Celiac Disease is a malabsorptive disorder of the small intestine that often presents with diarrhea as the most common symptom. Confirmatory diagnostic testing includes endoscopy, serologic testing, and biopsy of the small intestine. These two cases of Celiac Disease are unique because two women, mid-thirties and medically obese, presented with non-classic symptoms of CD. Patient A complained of recurrent upper abdominal discomfort and pain, while Patient B complained of persistent daily symptoms of nausea. Focal intraepithelial lymphocytes were present on small bowel biopsy for both patients. Villous atrophy consistent with Marsh Type 1 and Type 3 classification was also present on small bowel biopsy, for Patient A and Patient B, respectively. Both patients tested negative for Helicobacter pylori based on biopsy not through serology, yet the pattern of inflammation on gastric biopsy showed the possibility of H. pylori gastritis for Patient A.
Celiac disease, Gastroenterology, Malabsorptive disorders, Auto immune disease, Villous atrophy, Intraepithelial lymphocytes, Inflammation, Gastrointestinal disorders
CD: Celiac Disease; Anti-tTG2: Tissue Transglutaminase 2; DGP: Deamidated Gliadin Peptide; EGD: Esophagoduodenoscopy; PMH: Past Medical History; NSAIDs: Non steroidal Anti-inflammatory Drugs; Ab: Antibody; IELs: Intraepithelial Lymphocytes; IDA: Iron Deficiency Anemia
Celiac disease (CD) is a chronic, immune-mediated malabsorption disorder of the small intestine caused by exposure to dietary gluten proteins such as wheat, barley, and rye that can occur at any age [1,2]. Specific auto antibodies against tissue transglutaminase 2 (anti-tTG2), endomysium, and /or deamidated gliadin peptide (DGP) characterize this disease, along with microscopic evidence of villous atrophy of the small bowel seen on biopsy upon completion of esophagoduodenoscopy (EGD) [1]. CD manifests systemically and commonly presents with a wide variety of symptoms, such as diarrhea, steatorrhea, abdominal distension, impaired growth, muscle wasting, lethargy, irritability, and weight loss [2,3]. CD occurs more often in women than in men and presents with diarrhea as the predominant classic symptom [4]. Risk factors for CD include white race and a positive family history of CD [5]. Unfortunately, the only proven treatment of CD today is strict adherence to a gluten-free diet [6].
Patient A is a 34-year-old female that presented with recurrent upper abdominal discomfort and pain that began about one month previously. She also reported recent episodes of nocturnal awakening with abdominal discomfort and bloating. She also complains of intermittent heartburn, for which she uses Tums on a daily basis, and constipation. She has taken Dulcolax to alleviate the constipation symptoms, but this resulted in abdominal cramping and diarrhea. She was recently treated for a chlamydial infection with antibiotics and explained that her gastrointestinal symptoms seem to improve after treatment. She denied any rectal bleeding, weight loss, nausea, or vomiting, and recently had unremarkable blood work. Past medical history (PMH) consisted of gallstones, asthma, anxiety, and depression. Physical exam shows no relevant clinical findings, including no abdominal tenderness, guarding, or distension.
An EGD was performed one month after the initial visit. A Forrest 3 classification acute gastric ulcer without hemorrhage or perforation was identified in the antrum. Small bowel biopsy revealed focal intraepithelial lymphocytes (IELs) and villous architecture that was essentially preserved, however, Marsh Type 1 villous changes were present. Gastric biopsy revealed chronic active gastritis and no organisms consistent with Helicobacter pylori were identified by immune histochemistry, although the pattern of inflammation displayed the possibility of H. pylori gastritis. Gastric biopsy was negative for intestinal metaplasia, ulcer, or malignancy in sampled tissue (Figure 1).
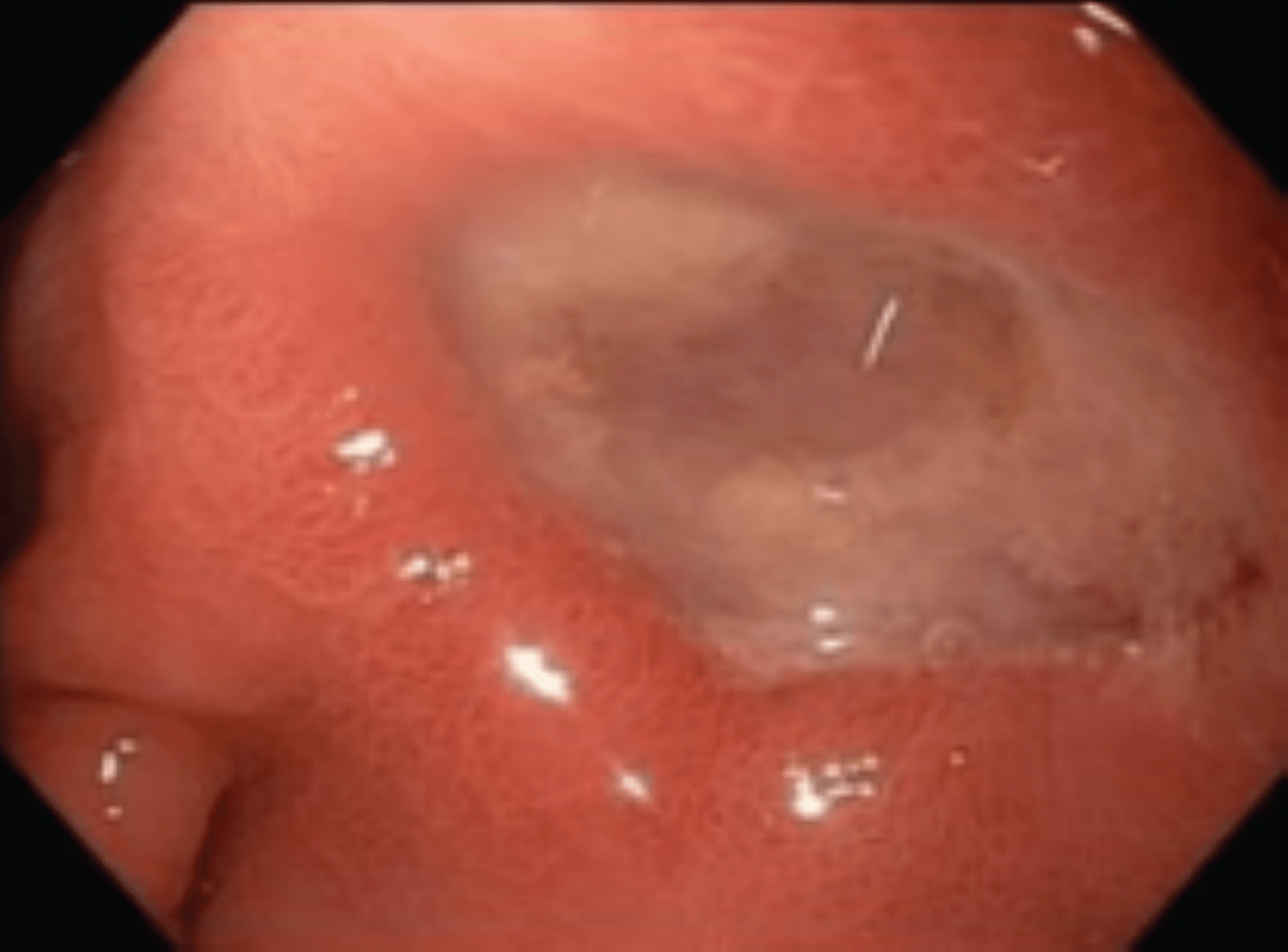 Figure 1: An acute gastric ulcer, Forrest 3 classification and measuring 3cm were discovered in the antrum of Patient A's stomach during EGD.
View Figure 1
Figure 1: An acute gastric ulcer, Forrest 3 classification and measuring 3cm were discovered in the antrum of Patient A's stomach during EGD.
View Figure 1
Approximately two weeks later, Patient A returned to the clinic to discuss the EGD and biopsy results. A repeat EGD in three months was recommended, to check on the status of the gastric ulcer, and the patient was instructed to take one 40 mg tablet of pantoprazole by mouth twice daily for two weeks, then once daily after the two week period. Urease breath test was discussed and planned as well, to confirm the presence of Helicobacter pylori. She was also instructed to avoid use of nonsteroidal anti-inflammatory drugs (NSAIDs) and to use Tylenol as needed. Comprehensive labs for CD were ordered, and the patient was instructed to follow gluten-free diet upon completion of these labs, to determine if her symptoms would subside from gluten-free diet (Table 1).
Table 1: Celiac disease laboratory analysis results. View Table 1
Three months later, she reported to the clinic for follow-up and to review lab findings, which showed positive findings for CD. She stated that she had been doing fairly well, although she was still struggling with occasional episodes of bloating and gas. She explained that she had been trying her best to be compliant with a gluten-free diet, although it was difficult to follow sometimes. An H. pylori breath test was scheduled to rule out H. pylori infection, and she was instructed to continue compliance with a gluten-free diet indefinitely. A follow-up in 6-9 months was recommended to review repeat celiac serology and assess her response to a gluten-free diet.
Patient A did not complete H. pylori testing and has not returned to the clinic yet. She had previously expressed that financial barriers existed and may prevent her from returning for more tests. It would be beneficial to perform a repeat EGD and rebiopsy to recheck for healing of the gastric ulcer and to determine if the possible H. pylori infection is present, or if it was eradicated. H. pylori testings are recommended to determine if the IELs were a result of the H. pylori, or if they were the result of another cause, such as NSAIDs or alcohol abuse.
Patient B is a 38-year-old female that presented with persistent daily symptoms of nausea ongoing for the last 4 to 5 months. She reported a lack of appetite and a weight loss of approximately 40 pounds because of the dyspepsia. The symptoms initially began as upper abdominal discomfort initially, although they have disappeared in the last two weeks prior to the initial visit. She denies any history of chronic NSAID use, hematemesis, melena, hematochezia, nocturnal symptoms, postnasal drip, vertigo, or marijuana use. She was prescribed Zofran, which made her symptoms worse, and she took over-the-counter proton pump inhibitors, which did not provide much relief. She has a PMH of prediabetes, hypothyroidism, and valvular heart disease. A recent computed tomography scan of the abdomen and pelvis was unremarkable, and a recent ultrasound of the bladder showed no gallstones, although fatty liver was noted. HIDA scan showed normal ejection fraction and blood work showed no abnormalities, except a mildly elevated AST of 41. The physical exam offered no relevant clinical findings, including no epigastric tenderness, abdominal guarding, or distension.
An EGD was performed approximately one month after the initial visit, revealing a single 5 mm sessile polyp in the gastric fundus with no indication of recent bleeding. Small bowel biopsy showed small intestinal mucosa with villous blunting, increased numbers of IELs and Marsh Type 3 villous blunting. Gastric biopsy revealed benign gastric mucosa with focal mild nonspecific chronic inflammation, which was not classic for H. pylori. Patient B returned to the clinic two weeks after the EGD was performed to discuss findings, reporting that the nausea present at her initial visit was still persistent. She was instructed to stop taking her daily proton pump inhibitor and begin a gluten-free diet, due to increased suspicion of CD as evidenced in EGD and biopsy results. A CD comprehensive panel was ordered, and a diagnosis of CD was confirmed (Table 1).
She returned to the clinic approximately two months later and reported feeling much better. Her nausea had significantly improved and she noted a weight loss of about 14 pounds. She was recommended to follow up in 3 months to check labs again.
It is essential that clinicians are aware of atypical and extraintestinal symptoms of CD to decrease the time that symptoms start to the time of diagnosis for patients. The Oslo classification for CD was established in 2011, which identified and defined various clinical presentations of CD as classic, non-classic, sub-clinical, potential, and refractory. Classical CD was defined as, "CD presenting with signs and symptoms of malabsorption. Diarrhea, steatorrhea, weight loss or growth failure is required" [3]. Intestinal/extraintestinal better represents the main clinical phenotypes of CD, in place of classic and non-classic [6]. Patient A presented with non-classic symptoms of CD: upper abdominal discomfort, heartburn, and constipation. While patient B presented with both non-classic and classic symptoms of CD, respectively: Nausea and weight loss. CD should not be ruled out of any clinician's differential diagnosis if classic symptoms are absent; patients must be viewed holistically, and all imaging, labs, and medical history must be carefully considered as potential diagnostic clues.
Pathology plays an important role in the diagnosis of CD, as tissue biopsy obtained at endoscopy serves as the gold standard for the diagnosis of CD. Indications of CD on tissue biopsy include displaying partial to total villous atrophy, increased inflammatory cells in the lamina propria, crypt hyperplasia, IEL with or without enterocyte damage [4,7]. Increased numbers of IELs were present on small bowel biopsy in Patient A and Patient B, which is clinically important because a clear association between the presence of IELs and CD has been established [4,7]. The presence of IELs may aid in the diagnosis of CD, and it is important to note that IELs may also be present in other conditions or exposures as well, such as H. pylori, NSAIDs, alcohol, graft vs. host disease, Crohn's disease, ulcerative colitis, and more [7]. Pathologists should always note on pathology reports that the presence of IELs may indicate several potential differential diagnoses including CD, as this may assist physicians in diagnosing CD faster, and educate clinicians that are not familiar with the clinical importance of IELs. The Marsh classification established criteria to distinguish small intestinal mucosal changes caused by CD, consisting of Type 1 (infiltrative), Type 2 (hyperplastic), and Type 3 (destructive) [8]. Patient A displayed evidence of Marsh Type 1 villous changes, while Patient B displayed Marsh Type 3 villous blunting, further corroborating a diagnosis of CD. Other intriguing pathological findings include evidence of inflammation consistent with H. pylori for Patient A, despite both patients testing negative for H. pylori. As an intestinal malabsorptive disorder, CD impairs iron absorption on its own, and H. pylori gastritis may work in conjunction with CD to cause iron deficiency anemia (IDA) [9]. Therefore, it is crucial for clinicians to remember this relationship between H. pylori, CD, and IDA, to consider performing upper and lower GI investigations in males and postmenopausal women with confirmed IDA, and to test for IDA in patients with CD or H. pylori, as it is the standard of care [10].
CD is associated with autoimmune disorders such as type 1 diabetes, thyroiditis, psoriasis, hepatitis, cardiomyopathy, and neurologic problems [2,4]. Both patients had a PMH of at least two autoimmune disorders or inflammatory processes: Patient B presented with a PMH of prediabetes, hypothyroidism, and valvular heart disease and Patient A presented with a past medical history of depression and anxiety, and interestingly, a Forrest 3 classification acute gastric ulcer found on EGD. Patients A and B were obese with BMI's of 33 and 41, respectively, and it is well known that obesity is associated with increased inflammation in the body and the release of inflammatory mediators such as interleukin-6 and C-reactive protein [11]. Patient A's PMH of depression should not be overlooked because there is an association with depression, immune activation, and the release of inflammatory cytokines [12]. The gastric ulcer found on EGD in Patient A is another severe inflammatory process present that may be adding to systemic inflammation. Associations between silent gastric ulcer disease and type 2 diabetes have been established, so it is important for clinicians to be aware of this relationship, especially when patients are already in the overweight or obese BMI range. It is unclear whether or not both patient's CD symptoms began or were exacerbated by these ongoing inflammatory processes. Autoimmune diseases and other inflammatory processes may be used as potential clinical markers for CD - an inflammatory disease itself -because autoimmune diseases tend to cluster together [13].
Both patients could benefit from HLA DQ2/DQ8 genotyping, as it offers yet another diagnostic tool for clinicians to use when patients present with nondescript gastrointestinal symptoms, if labs are borderline elevated, or if other diagnostic measures have already been exhausted. Although Patient A expressed that finances would likely be a barring factor in having more testing done, a potential area for further clarification regarding her diagnosis and condition would be genetic HLA testing. HLA DQ2/DQ8 genetic testing has high sensitivity, low specificity, and a high negative predictive value for CD. This testing is highly accurate in excluding the diagnosis of CD, however if patients are found positive for either HLA DQ2 or DQ8, it may not shed much light on the other diagnoses, as 25-30% of Americans are positive for at least one of these molecules [14].
We reported two atypical presentations of CD in two obese women in their mid-thirties. While CD is known for its common presenting symptoms such as diarrhea and weight loss, it may also present with initial symptoms of recurrent upper abdominal discomfort, nausea, and more, as seen in these two cases. It is important that physicians are informed of other diagnostic clues of CD, including its association with other autoimmune diseases, iron deficiency anemia, IEL's and advanced villous atrophy on histopathology. Earlier recognition of CD will result in better disease outcomes for patients, improved patient care, and increased quality of life.
We would like to thank the patients for the opportunity to present this research and for the family and friends that offered support to us during the process of completing this case report.
None.
All authors contributed equally to this case report.