Ischemic stroke following a snakebite is a rare complication. We report a case of a 49-years-old male who developed weakness of right upper and lower limb slurring of speech with facial asymmetry following Russell's viper bite. Magnetic resonance imaging of brain revealed infarct in the left middle cerebral artery territory. The possible mechanisms for cerebral infarction in this scenario are discussed, which were hypotension causing watershed infarcts due to hypovolemia.
Russell viper, Middle cerebral artery infarct, Hypotension, Watershed infarct
Snakebites are a common cause of morbidity and mortality in India. Over 20,00,000 snakebite cases were reported annually in India, among them 35,000-50,000 people die [1,2]. Predominantly, bites are more frequent among males, in the lower limb and during the rainy season [3]. The snake venoms are basically of two types: Neurotoxic and hemotoxic. Russell's Viper (Dabobia russelli) is widely distributed and the leading cause of fatal snakebites in India [1]. Viper envenomation causes multiple local and systemic manifestations including severe local bite site injury, cellulitis, neuroparalysis, coagulopathy, acute kidney injury, renal failure, generalized rhabdomyolysis, shock, spontaneous systemic bleeding, and hemorrhagic manifestation's including pituitary, intracranial hemorrhage and neurological manifestations confine only to cranial nerves commonly ptosis and external ophthalmoplegia [4]. Viper bites have been associated rarely with cerebrovascular accidents, most commonly due to hemorrhagic and rarely due to infarct [5]. Ischemic stroke following a viper bite is rare but the most common and serious neurological complication is intracranial hemorrhage. Ischemic stroke commonly involves anterior circulation. Here we describe a polyvalent anti-snake venom-treated patient with acute infarct in the left middle cerebral artery territory with mass effect following Russell's viper bite.
A 49-years-old previously healthy male was admitted to the emergency medicine department of a tertiary care hospital with complaints of snake bite on his right second toe while working in the agricultural field. The snake was identified as Viper as per the descriptions given by the patient attendees. A few minutes after the bite, the patient noticed minimal swelling over the right second toe. The patient was immediately taken to a Local hospital and was given 10 vials of polyvalent anti-snake venom. Following that, after 48 hours of the snake bite patient developed weakness in the right upper limb and lower limb with speech difficulty with facial weakness to the right-side present. CT Brain plain showed acute infarct in left middle cerebral artery territory, and ill-defined axial hypodensities noted in the left corona radiata, left basal ganglia, left caudate, left lentiform nucleus anterior limb of left temporo-parietal lobe with mild effacement of left lateral ventricle (Figure 1). MRI Brain showed acute infarct in the left temporo-parietal lobes, capsuloganglionic region, and corona radiate- middle cerebral artery territory was observed (Figure 2). The patient was referred to our hospital for further management. On arrival, the patient was conscious, afebrile, obeying commands with GCS E4V2M6 with weakness of the right upper limb and lower limb, pupils were bilaterally equal with 3 mm reacting to light and slurring of speech with a deviation of angle of mouth to left. The patient had severe pain and cellulitis over the right foot (Figure 3). Complete blood count with leucocytosis, PT, aPTT, and INR was prolonged (Table 1), and 2D Echo showed normal with an ejection fraction of 59%. The patient was treated with antibiotics, aspirin, and clopidogrel orally. There was remarkable improvement in the motor power and speech on discharge on the tenth day.
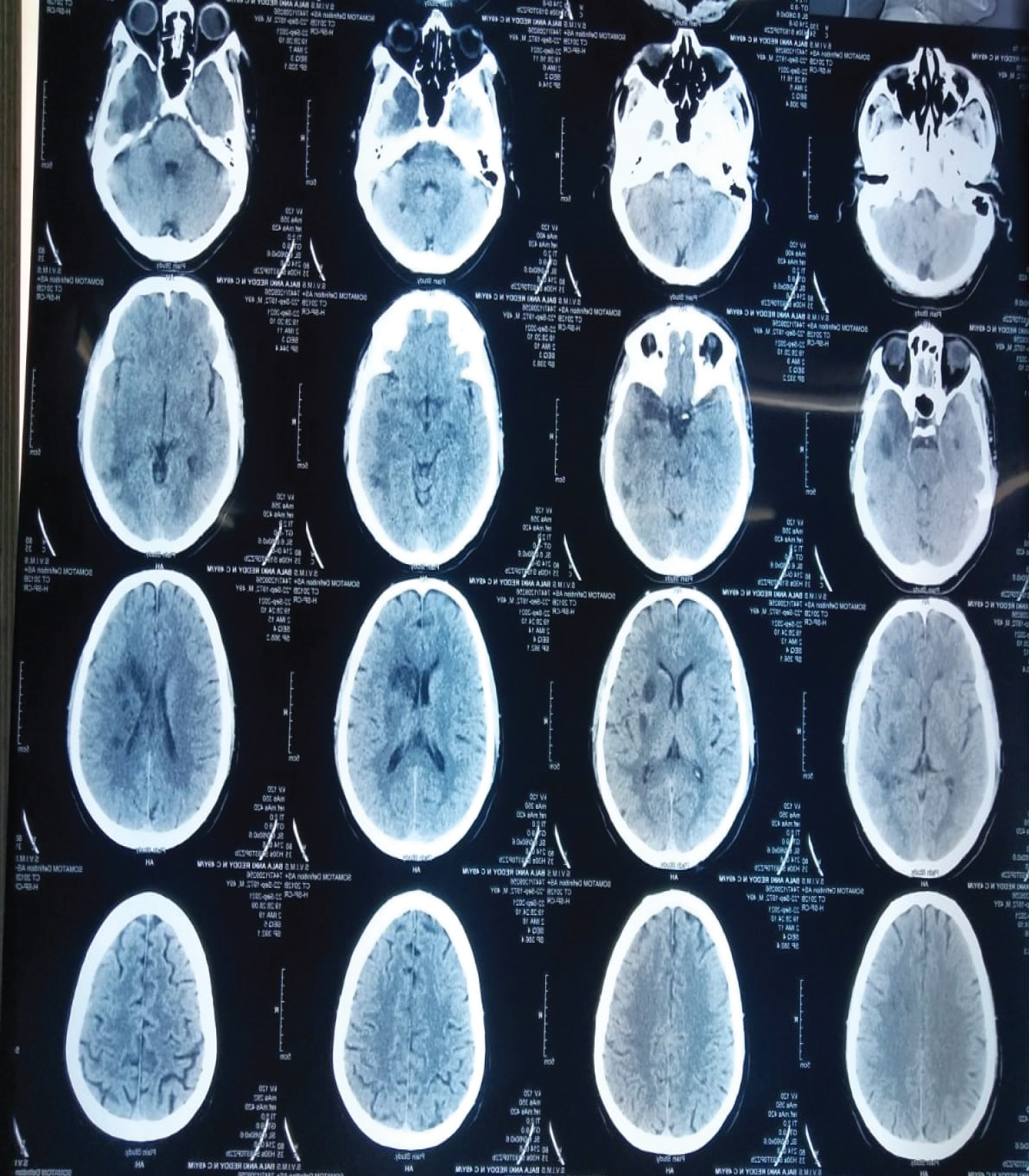 Figure 1: CT brain - acute infarct in left middle cerebral artery territory with mass effect with ill-defined axial hypodensities in the left corona radiata, centrum semi ovate, left caudate, left lentiform anterior limb of temporal lobe with mild effacement of left lateral ventricle and adjacent sulci.
View Figure 1
Figure 1: CT brain - acute infarct in left middle cerebral artery territory with mass effect with ill-defined axial hypodensities in the left corona radiata, centrum semi ovate, left caudate, left lentiform anterior limb of temporal lobe with mild effacement of left lateral ventricle and adjacent sulci.
View Figure 1
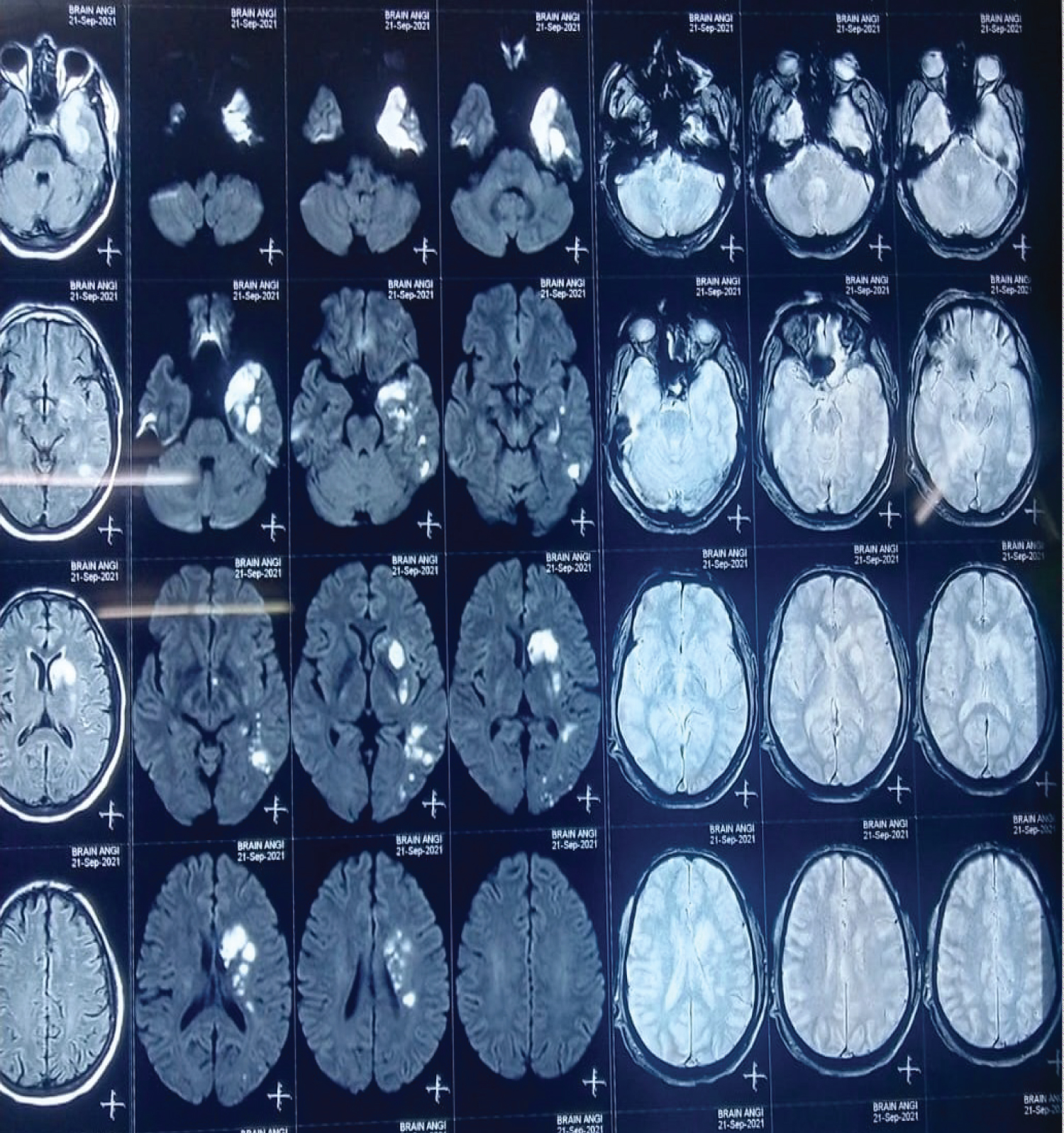 Figure 2: MRI brain large area of acute infarct distributed in left temporooccipito parietal lobes, capsuloganglionic region and corona radiate - MCA territory.
View Figure 2
Figure 2: MRI brain large area of acute infarct distributed in left temporooccipito parietal lobes, capsuloganglionic region and corona radiate - MCA territory.
View Figure 2
 Figure 3: Showing cellulitis of right second toe.
View Figure 3
Figure 3: Showing cellulitis of right second toe.
View Figure 3
Table 1: Laboratory investigations. View Table 1
This paper describes a case of snake bite with an atypical clinical presentation. Cerebral complications, particularly ischemic stroke, following snake bite, is rare and only a few cases of cerebral infarction resulting from viper bite have been reported in India and worldwide [5-8]. Most reported cases had anterior circulation strokes. In a study done by Mosquera, et al. out of 309 snake bite patients, 8 patients (2.6%) were having cerebrovascular complications of which 7 were hemorrhagic strokes and 1 ischemic stroke [5]. Bashir and Jinkins reported a patient in whom envenomation with Russell's Viper resulted in hemiplegia and aphasis, consistent with a middle cerebral artery infraction [7].
Viper venom is a complex toxin with rich components principally affecting hemostatic mechanisms [4]. Most of the vipers exhibit both anticoagulant and procoagulant effects. The Postulated mechanisms for cerebrovascular accidents following a snake bite are multifactorial they are venom procoagulants i.e., phospholipase A2, Kunitz type serine inhibitors, snake venom serine protease, snake venom metalloproteinase, c-type lentins, neurotoxic 3Ftx, cytotoxic 3FTx they cause intravascular coagulation that leads to microthrombi formation by small and large vessel Occlusion [9,10]. Hyperviscosity from hypovolemia and hypoperfusion causes small and large vessel occlusion [11]. Hypotension can occur due to hypovolemia from vomiting, decreased fluid intake and sweating, leading to watershed infarcts [7]. Complement-mediated toxic components of snake venom cause vasospasm, endothelium damage, and increased vascular permeability leading to toxic vasculitis and thrombosis. Cardiotoxic effects of venom cause dysrhythmias and cardiac thromboembolism. The synergistic action of venom components causes enhancing venom toxicity which causes hemolysis, thrombocytopenia, and hypotension [12].
Our patient was middle-aged men with no co-morbidity illness. Transthoracic echocardiography was negative for cardiogenic emboli. Clotting and Bleeding time were normal, which ruled out DIC. Infarct in our patient is most probably due to hypotensive etiology through possible, hypotension usually tends to cause watershed territory infarcts. We report this case to highlight this uncommon presentation of viper bite.
After the viper bite, cerebrovascular manifestations can be attributed to various mechanisms, such as toxin-induced vasculitis and thrombosis, anticoagulant and procoagulant effect, vasospasm, and endothelial damage, disseminated intravascular coagulation, and hypotension. Needless to say, in a snake bite-prone country like India, it is necessary to evaluate the patients with ischemic stroke or neurological disorder and possible viper bite. Proper monitoring of fluid assessment will prevent this rare but devastating complication.
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that his name and initials will not be published, and due efforts will be made to conceal his identity, but anonymity cannot be guaranteed.
Nil.
There are no conflicts of interest.