Work done for the purpose of analysis of the dependence of the pace of age-related decline in speed of cerebral blood flow and functional status of the musculoskeletal system of different groups of patients.
Investigated the blood flow velocity (FV) in middle cerebral arteries (MCA) during the function of the muscle samples from subjects of different age 12 groups (214 people): Healthy individuals, patients with fractures of the extremities and congenital shortening of the tibia in the treatment by Ilizarov.
The lower values of FV and a rate of increase age of decline is the consequence of disturbance in the health of patients and worsens the prognosis of the duration of their life. At the same time, age-related decline of FV in the MCA is a necessary condition for the preservation of cerebral autoregulation.
The output of scope change SC AGR in functional tests within the normal range (25%) is accompanied by decreased capacity of patients and slowing down the process of reparative regeneration.
Cerebral blood flow, Middle cerebral artery, Age, Pathology of the musculoskeletal system
It is known that with increasing age in people against the background of a steady decline in kinesophilia, there is a decrease in the thickness of the cortical layer of the brain and the speed of cerebral blood flow while maintaining [1-4]. In studies conducted in nursing homes, it was shown that the highest rate of decrease in cerebral blood flow rate is also observed in patients with pathologies of the musculoskeletal system [5].
In children, with increasing age, the maximum allowable values of the operative lengthening of the limbs lagging in growth decrease, the duration of the fixation of bone fragments decreases [4,5]. However, in older patients, the remaining reserves of reparative regeneration are sufficient to heal the damaged bones of the limbs [6]. The aim of the work was to analyze the relationship of the rate of age-related decline in cerebral blood flow and the duration of active life in different groups of patients.
The study of cerebral blood flow was performed in 45 healthy volunteers of different ages (from 5 to 70 years) in the control group. In addition, various groups of patients aged 15 to 67 years with congenital and acquired diseases of the lower extremities (see Table 1) were examined, as well as 91 patients aged 21 to 80 years with closed fractures of the leg or shoulder bones under the conditions of treatment Ilizarova.
Table 1: The coefficients of the equation A * X + B of the age dynamics of the BFV according to the MCA counter parties. View Table 1
Blood flow velocity (BFV) in the arteries of the extremities and the middle cerebral arteries (MCA) was determined using the Angiodin 2UK ultrasound unit (Russia) with sensors with a carrier frequency of 2 and 8 MHz, respectively. The registration of BFV by MCA from each side was repeated with a functional test with the compressing of an elastic expander with a brush of the right and left hand. At the same time, the maximum range of changes in indicators from baseline values was determined.
Self-assessment of the physical and mental state of patients was performed using the SF-36 test. The test card put into a computer contains 36 alternative questions that, based on 8 modules, allow us to judge the quality of life by integrating physical data (efficiency, ability to self-care, well-being, pain) and mental state (vitality, mood, emotional state, social activity) of each subject. The indicators measured in the modules contain from 0 to 100 points.
Statistical processing of research results was carried out using the data analysis package "Microsoft Exell-2010. The tables show the mean values of the indices and the mean square error (M ± m). To assess the statistical significance of the differences in the results in the case of the analysis of two independent samples, Student's t-test was used.
After conducting surveys of healthy people of different ages and different groups of patients, we constructed the linear regression equations for the age-related changes in the SC index for the MCA. The size of the SC in healthy children is 120 ± 4.5 cm/s, which is statistically significant 27% (p ≤ 0.001) higher than, for example, in patients with congenital shortening of limbs. If you follow the rate of age-related decline in IC, you can build a graph and determine when the rate will drop by 40%. Such a decrease in the norm occurs when the regional value of the average life expectancy of the population is reached and indicates the exhaustion of the reserves of functional adaptation of the centers of the nervous system.
In the different groups surveyed, as the SC increased in age, the MCA became smaller. When constructing graphs of linear regression equations, the threshold age-related decrease in the index is determined (Figure 1). Normally, the regional life expectancy of people in the Kurgan Region, as well as patients with fractures of the bones of the leg, vertebral artery syndrome, and osteoarthrosis is 67 years. In patients with congenital shortening of one of the limbs - 52 years. Knowing the rate of IC on the SMA and the age of the patient, it is possible to assess the effect of pathology on the expected life expectancy.
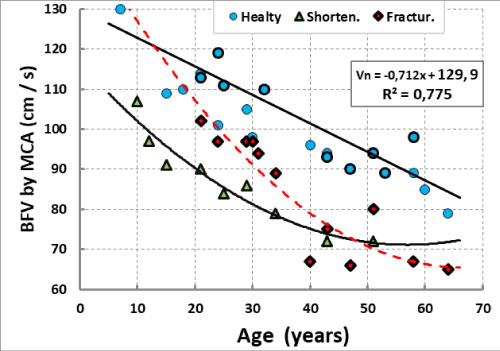 Figure 1: The age dynamics of BFV on MCA in healthy, in patients with congenital shortening of the limb and in patients with fractures.
View Figure 1
Figure 1: The age dynamics of BFV on MCA in healthy, in patients with congenital shortening of the limb and in patients with fractures.
View Figure 1
In the subjects of the control group, the rate of SC decline was 0.71 cm/s for each year of life. Taking this level of IC reduction as a basis, it turned out to be possible to calculate after how many years of life it will be achieved in patients of other groups, in particular with congenital pathology of the musculoskeletal system (Table 1).
These calculations are indicative, as the individual indicator of life expectancy depends on a number of other biological and social and medical factors. In addition, we took as a guideline not the maximum possible lifespan, but the value of 80 years. H was taken into account and the degenerate nature of the sample of observations after reaching 60 years. For us, it was important to show that under extreme conditions of bone injury and operative lengthening of an extremity, the rate of age-related decline in the SC index began to exceed 1 cm/s per year, and the estimated indicator of the likely life expectancy decreased significantly.
The age-related decline of the IC in the arteries was accompanied by the preservation of the magnitude of the magnitude (magnitude) of changes in the SC, indicating the state of autoregulation of the cerebral blood flow [7-10], since. the increase in blood flow velocity during the loading tests was the greater, the smaller the absolute values of the BFV were: ΔV = 0.174-0.0018 × V; r = -0.773. Consequently, despite the age-related decrease in the rate of cerebral arterial inflow, the reactivity of the indicators of cerebral blood flow autoregulation during muscle functional tests should not be disrupted.
The age of reaching the critical level of reduction of the SC index for SMA in the period of treatment of patients is not a true indicator of life expectancy, since the period of treatment is temporary. Moreover, in many cases, the linear nature of the decline in the indicator when approaching critical values becomes exponential. At initially low values of values in children, it is necessary to focus not on absolute values, but on the rate of their change, which is lower in patients.
The study of patients with different localization of a bone fracture allowed a comparative analysis of the effect of limb injury on the magnitude of IC growth along the MCA of the contralateral side of the brain (Figure 2). It turned out that the greater the mass of tissues of the damaged organ, the greater the reaction of the brain centers to the damage.
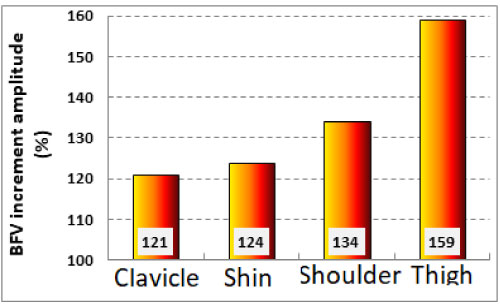 Figure 2: The maximum increase in the relative IC on the MCA of the contralateral side of the brain in the treatment of patients with injuries of different localization.
View Figure 2
Figure 2: The maximum increase in the relative IC on the MCA of the contralateral side of the brain in the treatment of patients with injuries of different localization.
View Figure 2
Disorders of autoregulation of cerebral blood flow can be identified with an increase in the range of SC changes along the SMA when performing functional tests with the work of the wrist grasp muscles. The magnitude of this range is determined mainly by the degree of decline in the state of rest and should not go beyond 17-25%. If it goes beyond the set limits, this indicates a violation of the function of the central nervous system. With such a violation, the process of reparative bone regeneration slows down. A change in the scope of the range of changes beyond the permissible limits was observed, for example, in the treatment of fractures of the shin bones in patients over 50 years of age (Figure 3). In patients with closed helical and comminuted fractures of the bones of the leg in the conditions of treatment according to Ilizarov, the fixation periods increased, respectively, by 2 and 3.3 days for every 10 years of life [10].
 Figure 3: The age dynamics of IC on SMA and the range of changes in the index in patients with fractures of the bones of the leg in the process of treatment.
View Figure 3
Figure 3: The age dynamics of IC on SMA and the range of changes in the index in patients with fractures of the bones of the leg in the process of treatment.
View Figure 3
The age-related decline of BFV in the MCA is compensatory, since it ensures the preservation of the magnitude of changes in the cerebral blood flow during functional muscle samples (Figure 4).
 Figure 4: Dependence of the increase in the SC index for the MCA when tested with the work of the arm muscles from the initial value of the relative IC for the MCA of the contralateral side of the brain.
View Figure 4
Figure 4: Dependence of the increase in the SC index for the MCA when tested with the work of the arm muscles from the initial value of the relative IC for the MCA of the contralateral side of the brain.
View Figure 4
The heavier the pathology, for example, the greater the shortening of the affected limb, the greater the decrease in the SC in the SMA when performing a muscle function test (Figure 5). Even faster with increasing age, the SC scores for SMA decrease with operative lengthening of the affected lower leg.
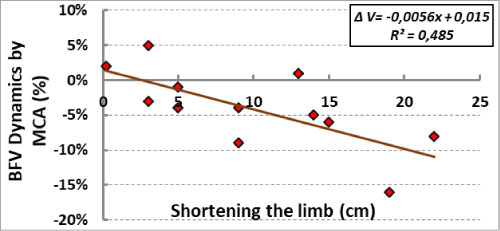 Figure 5: The dependence of the IC on the MCA of the contralateral side when conducting a muscle test on the magnitude of the shortening of the limb.
View Figure 5
Figure 5: The dependence of the IC on the MCA of the contralateral side when conducting a muscle test on the magnitude of the shortening of the limb.
View Figure 5
If in the treatment of patients with acquired limb shortening, the ratio of SC values by SMA on the contralateral and ipsilateral sides of the brain increases to 141%, then with congenital abnormalities it decreases to 74% (Figure 6).
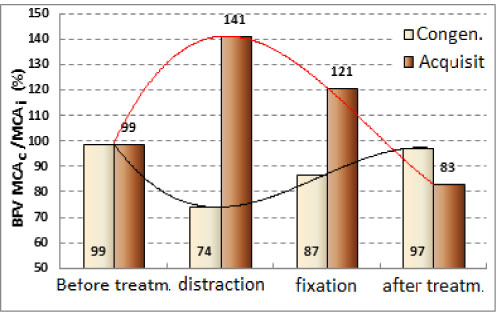 Figure 6: Dynamics of the ratio of BFV in MCA on the ipsilateral and contralateral sides of the brain during operative lengthening of the tibia in patients with congenital and acquired shortenings of the limbs.
View Figure 6
Figure 6: Dynamics of the ratio of BFV in MCA on the ipsilateral and contralateral sides of the brain during operative lengthening of the tibia in patients with congenital and acquired shortenings of the limbs.
View Figure 6
The range of BFV changes in the MCA when performing tests with the work of the wrist gripper muscles during the treatment of patients with congenital limb pathology was increased compared with the values of the change in healthy ones, since the muscle work was accompanied by a more pronounced decrease in cerebral blood flow rate. As a result, the magnitude of the magnitude of changes was normalized only in patients over the age of 20 years (Figure 7).
 Figure 7: Age-related dynamics of the magnitude of BFV changes along the MCA in a functional test in patients with congenital pathology of the extremities.
View Figure 7
Figure 7: Age-related dynamics of the magnitude of BFV changes along the MCA in a functional test in patients with congenital pathology of the extremities.
View Figure 7
A similar process of normalization of the magnitude indicator was revealed in patients after the equalization of the length of the limbs. In the process of distraction, the range increased to 33%, mainly due to the negative effect of muscle work on the SC index in the AGR. By the end of the distraction, the magnitude of the scale has stabilized at a level of up to 22% ± 1.6 (Figure 8), which is also characteristic of healthy people.
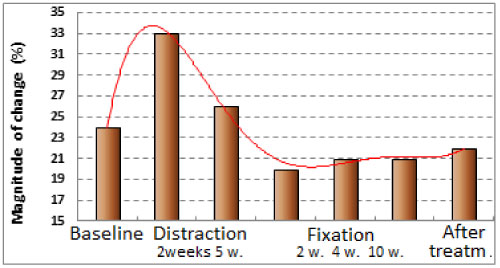 Figure 8: The dynamics of the scope of BFV changes in the MCA in the process of surgical treatment of patients with congenital shortening of the limb.
View Figure 8
Figure 8: The dynamics of the scope of BFV changes in the MCA in the process of surgical treatment of patients with congenital shortening of the limb.
View Figure 8
The performance of patients in the period of distraction was impaired. Preserving the variability of the BFV changes within the normal range is a necessary condition for the preservation of the normal functioning of the centers of the brain. During the SF-36 test, it was found that the greater the limiting effect of pain on the daily activities of patients during the period of distraction (P, points), the lower the BFV value on the MCA of the contralateral side was: Vc = 0.52 * P + 69; (r = 0.425). The smaller was the value of the relative BFV, the lower the capacity of patients (Figure 9). Too high a relative IC of the contralateral side of the brain (more than 120%) is also unfavorable for maintaining the capacity of patients.
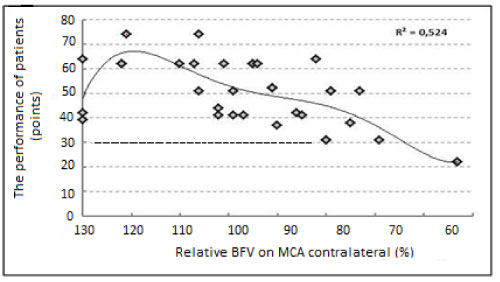 Figure 9: The relationship between the health of patients and the relative BFV on the MCA of the contralateral side of the brain during operative lengthening of the limb.
View Figure 9
Figure 9: The relationship between the health of patients and the relative BFV on the MCA of the contralateral side of the brain during operative lengthening of the limb.
View Figure 9
1. The age-related decline of BFV in the MCA is a necessary condition for the preservation of the autoregulation of cerebral blood flow.
2. The relatively low absolute indicators of BFV for MCA and the increased rate of their age-related decline are the result of impaired patient health and worsen the prognosis for life expectancy.
3. The output of the scope of BFV changes in the MCA beyond the norm in the process of surgical treatment of patients is accompanied by a decrease in their capacity and slowing down the process of reparative regeneration.