Background: The COVID-19 pandemic has adversely affected health care services worldwide, including India. A test battery approach is required to effectively diagnose various audiological conditions, and utilizing a test battery was challenging during COVID-19. The audiological practice has been modified during COVID 19 and the test is decided based on the client's urgent need. The present case study highlights the importance of the test battery approach for the effective diagnosis of Auditory Neuropathy Spectrum Disorder (ANSD) during the Corona Pandemic.
The case: A sixteen-year-old male reported reduced hearing sensitivity in both ears from six months, with sudden onset and acquired in nature. The diagnosis of the client was made after three evaluations as ANSD.
Conclusion: It is concluded that depending upon the population, it is necessary to add in all the tests for audiological evaluation so that there is no delay in the diagnosis.
Test battery, Differential diagnosis, ANSD, Pandemic, Case report
Auditory Neuropathy Spectrum Disorder (ANSD) is a form of sensorineural hearing impairment reported to cause impaired neural conduction with preserved cochlear outer hair cells [1]. It is characterized by reduced hearing sensitivity with fluctuating loss, difficulty understanding speech in noise, answering inappropriately, or limited response to a conversational level [2]. ANSD is a complex hearing disorder requiring methodic identification and a test battery approach to achieve a proper diagnosis. A test battery approach includes various diagnostic tests during the initial evaluation, including pure-tone audiometry, acoustic reflex testing, imaging, and auditory brainstem response testing to differentially diagnose. For the effective diagnosis of ANSD, the test battery should include an effective case history, pure tone audiometry, acoustic reflex testing, otoacoustic emissions, auditory brainstem responses, and neurological evaluation [3].
The COVID-19 pandemic has adversely affected health care services worldwide, including India. Some of the children's health services were interrupted to control the infection and protect the vulnerable population from getting affected by the COVID-19. To effectively diagnose various audiological conditions, a test battery approach is required. Performing the audiological evaluations and utilizing the test battery was a challenging task during COVID-19. Low- and no-touch services are necessary for audiology patients - who are typically at the highest risk for COVID-19 morbidity and mortality due to their age - to access medical care [4]. The audiological practice has been modified during COVID 19 and the test is decided based on the client's urgent need [5]. The present case study highlights the importance of the test battery approach for diagnosing ANSD during the Corona Pandemic.
A sixteen-year-old male reported to the Department of Audiology on 07/12/2020 with the complaint of reduced hearing sensitivity in both ears from six months, with sudden onset and acquired in nature. The routine audiological evaluations included pure tone audiometry, and immittance evaluations were performed on the client. A calibrated two-channel diagnostic audiometer, MA-53 (MAICO Diagnostics, Germany), equipped with TDH39 headphones, was used to perform pure tone audiometry. Pure tone audiometry revealed a minimal hearing loss in the right ear (Pure tone average, PTA: 20 dB) and normal hearing sensitivity in the left ear (PTA: 7.5 dB) (Figure 1). Immittance evaluation was done using GSI- TympStar (Grason-Stadler, MN, USA) to assess tympanometry and acoustic reflex. Tympanometry indicated an 'A' type tympanogram in both ears with ipsilateral reflexes present in the right and left ear. Though the client came with the complaint of reduced hearing sensitivity in both ears, speech audiometry, otoacoustic emission (OAEs), and auditory brainstem response (ABR) could not be done due to the pandemic.
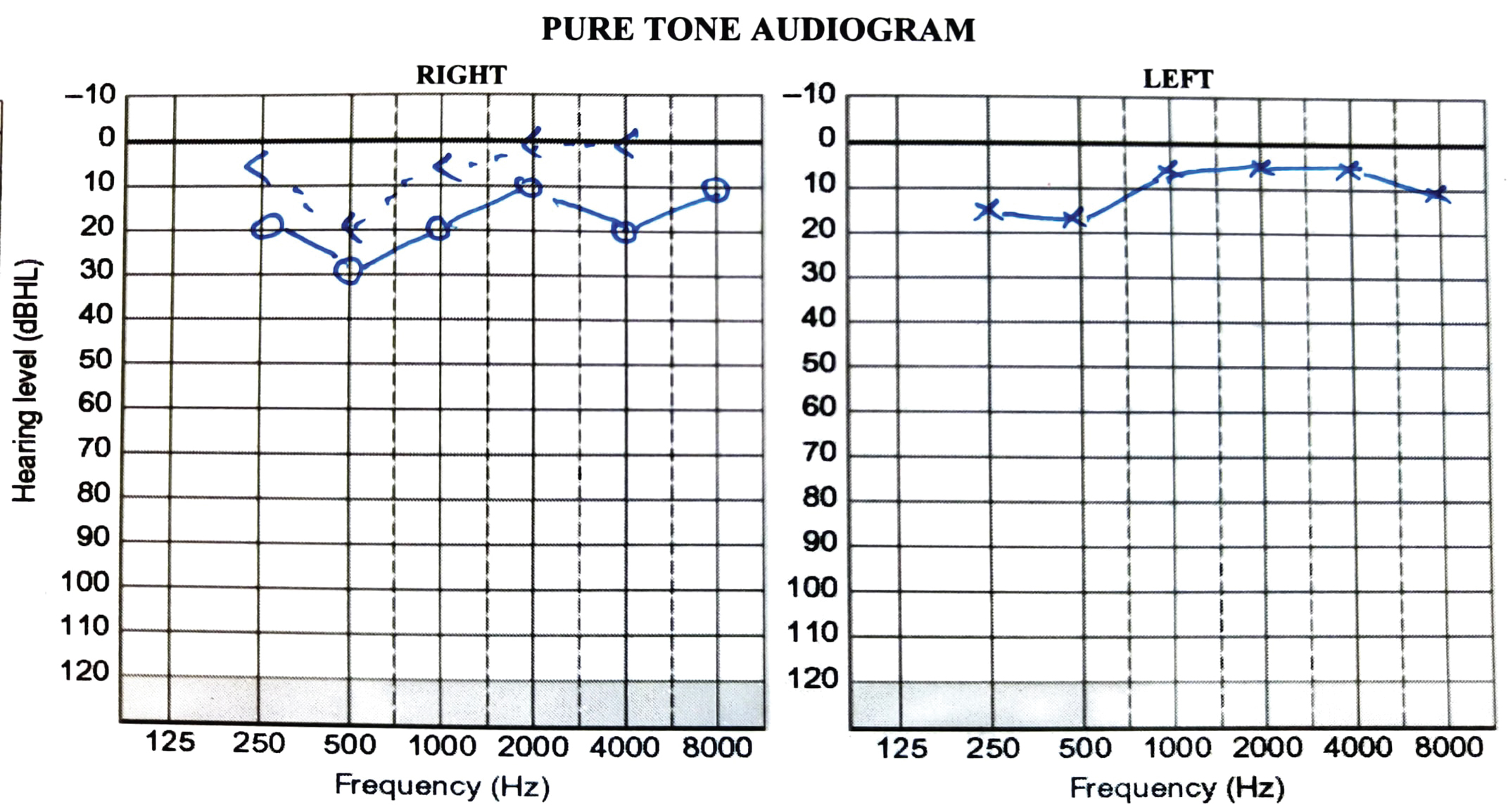 Figure 1: Pure tone audiogram of the client on the first visit.
View Figure 1
Figure 1: Pure tone audiogram of the client on the first visit.
View Figure 1
The client again reported to the Department of Audiology on 28/10/2021 with the same complaint of reduced hearing in both ears, especially in a noisy environment. During the second evaluation, pure tone audiometry, immittance evaluation, and OAE was done. Pure tone audiometry revealed a profound loss in both the ears (PTA in Right: 93.75 dB and left: 97.5 dB) (Figure 2). Immittance evaluation showed an 'A' type tympanogram with reflexes absent in both ears. A calibrated ILOV6 OAE analyzer (Otodynamics Ltd) was used for recording distortion product (DP) OAEs. DPOAEs were present in both ears. There was no correlation between the tests and the client was sent for auditory brainstem responses (ABR) for threshold estimation.
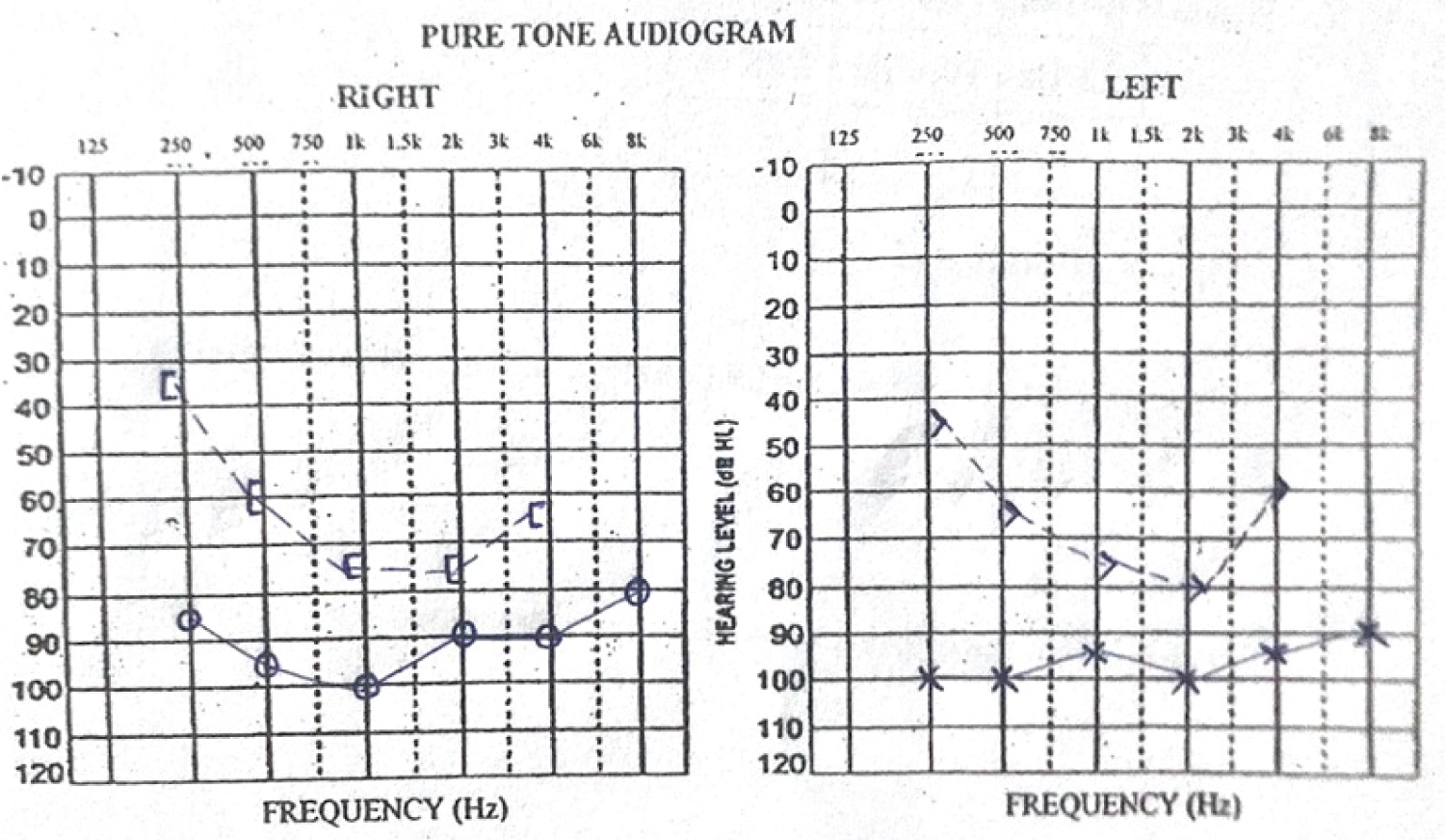 Figure 2: Pure tone audiogram of the client on the second visit.
View Figure 2
Figure 2: Pure tone audiogram of the client on the second visit.
View Figure 2
The third evaluation was done on 10/11/21. A calibrated Biologic Navigation Pro system (version 7.0.0) fitted with an ER-3A insert receiver was used for ABR recording. The ABR was done at 90 dBnHL with an 11.1/s repetition rate using click stimulus, and the results showed no identifiable peak in both ears. The cochlear microphonics was present in both ears till 3.5 ms (Figure 3). Further, all the other tests were repeated on the client. The pure tone audiometry revealed a moderately severe loss in the right ear (Pure tone average, PTA: 57.5 dB) and moderate loss in the left ear (PTA: 52.5 dB). Immittance evaluation showed an 'A' type tympanogram with reflexes absent in both ears. Distortion Product OAEs were present in both ears. Speech audiometry results showed speech recognition thresholds (SRT) of 30 dB in the right ear and 20 dB in the left ear for questions. Speech identification scores (SIS) in quiet were 75% in the right ear and 85% in the left ear. Further, SIS was done in the presence of noise at 0 dB SNR, which was 0% in the right ear and 25% in the left ear (Figure 4). Table 1 shows the summary of tests performed during each visit.
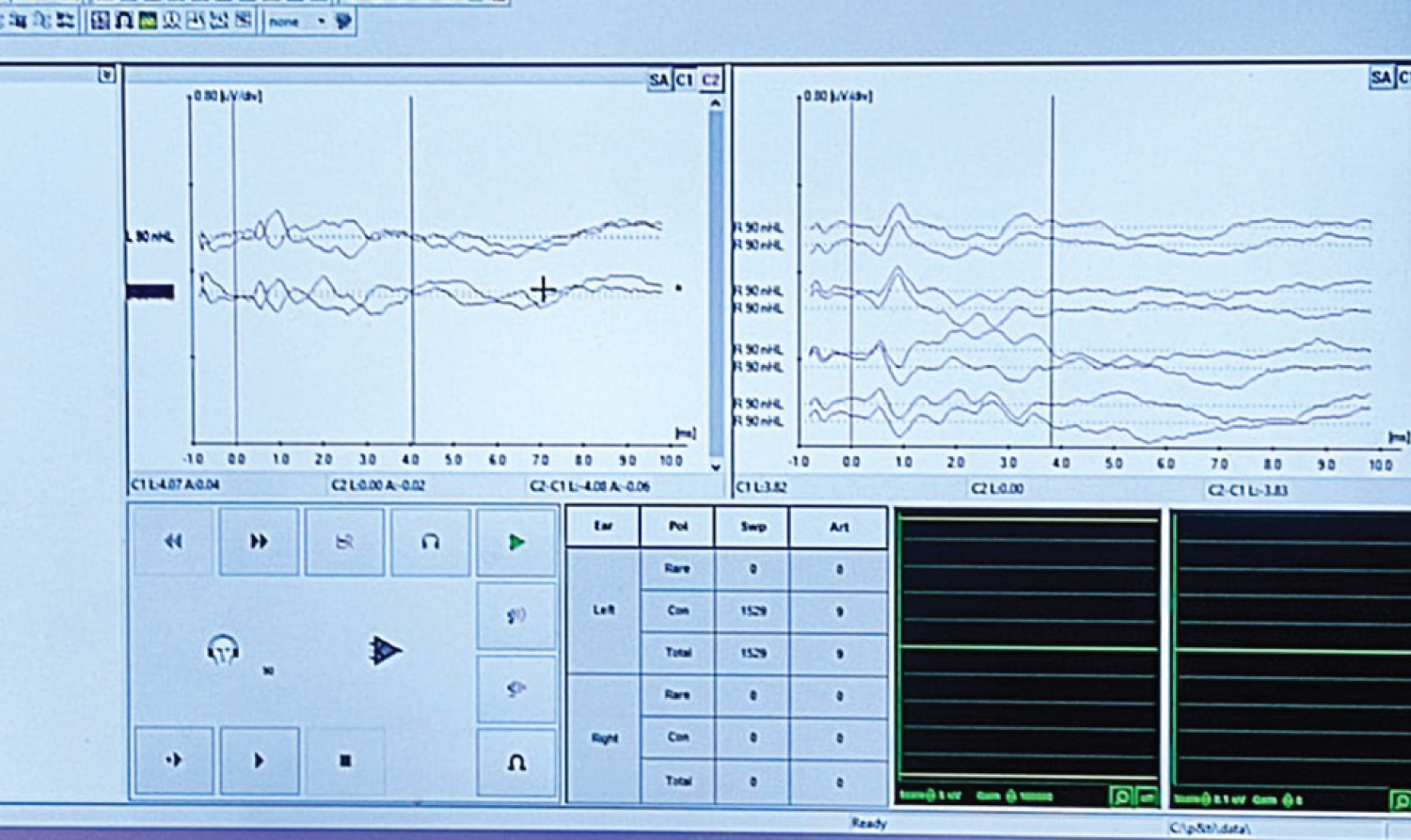 Figure 3: Auditory brainstem responses of the client.
View Figure 3
Figure 3: Auditory brainstem responses of the client.
View Figure 3
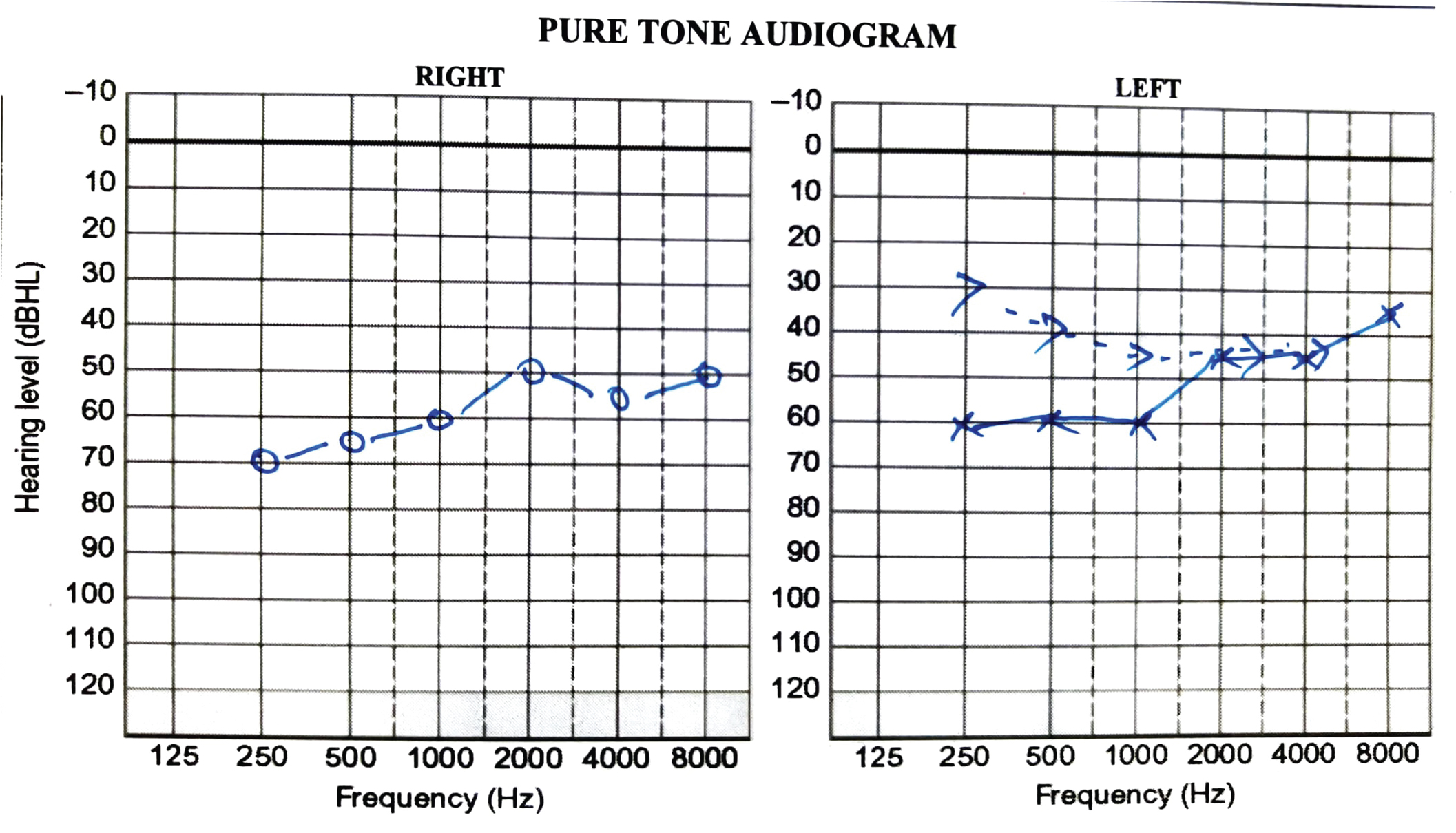 Figure 4: Pure tone audiogram of the client on the third visit.
View Figure 4
Figure 4: Pure tone audiogram of the client on the third visit.
View Figure 4
Table 1: Summary of the audiological tests performed during each visit. View Table 1
The present case was diagnosed with a moderate to moderately severe hearing loss with ANSD. The diagnosis was confirmed based on the audiological findings of fluctuation hearing loss across three evaluations, absent acoustic reflexes, presence of OAEs, presence of cochlear microphonics, and absent ABR. The above characteristics are typical in clients with ANSD [3]. It can be noted from the present case that the diagnosis of ANSD could be made during the third evaluation, as the whole test battery could not be done in the first two evaluations due to the pandemic. This is also supported by various studies wherein it is reported that the diagnosis of ANSD requires a battery of tests [1,3]. Thus the present case highlights the importance of the test battery approach in audiological assessment, especially during a pandemic for the effective diagnosis. Therefore, depending upon the population, it is necessary to add all the audiological evaluation tests to avoid delay in the diagnosis.
A test battery approach is required, especially in diagnosing atypical cases. Due to the pandemic, usage of the entire test battery has been difficult. But depending upon the population, it is necessary to add in so that there is no delay in the diagnosis.
Authors declare no conflict of interest.
Written informed consent was taken from the participant for their willingness to participate in the study.
Ayishath Ruwaidha PV, Aswathy R Nair, Apoorva Gogiyan, Ansila Raslan: Data collection, preparation of manuscript. Vikas MD, Chandni Jain: Reviewing the literature, overviewing the data, preparation of manuscript.