The aim of our study was to examine both age and gender-related alterations in collagen expression of the transverse carpal ligament (TCL) in patients with idiopathic carpal tunnel syndrome (CTS).
Resected TCLs were collected from 10 patients undergoing open carpal tunnel decompression. These were randomly divided equally into two groups of five patients, with equal numbers of men (average age 49.6) and women (average age 57.4). Histological staining [Hematoxylin & eosin and Picrosirius red (PSR)] and Western blot analysis were performed on the resected tissue.
Data from the histological analysis showed a 73% increase in fibroblast cell densities in the TCL specimens from the CTS patients. The PSR staining-polarization microscopic and immunoblot analysis data shows that men have significantly increased collagen I and decreased collagen III (P ˂ 0.05) compared to women. An age-related decline was observed in the expression of collagen I in both sexes, and the ratio of collagens III to I was significantly increased (P ˂ 0.05) in women compared to men. The major component of the TCL in both sexes was found to be Collagen type VI. Levels of collagens II, V and X were also elevated to lesser extents.
Our data enhances the understanding of collagen alterations in the transverse carpal ligament in CTS. Collagens I and III are significantly elevated, especially in males, while other collagen isoforms, II, V, VI, and X, are also up-regulated. Moreover, there appears to be a general decrease in the up-regulation of collagen levels as a function of advancing age.
Carpal tunnel syndrome, Transverse carpal ligament (TCL), Collagen, Picrosirius red staining, Western blotting
Carpal tunnel syndrome (CTS), of idiopathic origin, requiring surgery is estimated to occur in approximately 4% of the population [1,2]. CTS is a neuropathy of the median nerve at the wrist and is more common in women than in men [3]. The carpal tunnel is a semi-rigid canal with carpal bones making up the floor and lateral walls, and the transverse carpal ligament (TCL) forming the roof; the median nerve runs through the carpal tunnel underneath the transverse carpal ligament and along with the long flexor tendons. Most CTS cases are idiopathic, but some systemic conditions, notably, diabetes [4], hypothyroidism [5], alcoholism [6], rheumatoid arthritis [7], and renal dialysis [8], can predispose to this pathology. Predispositions based on gender have been documented, including females in menopause [9].
CTS has previously been demonstrated to be associated with alterations in collagen synthesis [10,11]. Therefore, determining the levels of the collagen isoforms involved is a fundamental step in the understanding of the pathophysiology of CTS. Human TCL is known to be comprised of collagen types I, III-VI, and proteoglycans. Collagen types I, III & VI have been identified as contributors to the pathogenesis [10], although other smaller chained collagens, such as types II, V, IX, and type X may also be related to the mechanism. To our knowledge, there are relatively few histological [10-13] and no biochemical quantitative analyses for the expression of collagen subtypes regarding the TCL. The aim of our study was to both histologically and biochemically assess the TCL harvested during open carpal tunnel surgery in order to identify age and gender-related changes in collagen subtype expression.
This study was approved by the IRB at our University and informed consent was obtained from all the patients prior to surgery. The study group comprised 10 patients (5 men, 5 women) who were treated surgically for idiopathic unilateral CTS between January 2011 and December 2011. The average age for men was 49.6 years (range 42- 63 years) and an average age of 57.4 years (range 48 - 69 years) for women. Five patients were affected on the right and 5 on the left. Patients with a previous health history of diabetes mellitus, autoimmune disorders, renal failure, arthritis or pregnancy were excluded from the study. Prior to surgery, all the patients had received conservative pre-op treatment with a splint, NSAIDs, and vitamin B12, but none of the patients had received steroid injections. All patients had experienced pain and numbness in the median nerve distribution for > 6 months (average 12 months, range from 6 to 48 months), but exacerbation of symptoms had led them to choose surgery, following the failure of conservative management.
During carpal tunnel surgery, a central 5 mm strip of the TCL was excised, and a median nerve neurolysis was performed. The excised TCL specimen was split into 2 equal halves, one half was fixed in 10% formalin for histological processing and the second was stored immediately in dry ice for Western-blot analysis.
Harvested specimens were fixed in paraffin, sectioned into 10 μm thin sections, and stained with hematoxylin and eosin (HE). Next, the specimens were dewaxed in xylene and rehydrated in graded methanol (99% to 70% (v/v)) in distilled water, H&E staining was performed. Sections were examined with attention to inflammation, amyloid deposition, mucoid change, synovial chondromatosis, fibrosis, vasculature, cell nucleus distribution and density.
Tissue specimens were fixed in paraffin with a 10% neutral buffered formalin solution, sectioned into 10 μm thin sections, and stained with Picrosirius Red [14,15] (PSR). Organization of the collagen fibers were evaluated using birefringence measurements, and the amount of collagen content was determined utilizing PSR staining.
Birefringent collagen were visualized using a Nikon ECLIPSE EP200 microscope (Nikon Corporation, USA), which was fitted with a polarizing filter, the background was black and the stained collagen fibers were displayed as green through red colors. Slides were then captured with a Spot RT slider cooled CCD camera (Diagnostic Instruments, Inc., Sterling Heights, MI) as digital images to score the slide in an objective and quantitative system. Five high powered fields were captured from each slide, and all slides were photographed on the same day to maintain consistency of the light source and to avoid any variables.
Image morphometry was determined using Image J (Version 1.44) analysis software (National Institutes of Health, Bethesda, MD) [16]. Areas of green (type III collagen-like) and red (type I collagen-like) were calculated for each of the captured fields. The pixels counted were defined by selecting ranges in the red, green, and blue channels that selected the color green or red. The settings profiles were maintained throughout the analysis process. The ratio of type III to type I collagens was calculated for each field, by dividing the area for green by the area for red, and the average and standard error of the mean were determined for each treatment.
The harvested tissues, approx. 20 mg wet weight each, were rinsed in PBS prior to homogenization in 15-fold excess of extraction buffer (20 mM Tris pH 7.4, 150 mM NaCl, 1 mM EDTA, 2% SDS, and proteinase inhibitor cocktail, Roche). The homogenized sample was centrifuged at 14,000 rpm for 10 min at 4 ℃ (Biofuge Pico, Heraeus), and the supernatant was removed and stored at -80 ℃ (Thermo Scientific Forma, -86 ℃ ULT Freezer, USA). A BCA Protein Assay Kit (Pierce, Thermo Scientific, USA) was used to determine the total protein content in each sample [17].
The samples' constant total protein was resolved using 7% SDS-PAGE and transferred on to nitrocellulose membranes (Pall, East Hill) via a semi-dry transfer cell apparatus (Trans-Blot SD, Biorad, USA). Immuno-blotting was done with anti-collagen I, collagen II, collagen III, collagen V, collagen VI and collagen X antibodies (Abcam, USA) used at 65 ng/ml for collagen I, 2 μg/ml for collagens II and V, 4 μg/ml for collagen III, 100 ng/ml for collagen VI, and 500 ng/ml for collagen X. Calnexin served as a loading control in each sample and was probed with rabbit anti-calnexin polyclonal antibody (2 μg/ml; Abcam, USA). Goat anti-rabbit IgG-peroxidase (GE Healthcare, Piscataway, NJ) at 1:8000 dilution with ECL was used as the secondary antibody detection system (Fischer Scientific, USA). For each independent sample, immuno-blotting was done at least in duplicate.
For semi-quantification of immunoblot signals, the densities of bands with specific antibodies, using calnexin as a positive control, were measured using Image J software (NIH, USA).
A students t-test was performed to evaluate significant differences between females and males, with P < 0.05 taken as the level of significance.
Sectioned specimens of the TCL were stained with H & E and crystal violet (not shown here) and examined (Figure 1). The specimens from TCL were pathologically evaluated according to parameters of the presence of amyloid deposits, fibrosis, edema, lipomatosis, vascular proliferation, and perivascular lymphocytic infiltration. H & E stained TCL sections of CTS patients showed a dense connective tissue with aligned fibroblasts intermingled between collagen fibers and few areas of fibrosis.
 Figure 1: Haematoxylin and eosin staining of specimens [young (A) and old (B) aged women, and young (C) and old (D) aged men] of transverse carpal ligament (TCL) from showing collagen fibres, vascular proliferation, lipomatosis, and perivascular lymphocyte infiltration (H&E x 100).
View Figure 1
Figure 1: Haematoxylin and eosin staining of specimens [young (A) and old (B) aged women, and young (C) and old (D) aged men] of transverse carpal ligament (TCL) from showing collagen fibres, vascular proliferation, lipomatosis, and perivascular lymphocyte infiltration (H&E x 100).
View Figure 1
Semi-quantitatively, edema, fibrosis and vascular proliferation were classified as none (0), mild (1), moderate (2). Lipomatosis, perivascular lymphocyte infiltration and amyloid deposition were classified as none (0) and present (1) (Table 1). A p-value less than 0.01 was accepted as significant.
Table 1: Semi-quantitative measurement criteria of edema, vascular proliferation and fibrosis. View Table 1
PSR staining of histologic sections was used to assess collagen deposition in the TCL (Figure 2). Image analysis quantification of PSR staining of the ligament revealed no significant differences in collagen deposition in both women and men. On the ligament, however, there was significantly greater (P ˂ 0.05) collagen deposition in women than men.
 Figure 2: Polarized light microscopic pictures showing collagen types I and III, and merge of green and red proteins in young and old age of women and men.
View Figure 2
Figure 2: Polarized light microscopic pictures showing collagen types I and III, and merge of green and red proteins in young and old age of women and men.
View Figure 2
During our analysis, statistically significantly greater amounts of type I collagen fibers were observed in men (P ˂ 0.04), and statistically significant differences in the amounts of type III collagen were also found between women and men (P ˂ 0.05). We also found a reduced total renewal rate for collagen type I and increased total renewal rate for collagen type III with increasing age in both genders (Figure 3).
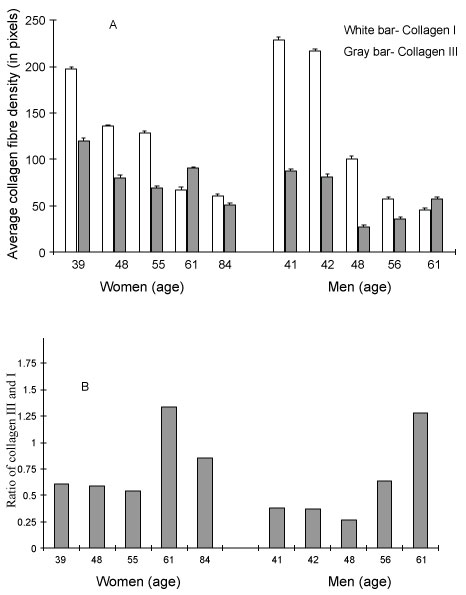 Figure 3: Picrosirus red staining-polarization showing average collagen fibre density (A) and ratios of green (indicative of type III collagen) to red (indicative of type I collagen) staining (B) in the TCL. Results are represented as mean ± standard error of the mean.
View Figure 3
Figure 3: Picrosirus red staining-polarization showing average collagen fibre density (A) and ratios of green (indicative of type III collagen) to red (indicative of type I collagen) staining (B) in the TCL. Results are represented as mean ± standard error of the mean.
View Figure 3
Collagen types I, II, III, V, VI, and X in the TCL were specifically investigated in the western blot analysis (Figure 4). Men presented significantly higher collagen I (P ˂ 0.02) and less collagen type III (P ˂ 0.05) than women (Figure 5). The ratio of collagen types III to I was significantly increased (P ˂ 0.05) in women (Figure 5).
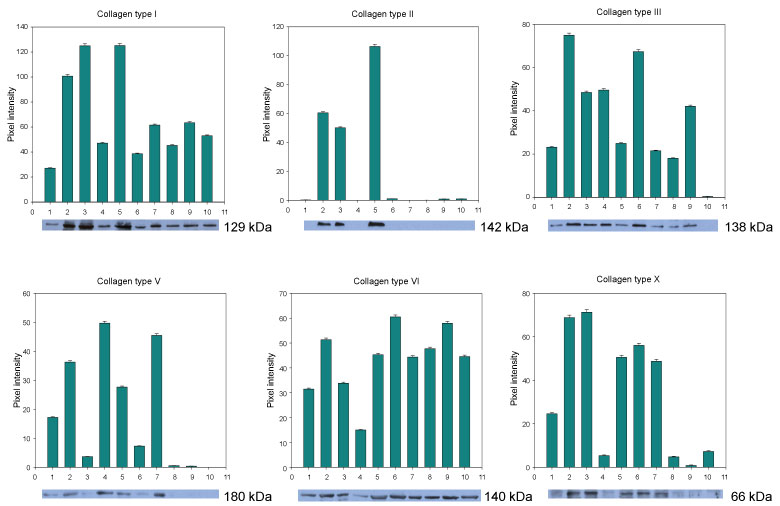 Figure 4: Western blot analysis of collagen types I, II, III, V, VI and X in TCL tissues. Results are represented as mean ± standard error of the mean.
View Figure 4
Figure 4: Western blot analysis of collagen types I, II, III, V, VI and X in TCL tissues. Results are represented as mean ± standard error of the mean.
View Figure 4
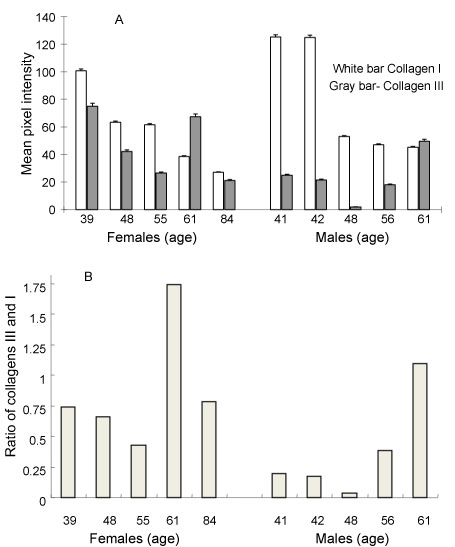 Figure 5: Western blot analysis showing mean pixel intensity of collagen types I & III (A) and the ratios of collagen types III and I (B). Results are represented as mean ± standard error of the mean.
View Figure 5
Figure 5: Western blot analysis showing mean pixel intensity of collagen types I & III (A) and the ratios of collagen types III and I (B). Results are represented as mean ± standard error of the mean.
View Figure 5
Published literature has reported histologic differences of the TCL and tenosynovium in idiopathic CTS. Vascular sclerosis [18], synovial hyperplasia, increased fibrous tissue, and edema [19] have been documented. However, differences between patients and controls have not been reported in histological morphology or biomechanical patterns [20]. In keeping with the literature, our series has not revealed any consistent histologic ligamentous changes that were found to be contributory to idiopathic CTS in both younger and older patients. The histology was reported as normal grading in 73.5% of the specimens. Inflammation (3.0%), mucoid change (17.5%), and amyloid deposits, except in cases of familial amyloidosis (6.0%), were all found to be mild and considered non-specific [21].
The use of PSR to differentiate between the different collagen types in tissue was originally described by Junqueira, et al. [22]. Observations show that PSR stains pure collagen strongly, without staining other proteoglycans, with a simple, reliable, and inexpensive technique. Collagen fibers show up in bright colors contrasted against a black background. Type I collagen, formed from thick fibers composed of closely packed fibrils, exhibits an intense red or yellow birefringence. Type III collagen forms thinner fibers, of loosely disposed fibrils with weak green birefringence. Significantly greater amounts of type I collagen fibers were found in men compared to women, and significant differences in the quantity of type III collagen were found between women and men. We found a reduced renewal rate for collagen type I and an increased rate for type III, with increasing age in both genders. Three potential explanations for these findings can be considered: (i) Both the fibroblast numbers and the rate of collagen formation decreased with age; (ii) Rate of collagen production decreased whilst the fibroblast numbers remained constant; or (iii) The number of fibroblasts decreased but the rate of collagen formation was stable. Regardless of the mechanism, these observations allow us to conclude that the formation of collagen fibers decreased with increasing age.
We found that collagen I levels decreased almost linearly with increasing age in both sexes. Published literature reporting reduced collagen expression and synthesis as a function of aging fibroblasts [23], corroborates our findings. Our data suggests that alterations in collagen I expression may contribute to age-dependent degeneration of TCL. The immunoblotting results were corroborated by the PSR staining-polarization microscopy data for the distribution of collagen types I and III in TCL. Collagen type VI is a primary extracellular matrix component in vascular tissues, responsible for von Willebrand factor dependent platelet adhesion/aggregation [24]. Dysregulation of collagen VI synthesis may be an important contributing factor to the disordered matrix protein deposition resulting in tissue fibrosis [25]. An upregulation of Collagen VI was observed in this patient group reported in our work, Figure 4.
The strength of this study lies in the expression of collagen sub-types in the transverse carpal ligament. This is the first study to assess the age and gender-related alternations to the distribution of collagen types in TCL. Significant study findings include the distribution of collagen types I and III, and the distribution and upregulation of collagen type VI. We also noted some differences in collagen morphology in patients with CTS in women as compared to men. Moreover, our results clearly present evidence for an age-related decline of collagen I expression in both men and women.
We conclude that in patients with idiopathic Carpal tunnel syndrome, the transverse carpal ligament often presents normal histology with no typical or consistent changes with which idiopathic CTS can be associated. We identified that collagen types I, II, III, V, VI, and X in the TCL of individuals with CTS. Collagen types I and III are widely distributed in collagen bundles. These bundles are larger in female patients with CTS than in males. Decreased collagen type I in TCL is the first example which directly suggests the possible importance of alterations in collagen expression with the aging process. Further accumulation of more histological and biochemical data would eventually clarify the intrinsic causes of age-dependent degenerative alterations of collagen in TCL. Collagen type VI is found throughout the TCL of all CTS patients. Future studies should explore additional biomolecules using proteomics to help understand the pathogenesis, and potentially identify targets for prevention of CTS. Our present results support the view that collagen distribution is specifically associated with aging and gender in TCL.
None to report.
None.