Obesity is characterized by an excessive body-fat and a chronic low-grade inflammatory state. Its population diagnosis is measured by body mass index (BMI), which classifies obesity as a BMI of ≥ 30 kg/m2. Raised BMI is a known risk factor for multiple chronic disorders, particularly diabetes and cardiovascular diseases. In recent decades, there has been an emergent scientific interest in more natural therapeutic approaches, including phytotherapy. In this context, green tea (GT) is a popular beverage made out of the leaves and buds parts of Camellia sinensis, which, due to its rich polyphenol source, presents various functional properties, including the role as antioxidant, anti-inflammatory and appetite inhibitor. Hence, GT and its constituents have been widely investigated as a potential target for the treatment of obesity and its related comorbidities.
To evaluate the effect of GT as a treatment for obesity based on anthropometric and biochemical parameters in both humans and experimental models.
A systematic review was performed on different platforms: MEDLINE (via PubMed), LILACS, COCHRANE, SCIELO and related articles, which included studies that used GT as treatment for obesity and its related comorbidities.
In experimental models, treatment with GT showed a tendency to reduce body weight and serum inflammatory biomarkers IL-6 and IL-1β. In humans, a reduction in BMI and waist circumference has been demonstrated, as well as an improvement in biomarkers such as TNF, CRP, serum insulin, HbA1c, HOMA-IR, in addition to lipid profile, especially TG.
The present review points out that there is a positive trend in important effects associated with the use of GT. However, its benefits in the context of obesity treatment are still scarce and unclear, requiring more research to better support these effects.
Green tea, Camellia sinensis, Epigallocatechin, Herbal medicine, Obesity
ATGL: Adipose Triglyceride Lipase; BP: Blood Pressure; BMI: Body-Mass Index; C: Catechin; CAT: Catalase: CRP: Reactive C Protein; CVD: Cardiovascular Disease; DGAT: Diacylglycerol Acyltransferase; EC: Epicatechin; ECG: Epicatechin Gallate; EGC: Epigallocatechin; EGCG: Epigallocatechin Gallate; FFA: Free Fatty Acids; GC: Gallocatechin; GCG: Gallocatechin Gallate; GLUT 4: Glucose transporter 4; GPXs: Glutathione Peroxidases; GSH: Glutatione; GT: Green Tea; HbA1c: Glycated Hemoglobin; HDL: High-Density Lipoprotein Cholesterol; HNE: Hydroxynonenal; HOMA-IR: Homeostatic Model Assessment Of Insulin Resistance; HSL: Hormone-Sensitive Lipase; IL: Interleukin; JNK: JunN-Terminal Kinase; LDL: Low-Density Lipoprotein Cholesterol; MCP1: Monocyte Chemostactic Protein 1; MDA: Malondialdehyde; METs: Metabolic Syndrome; MMP: Matrix Metalloproteinases; mRNA: Messenger RNA; NFkB: Nuclear factor kappa b; PICO: Population, Intervention, Comparators, Outcome; SNS: Sympathetic Nervous System; TC: Total Cholesterol; TDM2: Type 2 Diabetes Mellitus; TG: Triglycerides; TNF: Tumor Necrosis Factor; WAT: White Adipose Tissue; WHO: World Health Organization
Obesity is defined as an excess of adipose tissue. Screening measurement of obesity is commonly made with body-mass index (BMI; weight in kg/height in m2), which has a good correlation with body fat [1]. According to the World Health Organization (WHO), a BMI of 30 kg/m2 or higher is classified as obesity in adults [2].
Raised BMI is a risk factor for noncommunicable diseases such as diabetes, cardiovascular diseases, and musculoskeletal disorders, resulting in dramatic decrease of life quality and expectancy [3]. The global prevalence of obesity has increased substantially over the past 40 years, from 3% in 1975 to 11% in 2016 among men and from 6% to 15% among women over the same time period [4]. Meanwhile, linear time trend forecasts suggest that by the year of 2030, worldwide obese population will reached out to 51% [5].
It is consensual that the primary treatment intervention for obesity underlies in behavioral modification, particularly associated with calorie restriction intake and regular physical activity [6]. In recent years, however, complementary, and alternative treatments for obesity have emerged as a potential field of research. Drug-therapy commonly used to induce weight loss and minimize physiological changes caused by excessive body-fat usually has a high cost, potential side effects and low-efficacy. Alternative treatments include acupuncture, homeopathy, sleep therapy and medicinal plants and their active ingredients, which have existed since ancient times [7].
In the context of herbal medicine, Green tea (GT) is a type of tea made out of the leaves and buds of Camellia sinensis, a evergreen shrub usually trimmed to below two meters (six feet) when cultivated for its leaves [8]. C. sinensis originated from southeast Asia, and currently it is cultivated in more than 30 countries, including India, China, Sri Lanka, Kenya, Indonesia, Turkey, former Soviet Union, Japan, Iran, Bangladesh, Malawi, Vietnam, and Argentina [9].
The dried, cured leaves of C. sinensis have been used to prepare beverages for more than 4000 years. The method of curing determines the nature of the tea to be used for infusion. White tea, green tea, oolong and black tea are all harvested from this species but are processed differently to attain different levels of oxidation. Of them, GT is made from the unfermented dried leaves of the plant [10,11].
Due to its widely known medicinal properties, including the role as anti-carcinogenic, antioxidant, anti-inflammatory and anti-aging [12,13], GT has been considered a medicine and a healthful beverage since ancient times. Traditional Chinese Medicine has recommended this plant for headaches, body aches and pains, digestion, depression, detoxification, as an energizer and, in general, to prolong life [14].
GT mainly consists of polyphenols (~90%), amino acids (~7%), theanine, proanthocyanidins, and caffeine (~3%). Among the different polyphenols, flavanols and flavonols are the major constituents. Catechins are the predominant form of the flavanols and are consisted of catechin (C), epicatechin (EC), gallocatechin (GC), epigallocatechin (EGC), epicatechin gallate (ECG), gallocatechin gallate (GCG) and epigallocatechin gallate (EGCG), the major catechin present in GT [15,16]. This composition, however, depends on season, climate, horticultural practices, and age of the leaf [9], with oldest leaves presenting more catechins and polyphenols and the youngest ones more caffeine content [17].
The health-promoting effects of GT are mainly attributed to its rich source of polyphenol content, which represent approximately 30% of dry weight of the fresh leaf [8]. More specifically, its catechins content, particularly EGCC, the most active catechin in GT, is best correlated with their well-known antioxidant and anti-inflammatory properties, leading to their evaluation in a number of diseases such as cancer, cardiovascular and neurodegenerative diseases [18-20], as well as obesity and metabolic syndrome (MetS), since these illness can be related when its complex physiopathology is considered [20].
Therefore, the aim of this review was to evaluate the effect of consumption of GT on treatment of obesity, regarding anthropometrics and biochemical parameters in humans and experimental models.
A systematic review evaluating the effect of GT intake and changes on the anthropometric and biochemical profile. This review was registered in the international prospective register of systematic reviews PROSPERO network (registration n°. CRD42021259754). At the same time, a systematic review of experimental models of obesity evaluating the effect of GT in tissues affected by the disease was realized.
Between January and August 2021, searches were performed with the use of MEDLINE (via PubMed), LILACS, COCHRANE, SCIELO and related articles. Besides, bases of unpublished articles and thesis bases were also used as sources of articles in unpublished studies. No period or language restrictions were used in the search strategy. Keywords were "Green tea", "Camellia sinensis", "Epigallocatechin", "Herbal medicine" and "Obesity", and it was used as indexing terms, like MESH and Entree when available, and text words.
Clinical trials: Inclusion and exclusion criteria were developed using the Population, Intervention, Comparators and Outcome (PICO) method.
Furthermore, we determined the following main parameters to evaluate each alleged effect of GT: a) The effect of green tea on body weight: BMI, weight, circumferences, body fat mass, lean body mass; b) The effect of green tea on the inflammatory profile: Interleukins, Reactive C Protein (CRP), Tumor Necrosis Factor (TNF); c) The effect of green tea on glycemic profile: Serum glucose, Insulin, Glycated Hemoglobin (HbA1c), Homeostatic Model Assessment of Insulin Resistance (HOMA-IR); d) The effect of green tea on cardiovascular health: Total cholesterol (TC), Triglycerides (TG), High-density lipoprotein cholesterol (HDL), Low-density lipoprotein cholesterol (LDL), Free fatty acids (FFA), blood pressure (BP), serum and endothelial biomarkers of oxidative stress. To better analyze the collected data, we also included other relevant results to each topic, when present.
The population of interest was adults and elderly people at the age range 18-70 years old with obesity with or without related comorbidities. The clinical trials had to compare the intake of GT to a placebo or no intervention. We excluded studies in which GT was administered with fermenter microorganisms or other herbs, co-intervention with drugs or was produced synthetically. Moreover, we have excluded literature reviews, opinion papers, and abstracts with irretrievable full text.
Finally, the results were classified according to the mentioned p value, in which a p value higher than 0.05 was considered not significantly relevant, therefore mentioned as a neutral effect. Jointly, a p value lower than 0.05 was considered statistically relevant, therefore mentioned as a reduction or elevation effect, considering the respective placebo group (Table 1 and Table 2).
Table 1: Main results for clinical studies. View Table 1
Table 2: Main results for experimental studies. View Table 2
Experimental models: Similarly to what was done for clinical studies, we determined the following main parameters to evaluate each alleged effect of GT: a) The effect of green tea on body weight: body weight, body weight gain, total body fat mass, total body free-fat mass; b) The effect of green tea on the inflammatory profile: Interleukins, Reactive C Protein (CRP), Tumor Necrosis Factor (TNF); c) The effect of green tea on glycemic profile: Serum glucose, Insulin, Homeostatic Model Assessment of Insulin Resistance (HOMA-IR); d) The effect of green tea on cardiovascular health: Total cholesterol (TC), Triglycerides (TG), High-density lipoprotein cholesterol (HDL), Low-density lipoprotein cholesterol (LDL), Free fatty acids (FFA), serum and endothelial biomarkers of oxidative stress. We also included other relevant results to each topic when present.
We included all studies that performed a diet-induced obesity in animal models and used green tea administered only as a treatment for obesity. Therefore, genetic-induced or medicine-induced obese animals and GT administered at the same time of diet-obesity induction were excluded. Moreover, studies with non-mammals were all excluded. We also excluded studies in which GT was administered with fermenter microorganisms or other herbs or was produced synthetically.
We selected all randomized clinical trials and experimental model studies meeting the eligibility criteria for this paper. The software ENDNOTE (EndNote X9.3.1, Clarivate Analytics) was used to exclude duplicates, and read titles and abstracts. The titles and abstracts were rescreened in duplicate by two investigators (LSF and IAD) to check for eligibility criteria, with differences resolved by consensus. Full-text papers were independently assessed for eligibility by each investigator (LSF and IAD). Disagreements between reviewers were resolved by a third author (PBG).
Data of each individual study was extracted independently by two investigators (IAD and LSF), including the year when the study was performed and reported, study design, sample size, type of population studied, sex, age, anthropometrics parameters and biochemical and pro-inflammatory profile. Collected data from experimental studies also included animal's genetic line and obesity's model, period of diet-obesity induction, sex, age, anthropometrics parameters, biochemical and pro-inflammatory profile, and specific tissue biomarkers.
In systematic research of literature, 3377 studies were found. Of these, 2060 were duplicates and, after title and abstracts screenings, 204 full-text citations were evaluated. Sixteen studies total met the eligibility criteria and were included in the systematic review; eleven [21-31] eligible clinical trial and five [32-36] experimental studies (Figure 1).
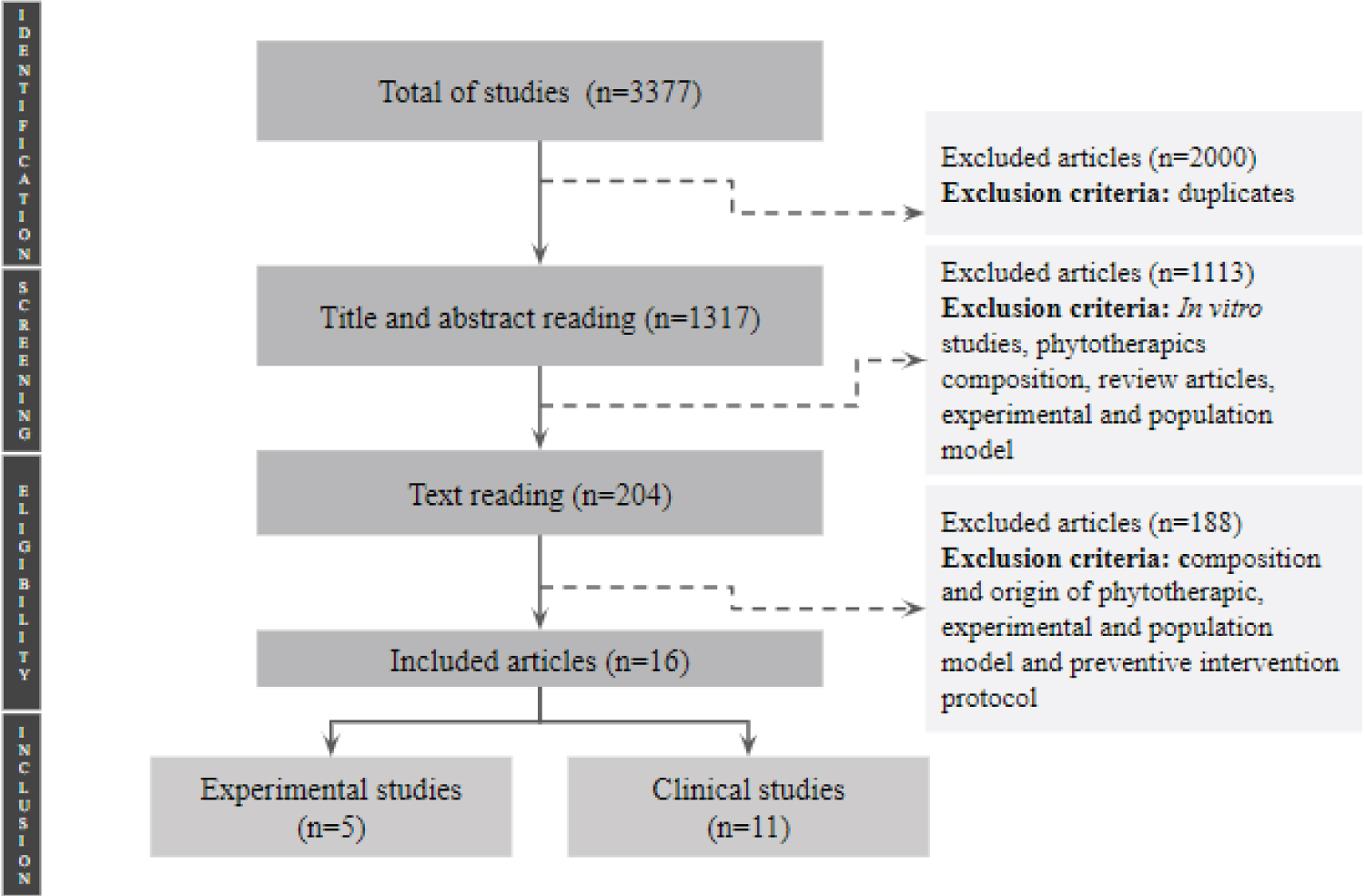 Figure 1: Flowchart showing the process of article selection.
View Figure 1
Figure 1: Flowchart showing the process of article selection.
View Figure 1
The characteristics of the included clinical trials are presented in Table 3, and the results are described in Table 1. Out of the eleven selected studies, 8 were randomized double-blinded placebo-controlled clinical trials, 2 were randomized single-blinded placebo-controlled clinical trials, and one was a prospective observational study. The samples of the studies varied from 6 to 83 participants, with mean age of 20 to 70-years-old, and total study time ranged from 4 to 16 weeks. Also, the amount of GT offered to intervention arms varied substantially between studies: 300 to 2576 milligrams a day for capsules, and 928 to 1000 milligrams a day for tea.
Table 3: Characteristics of clinical studies. View Table 3
Completely, the characteristics of the included experimental studies are presented in Table 4, and the results are described in Table 2. All five studies used a diet-induced obesity experimental model for mice or rats, followed by the treatment with GT. Total study time ranged from 8 to 32 weeks, and the samples varied from 24 to 48 animals, distributed in 2 or 4 distinct groups. The amount of GT offered to intervention arms also varied substantially between studies: 50 to 500 mg/kg/day for oral gavage [33,34]; 2% of the diet when administered with food [32]; and 0.5% (wt/vol) when diluted in water [35,36].
Table 4: Characteristics of experimental studies. View Table 4
Eleven clinical studies [21-31] with 282 individuals provide estimates for the relationship between consumption of GT and obesity treatment. Three studies [22,25,27] demonstrated decreased BMI and body weight after intervention with doses of 1430 mg (capsule) [22], 208 mg (capsule) [24], 870 mg (capsule) and 928 mg (tea) [27] of total catechins. Seven studies [21,23,24,26,28,30,31] have not shown these results with different doses. Only two studies [22,25] demonstrated decrease of waist circumference after administration of 379 mg (capsule) of GT, which was not found with other doses.
In experimental models, reduction in body weight was observed in two out of the five studies that met the criteria. Only 4 of them [33-36] evaluated body weight and, of those, two [33,36] did not show a significant difference, while the other two [34,35] showed a decrease in the same parameter after the administration of a dose of 50 mg/kg/day (capsule) and 0.5% (wt/vol) (drinking water), respectively. This result was followed by a significant decrease also in body weight gain [33-35], but unchanged body fat mass [33,34]. Although no significant difference in adiposity was observed, has a decreased adipocyte size after administration of GT [33].
Interestingly, one experimental study [33] evaluated and showed a decrease in mRNA expression of Diacylglycerol Acyltransferase (DGAT) and an increase in mRNA expression of Adipose Triglyceride Lipase (ATGL) and mRNA expression of Hormone-Sensitive Lipase (HSL).
In humans, two studies evaluated TNF [24,26] and only one of them [26] showed a significant decrease, using 379 mg of GT. Two clinical studies evaluated Interleukin 6 (IL-6) serum concentration [24,27] but none of them showed significant increase nor decrease in this parameter. Four studies [25-27,30] evaluated CRP, in which one of them showed reduction in this parameter [26].
Regarding experimental studies, one of them has evaluated serum TNF [33] but has not shown significant reduction. However, in white adipose tissue, one study has evaluated and presented a reduction in TNF after 12 weeks of GT treatment [34]. Two studies evaluated Interleukin-1β (IL-1β) and Interleukin-6 (IL-6) serum concentration [33,35] and, for both parameters, one [33] showed no significant changes after 12 week treatment, while other [35] showed a decrease after the same time period with administration of GT diluted in water at 0.5%.
All clinical studies [21-31] analyzed glycemic profile after intervention with GT. Of these, studies using whole plant extract in doses of 379 milligrams (capsules) [26], and 1000 milligrams (tea) [22] showed a decreased HOMA index after GT treatment. Also, leaf extract containing 2576 milligrams (capsules) was capable of decreasing Hb1Ac [23].
None of the clinical trials showed significant effects of GT treatment in fasting glucose, and only one of them showed reduction in postprandial glucose and insulin [22]. Four studies evaluated Hb1Ac concentration, but only one revealed significant reduction [23]. Other than that, eight studies evaluated HOMA-IR, and two showed reduction and better insulin sensitivity [22,26], both after 12 weeks of treatment with GT. Finally, eight studies evaluated fasting insulin and, of those, one revealed reduction [26].
Similarly, obese male Wistar rats showed decrease in oral glucose and insulin tolerance tests after 12-week treatment with 500 mg/kg/day GT by oral gavage [33]. On the other hand, obese male Swiss rats showed increased serum glucose, insulin and HOMA-IR levels after treatment with 50 mg/kg/day GT also by oral gavage [34]. At last, out of the 5 studies that met the criteria, only these 2 show results regarding some glycemic parameter.
Four clinical studies showed decreased TG serum concentration in GT treated groups with doses of with doses of 1430 mg (tea) [22], 208 mg (capsule) [25] and 150 mg (capsule) of total catechins [21] within 8 to 12 weeks of treatment; one study demonstrated TC reduction [25]; and two studies pointed LDL cholesterol reduction after GT treatment [25,31] for 12 weeks. All eleven studies evaluated HDL levels but none of them showed an alteration in this parameter [21-31].
Three out of the nine clinical trials that evaluated blood pressure showed significant reduction [21,24,26], using doses of 150 to 1500 mg of GT. Two out of three clinical trials that evaluated oxidative stress also showed reduction in this parameter after 8 weeks of treatment with capsules containing 150 mg of GT [21] and after 12 weeks of treatment with capsules containing 379 mg of GT [26]. Specifically, one study evaluated and showed a decrease in Malondialdehyde (MDA) and Hydroxynonenal (HNE) serum concentration, important biomarkers of oxidative stress [27], after 8 weeks of treatment.
Regarding experimental studies, out of the 6 studies that met the criteria, only 2 of them [33,34] evaluated cardiovascular health related parameters. Both of them showed no significant difference in serum dosage of TC, LDL, TG or HDL [33,34]. These 2 studies also evaluated FFA, and one [33] has shown significant decrease, while the other one [34], has not. Regarding liver dosages, one study [33] evaluated and showed significant reduction of the three aforementioned parameters (TC, TG and fat accumulation).
Obesity is a metabolic disorder characterized by an excess accumulation of fat in the body due to energy intake exceeding energy expenditure [37]. The most serious medical consequences of obesity are a result of endocrine and metabolic changes; most notably, type 2 diabetes mellitus (TDM2), cardiovascular disease (CVD), and increased risk of cancer [38].
The management of obesity and its related complications has evolved in recent years. Nowadays, due to their medicinal properties, phytotherapics are emerging as an alternative target for therapeutic approaches [39].
Therefore, the aim of this systematic review was to evaluate the consumption of GT on obesity-related metabolic and physiological changes, specifically on body weight and composition, inflammatory and glycemic profile and cardiovascular health, including lipid profile and oxidative stress. For that, further into this topic we shall also discuss the possible mechanisms for each allegated GT effect aforementioned in the results.
Mainly, the deleterious effects of obesity results from two factors: Adipose tissue excessive expansion and increased secretion of pathogenetic products from enlarged fat cells [40]. It is evident now that white adipose tissue (WAT) is the source of production of a multiplicity of secretory factors, playing an active role as an endocrine organ [41]. Moreover, body fat distribution is considered an important predictor of the adverse health consequences of obesity, with upper-body obesity, especially increased visceral fat, associated with a higher risk of developing obesity-related metabolic dysruptions [42].
In this manner, some studies show that GT treatment promotes weight loss, considering BMI [22,25,27], body weight [22,27] and circumferences [22,25] in human subjects, as well as a lowering effect on body weight [34,35], body weight gain [33-35], and total body fat [36] in animals. Although the mentioned data suggests the beneficial effects of GT on weight loss, it is also important to highlight that most of both human and animal studies reported no significant changes in at least one of the aforementioned parameters [21,23,24,26,27-31,33,34,36], enforcing that it is still not clear whether GT treatment has a lowering body weight effect or not (Table 1 and Table 2).
When evaluating weight loss in humans, GT was effective in tea form [22] or capsule [29] only when consumed by significant clinically obese individuals (IMC > 35) with mixed comorbidities. Furthermore, regarding to BMI, the dosage of 379 mg of GT in obese individuals without associated comorbidities has not shown significant differences [26]. In obese individuals with cardiovascular disease, 1000 mL of GT appeared to be enough to demonstrate significant BMI reduction [22,25]. It may suggest that the GT treatment response also differs depending on which comorbidities the individuals carry.
Interestingly, in experimental models, GT showed a positive effect on adipogenesis and lipolysis, inducing a decrease in mRNA expression of DGAT, a key enzyme in the synthesis of triglycerides, and an increase in mRNA expression of ATGL and HSL, proteins related to lipid hydrolysis, suggesting how GT might induce changes in lipid-metabolism at a molecular level [33]. Both contribute to WAT remodeling by reducing its deleterious effects in expansion observed in obesity.
Adipose tissue expands by two mechanisms: hyperplasia (cell number increase) and hypertrophy (cell size increase). Hyperplastic growth appears only at early stages in adipose tissue development. Meanwhile, hypertrophy occurs prior to hyperplasia to meet the need for additional fat storage capacity in the progression of obesity [43]. In general, hypertrophic cells are considered less metabolically favorable and are associated with pathophysiological conditions, such as arteriosclerosis, diabetes, osteoporosis, and cancer [44]. GT also demonstrated was shown to be effective in reducing adipocyte size in animal's WAT, implying that even in the absence of a positive modulation in its mass, it might be able to promote effective changes in tissue morphology [33].
As mentioned, obesity is considered a state of chronic low-grade inflammation. The adipose tissue expansion and infiltration of cells stimulates them to release inflammatory mediators such as TNF and IL-6, and reduces production of adiponectin, predisposing to a pro-inflammatory state and oxidative stress [45]. In the present review, two clinical trials showed that GT did not influence serum IL-6 level [24,27]. Only one study [26] showed reduction in TNF and CPR after a 3 months follow-up, administering a dose of 379 mg (Table 1).
In animal models, GT did not affect TNF level [33], but seemed to have a beneficial effect reducing IL-1β and IL-6 only after a 4 months follow-up [33,35]. However, in WAT, GT showed a positive influence in reducing TNF protein expression, suggesting that it might ameliorate pro-inflammatory biomarkers at a local level [34].
Plasma TNF and FFA levels are all elevated in obesity and play a role in causing insulin resistance by interfering in insulin-receptor activation and insulin signaling that, ultimately, can lead to TDM2 [46]. Our results in the glycemic profile showed that GT had no effects on fasting glucose but presented a positive effect on postprandial glucose and insulin, fasting insulin and HOMA-IR in humans when the whole plant extract was used [22,26]. Besides, GT also was effective in reducing Hb1Ac when the leaves part was used, in concentration of 2576.4 mg of EGCC [23].
Consistently with clinical results, experimental models showed no effect in fasting glucose, and one positive effect on oral glucose tolerance test and insulin tolerance test [33], suggesting that GT may promote an increase in intestinal glucose absorbance and clearance. Also, only one study evaluated serum glucose and insulin and HOMA-IR and showed negative correlation after GT treatment in those parameters [34]. The study highlighted that GT treatment could improve insulin resistance and metabolic profiles in a normolipidemic diet, but the same could not be said for high-fat diet-fed mice, considering their results and others mentioned in their discussion [34].
The typical dyslipidemia associated with obesity consists of increased TG and FFA, decreased HDL-C with HDL dysfunction and increased LDL-C [47], promoting oxidative stress, inflammation and endothelial dysfunction [48]. These abnormalities have been shown to be atherogenic, and therefore playing a key role in the development of CVD [49]. Our data showed that GT was effective in reducing TG, TC and LDL-C serum concentration, but demonstrated no effects on HDL-C levels in clinical trials (Table 1) [21,22,25,26,31].
Animal models did not present any beneficial effects of GT on TG, TC, LDL-C and HDL-C [33,34], but showed a positive effect on FFA after GT treatment for 12 weeks [33] (Table 2 and Table 4). Moreover, it was shown that GT had a beneficial effect on hepatic TG, TC and fat accumulation, which indicates that it might at least contribute to alleviate ectopic fat deposition in the liver, closely related to non-alcoholic fatty liver disease in obesity [33].
Jointly, obese individuals are more susceptible to develop cardiovascular disease when compared to eutrophic subjects, such as higher blood pressure. At the same time, hypertension presents itself as a great risk factor for the development of heart attack and stroke. In this manner, some data presented in this study also showed that GT was effective in reducing BP in humans [21,24,26].
Besides, the organism's imbalance between oxidative and antioxidative functions requires attention. Thus, two clinical trials evaluated GT treatment in oxidative stress, and showed a positive effect in reducing this parameter, specifically in two molecules related to oxidative stress [25,26]. MDA is the principal product of polyunsaturated FA peroxidation [50]. HNE is a major end product of Ω-6 polyunsaturated FA peroxidation, playing a crucial role in cell processes such as oxidative stress signaling and cell death [51].
Several studies have suggested that oral consumption of GT may attenuate excess body fat related to positive balance energy in obesity. Much of the work in humans has focused on the effects of GT on thermogenesis and substrate oxidation, both of which are mediated by sympathetic nervous system (SNS) activity. Other potential mechanisms include modifications in appetite control, down-regulation of enzymes involved in hepatic lipid metabolism and decreased nutrient absorption [52].
Indeed, the main purpose for GT consumption found in our clinical findings is its potential ability to ensure weight loss. One of the mechanisms to explain body weight reduction evident in some of the studies is due to the GT catechins and caffeine content, which seem to enhance energy expenditure and promote fat oxidation through activation of the SNS [53]. Another option is the fact that EGCG could be able to decrease the secretion of specific hormones [23]. Ghrelin is commonly called "hunger hormone" and it stimulates appetite and increases food intake. Adiponectin is an adipocyte-derived peptide that plays an important role in lipid metabolism. As a result of EGCG effects, these hormones might suffer a healthy decrease, favoring weight loss and, therefore, health benefits in obese individuals. Consistent with some of our human results were demonstrated that GT extract reduced body weight, BMI, body fat mass, waist circumference, hip circumference, visceral fat area, and subcutaneous fat area in overweight and obese Japanese subjects [54]. Also were demonstrated that GT synthetic capsule was effective in reducing body weight, but without significant differences in BMI or waist circumference in Thai obese subjects [55]. However, did not found any differences in body weight, BMI and waist circumference in the obese adolescent and adult women group treated with GT extract and the placebo group, which are closely related to cardiovascular risk [56].
The beneficial effects of GT on inflammatory profile might be linked to the anti-inflammatory effects of various antioxidant polyphenols in its content, which are capable of induce an increase in the production of anti-inflammatory cytokines and a decrease in the pro-inflammatory cytokine's levels [57].
Consistent with most of our results, the effect of GT and its catechins has studied on gene/protein expression in cell and animal experiments to reveal their beneficial effects on various diseases, demonstrating that it affected the expression of inflammation-associated genes and proteins such as TNF, IL-1, and matrix metalloproteinases (MMP) [58]. Also was demonstrated that EGCC was able to inhibit the protein expression of IL-1β, IL-6, monocyte chemotactic protein-1 (MCP-1), chemokine expressed by inflammatory cells, and other molecules related to inflammation by inhibiting the activation of NF-κB and c-Jun N-terminal Kinase (JNK)-MAPK in human chondrocytes, transcription factors crucial in the inflammation signaling pathway [59]. In summary, this shows us the promising effects of GT in the inflammatory profile.
Evidence suggests that GT, predominantly EGCC, may favorably modulate insulin sensitivity and glucose homeostasis in many different ways such as by improving the absorption of glucose into skeletal muscle, increase the expression of glucose transporter 4 (GLUT 4), rehabilitate damaged beta-cells, which are responsible for insulin production, or attenuate pro-inflammatory pathways that could interfere in insulin sensitivity [14,60,61]. Still, GT extract did not present any significant effects on blood glucose and HbA1c levels, pro-inflammatory markers or insulin resistance in subjects with borderline diabetes or diabetes [62]. But, demonstrated that GT polyphenols significantly increased basal and insulin-stimulated glucose uptake of adipocytes in rats [63]. However, moderate consumption of EGCC can significantly reduce plasma glucose concentrations in overweight individuals undergoing regular exercise [64]. By contrast, this result was not observed in the present review.
In our findings one experimental study presented a significant decrease in oral glucose and insulin tolerance tests at the same time as a reduction in adipocyte size [33], indicating that changes in WAT morphology may also be linked to a better glycemic control. Although none of the studies in both animals and humans exhibited a positive effect of GT on fasting glucose, it was shown that GT might interfere in glucose metabolism and insulin sensitivity, suggested by the positive effect demonstrated on HOMA-IR, serum HbA1c, fasting insulin and both postprandial glucose and insulin in some of the clinical trials. However, that GT effects on glucose and insulin remain controversial.
One of the important functions of GT polyphenols is their potential vascular protective effect by anti-oxidative, anti-hypertensive, anti-inflammatory, anti-proliferative, anti-thrombogenic, and lipid-lowering activity. It is hypothesized that they can scavenge free radicals, chelate redox active transition metal ions, and inhibit redox active transcription factors, alter enzymes involved in lipid biosynthesis, and reduce intestinal lipid absorption [65].
Indeed, as we presented in this review, GT seems to have a potential favorable effect on lipid profile. Due to rather poor absorption and greater availability of GT catechins in the intestinal lumen, it is likely that the lipid-lowering effect of GT and its constituents is mediated largely via their influence on the intestinal processes involved in digestion and absorption of lipids [66]. In ovariectomized rats, GT significantly lowered the intestinal absorption of cholesterol and α-tocopherol [67]. Moreover, GT extract significantly inhibited gastric and pancreatic lipase activities in vitro [68].
ROS are by-products of aerobic metabolism that when elevated in cells can cause damage to lipids, proteins and DNA and lead to an oxidative stress [69]. Oxidative stress can have an impact on many biological processes including apoptosis and autophagy, as they can harm different molecules and organelles and lead to an inflammatory response in the host. The cells have evolved a balance system of antioxidant enzymes such as catalase (CAT), glutathione (GSH) and glutathione peroxidases (GPxs), which can neutralize an excess amount of ROS inside the body [70].
Consistently with our results, catechins reduce ROS and MDA serum and blood levels content in genetic-obese mice [61]. Specifically, EGCC was able to attenuate TNF promoted ROS generation by its ROS scavenging functions, suggesting that it may also improve whole-body inflammation-related disturbances such as insulin resistance.
Despite numerous studies reporting the influence of GT on obesity and obesity-related comorbidities, the results remain controversial. All the studies conducted with Asian subjects have shown positive results about the anti-obesity effects of GT constituents. On the other hand, studies with Caucasian subjects reported mixed results [71]. Possible factors that might influence on multiplicity of results in clinical trials might be linked to characteristics of the population (ethinicity, age, sex, BMI), period of treatment, dosage, presence of drug-therapy or association with other eating habits or lifestyle interventions. Experimental studies may be influenced by animal's line and sex, period of treatment, dosage and type of administration.
Furthermore, it is worthy to note that none of the experimental nor clinical studies evaluated the effect of GT associated with changes in eating habits and lifestyle activities, such as calorie intake restriction and regular physical exercise, considered the key intervention in obesity treatment. Therefore, it is possible that the overall effects of GT consumption might have been attenuated since it was used as a conventional treatment instead of a complementary one.
In conclusion, the present review showed that there is trend indicating that GT can potentially influence some of the physiological changes related to obesity development and progression, contributing to the treatment. In diet-induced obese animals, GT tended to reduce body weight, and improve serum inflammatory biomarkers IL-6 and IL-1β, and glycemic control. Similarly, GT was inclined to reduce BMI and waist circumference, and improve serum inflammatory biomarkers TNF and CRP, in addition to lipid profile, especially reducing TG in obese subjects, with or without related comorbidities. Finally, more studies are requested to be carried out in exclusively obese subjects in order to better clarify the potential beneficial effects and its mechanisms regarding the consumption of GT an obesity treatment and in the overall body health.