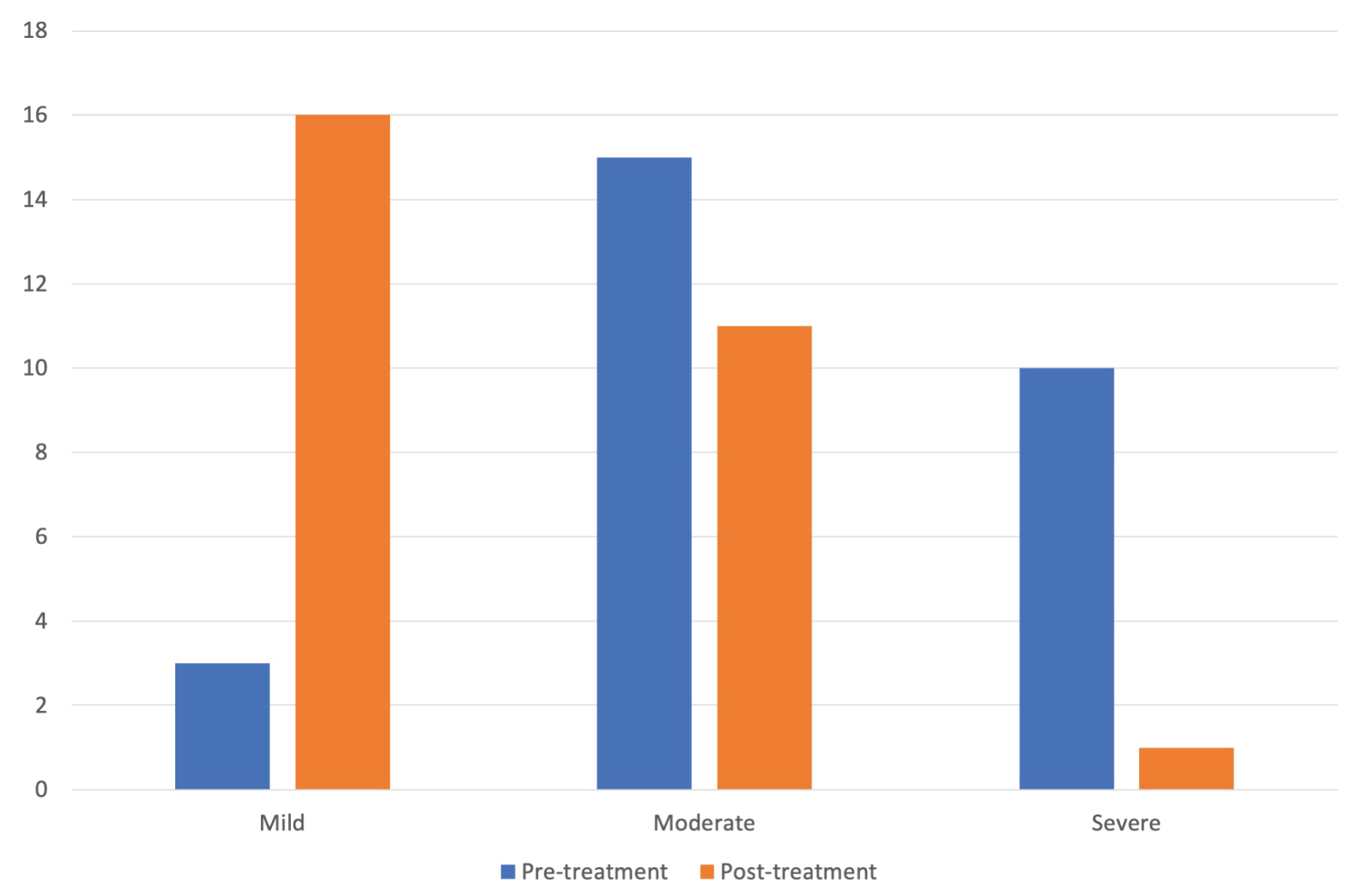 Figure 1: Tenderness before and after the treatment.
View Figure 1
Figure 1: Tenderness before and after the treatment.
View Figure 1
Table 2: Pre- and post-treatment pain, dysfunction, and tenderness scores. View Table 2
The subgroup table shows higher baseline scores for pain (7.92 ± 1.68 vs. 7.88 ± 1.89), dysfunction (9.25 ± 1.48 vs. 7.75 ± 2.32), and tenderness (2.50 ± 0.52 vs. 2.06 ± 0.68) in men compared to women. In both females and males, all the scores significantly reduced after the therapy (highest p-value = 0.010). Table 3 summarizes subgroup analysis results.
Table 3: Subgroup analysis. View Table 3
In this study, we found that injection of ozone gas reduces pain, and local tenderness, and improves functions in the LE. In addition, no remarkable adverse effects included local infection, necrosis or tendon rupture during or after injection of ozone were reported in patients.
The efficacy of ozone therapy as a conservative treatment in pain medicine, especially shoulder, knee, and spine is well-known [7]. Several mechanisms were suggested for the ameliorating effect of ozone on pain. The main mechanisms behind the ozone effects are anti-inflammation, analgesic, anti-edema, and oxidation of the algogenic receptors which activate the antinociceptive system [8]. In addition, oxygen and ozone gas help muscles to recover faster from activities and relax by improving the oxygenation of the tissue [9].
In our study, we used six to ten ml of ozone gas with the 30 μg/ml concentration every three to five days. There is no standardized dosage for the injection of ozone in the literature. However, in a review by Hidalgo-Tallon, et al., injection of between five to 15 ml of ozone with the concentration range of four to 30 μg/ml and three to ten sessions, one or two per week, was recommended [7]. Consequently, our procedure details for dosage were in the ranges mentioned in the review.
Despite our hard work to minimize biases, there were some limitations in our study. First, all the patients were selected from a single center. Second, there were no control or placebo group for validating our results. Finally, all the analyzed data were subjective, and due to the low sample size, they are not generalizable to all patients with LE.
Ozone therapy is an effective therapy besides conservative treatments in reducing pain, and tenderness, and also in improving performance and activity without the pain of the patient's involved upper limb. The results were similar in men and women. However, more studies are required to assess the effectiveness of ozone injection in LE and also for standardization of treatment protocols and determination of indications and side effects.