Asbestos fibres, inhaled and displaced by various means to lung tissue, may cause a spectrum of diseases from benign diseases to malignancies. Pleural plaques (PPs) are usually asymptomatic and cause slight impairment of lung function only when they are extended in size [1]. The cause of pleural plaques is exposure to asbestos fibres, most commonly in an occupational setting [2]. Relationships between the dose-response and prevalence of asbestos-related diseases are complex [3]. We present a case of asymptomatic benign pleural plaque due to asbestos exposure accidentally found on medical check up in a former tuberculosis (TB) patient.
Asbestos is a fibrous hydrated magnesium silicate. Intensity and duration of exposure play an important role in the prevalence of asbestos-related disease [4]. Asbestos fibres, inhaled and displaced by various means to lung tissue, may cause a spectrum of diseases from benign diseases to malignancies [1]. Pleural plaques are the most common manifestation of asbestos exposure [4]. They are usually asymptomatic and cause slight impairment of lung function only when the size are extended [1]. Most often they are incidental findings on chest X-rays (CXR) [4]. Common sites are the posterolateral midzones, following the rib contour, and on the diaphragm. The lesions are usually stable and remain the same size for months with irregular borders usually found on the parietal and rarely on the visceral pleura [4,5]. This helps to differentiate plaques from pleural tumors. Histological tissue examination is not necessary for diagnosis and no specific treatment is required. Medical surveillance, including periodic CT scans and blood biomarkers, are recommended [4]. About 80% of individuals significantly exposed to asbestos will have plaques on the CXR while only 0.5-8% of an unexposed population will reveal such findings [3]. Between 5 and 15% of those with occupational exposure will have plaques after a latent period of 20 years, rising as the latent period increases. Two studies in France stated that the prevalence of PPs in 5545 asbestos exposed workers was 15.9% and in a second study, 46.9% of 1011 [2].
Two theories have been proposed for the pathogenesis of pleural plaques. The most plausible is based on the direct effects of fibers that reach the pleural space [4]. Asbestos fibers may pass alveolar barrier then reach the lung interstitium via paracellular route due to osmotic and hydraulic pressure gradient. Fibers can be dragged from lung interstitium by pulmonary lymph flow (primary translocation) wherefrom they can reach the blood stream and subsequently distribute to the whole body (secondary translocation). Secondary translocation to the pleural space may occur via the physiological route of pleural fluid formation across the parietal pleura. Figure 1A shows the pathogenesis of primary translocation (black arrow) and secondary translocation (white arrow) of asbestos fibers to pleural cavity. Inflammation reverses the transendothelial and trans-mesothelial pressure gradients which then increases the pulmonary interstitial pressure. This causes primary translocation of asbestos fibers in pulmonary capillaries and across the visceral pleura, as shown in Figure 1B [6].
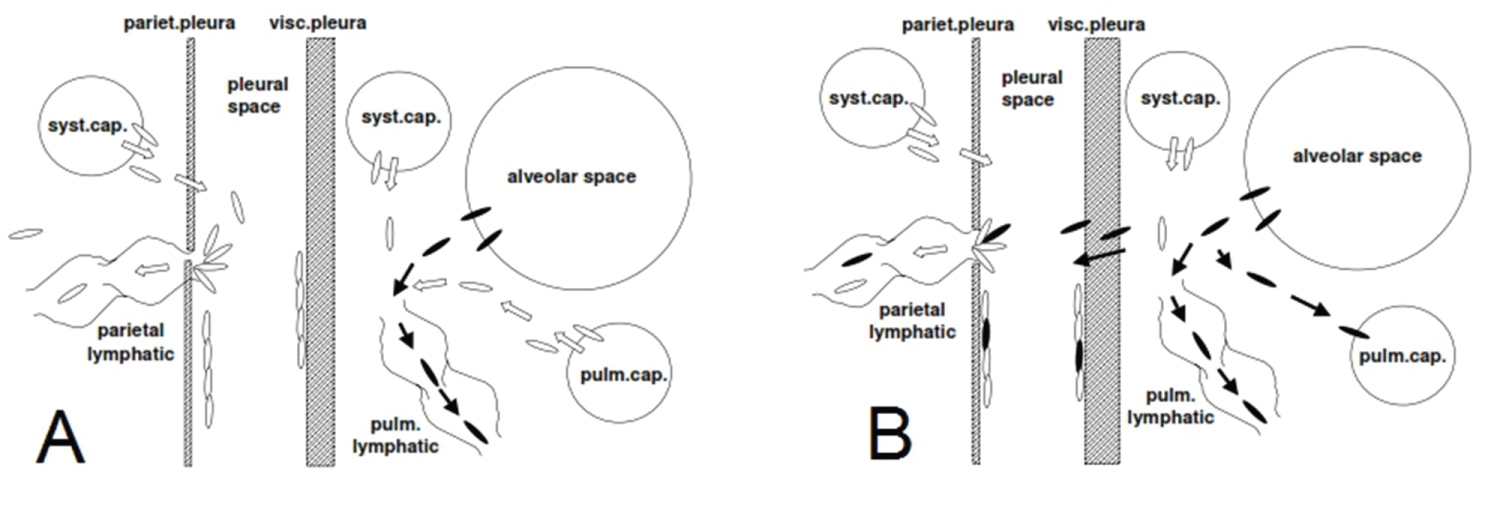 Figure 1: Pathogenesis of asbestos fibers' primary and secondary translocation to pleural cavity. View Figure 1
Figure 1: Pathogenesis of asbestos fibers' primary and secondary translocation to pleural cavity. View Figure 1
A 49-year-old male was referred to our clinic in Persahabatan Hospital because abnormality of his CXR since year 2000. He had neither respiratory symptoms (cough, dyspnea, chest pain and hemoptysis) nor constitutional symptoms (fever, night sweat and weight loss). His CXR was stated abnormal since he was diagnosed having pulmonary TB in 2000. The abnormality was persistent, neither getting worse nor getting better. This abnormal CXR was considered problematic in every medical check up held by the company he worked for. The patient had a history of pulmonary TB in 17 years prior admission. He completed the first category of antituberculosis drugs for 6 month from other hospital and was stated as cured. The patient was also diabetic and had routine insulin injection intramuscularly since 17 years ago. In the last twenty five years, he had been working in many building development projects. The working activity was vary, from indoor office activity in a semi-permanent building (with a roof made from asbestos) to outdoor monitoring activity. He worked from 8 a.m to 7 p.m and rarely used the respiratory protection devices.
This patient had no smoking history. He stated that his house had a ceiling made from asbestos. The physical examination showed a good general condition with normal vital signs (respiratory rate of 16/min and peripheral oxygen saturation of 98% in room air). On pulmonary examination we did not find any abnormalities. We could not afford to get the previous CXRs so we did thoracal CT scan (Figure 2 and Figure 3). The CT scan showed right pleural thickening. We diagnosed the patient as Benign right pleural plaque ec asbestos exposure with former TB. Since the patient was asymptomatic, we did not manage the patient with any medical treatment. We advised the patient to have a routine medical check-up, especially thoracal CT scan, yearly or whenever he is symptomatic. The patient is still healthy and routinely undergoes medical check-up.
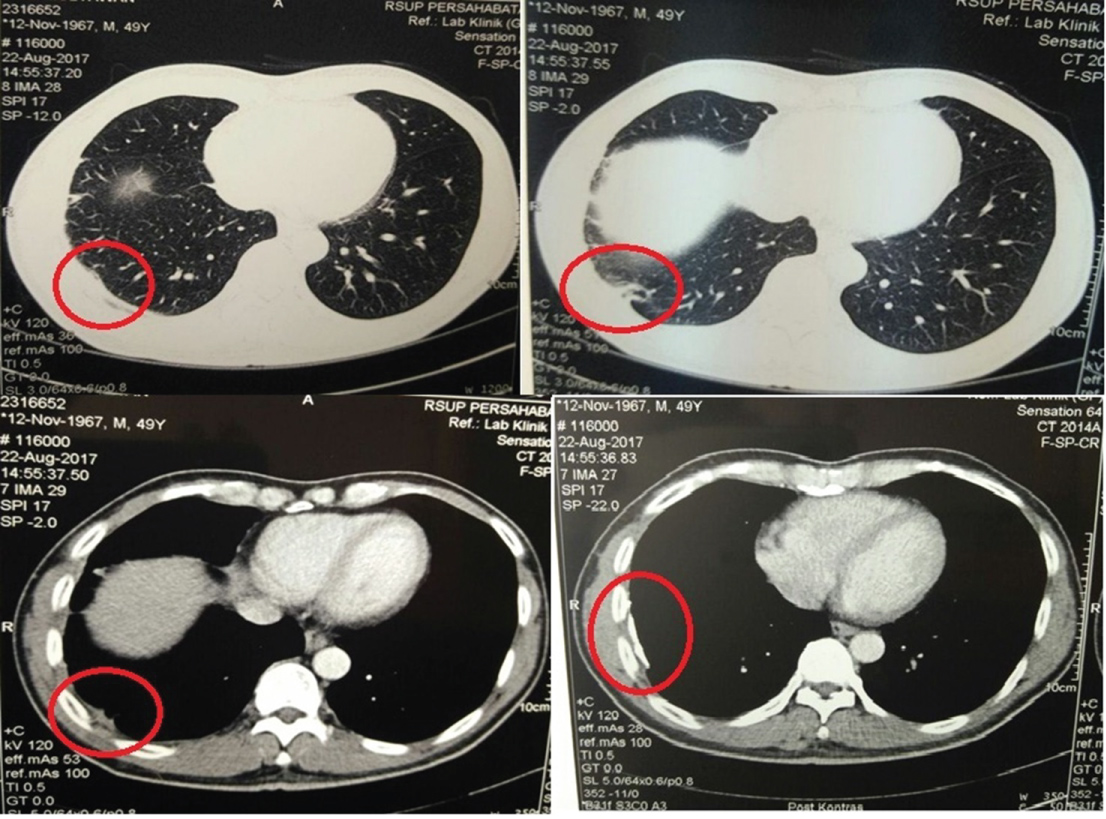 Figure 2: Axial view of thoracal CT in lung and mediastinal windows: right pleural plaque following the rib contour. View Figure 2
Figure 2: Axial view of thoracal CT in lung and mediastinal windows: right pleural plaque following the rib contour. View Figure 2
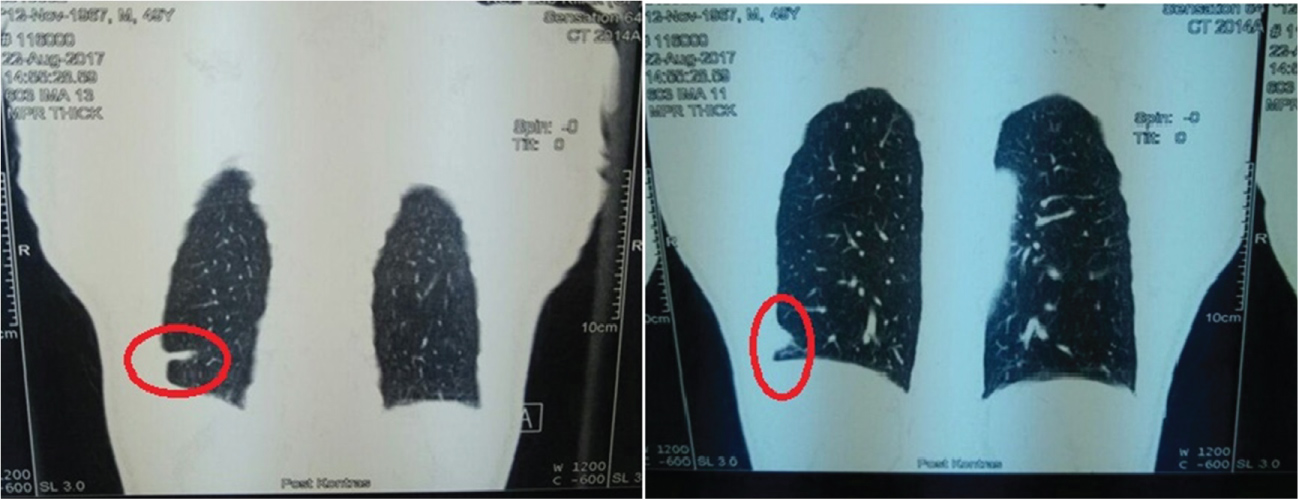 Figure 3: Sagital view thoracal CT in lung window: right pleural plaque. View Figure 3
Figure 3: Sagital view thoracal CT in lung window: right pleural plaque. View Figure 3
Pleural plaques are usually asymptomatic [4]. Our patient had neither respiratory nor constitutional symptoms. Pleural plaques are often incidental findings in CXR. The lesions are usually stable and remain the same size for months [4]. The CXR of our patient could not be obtained but the radiographic abnormality had remained unchanged for 17 years. They may follow the rib contour in radiographic examination [5]. Pleural plaque following the rib contour in our patient is shown in Figure 2. A study from Mazzei, et al. found that lower half chest wall with dorsal predominance was more commonly involved than the upper one [1]. Kim, et al. also stated the same thing in their study which compared the occupational and environmental asbestos exposure [7]. The thoracal CT of our patient showed that the PPs was found in dorsal-lower half of the chest wall, shown in Figure 3.
The prevalence of PPs is most strongly related to the length of time since first exposure and when detected there is usually a latent period of 20-40 years. Prevalence is also statistically related to the duration of exposure, the level of exposure and the cumulative exposure [2]. Our patient had been working for 25 years in bulding development projects, 11 hours per day, which gave high duration and cumulative exposure. A systematic review from Kerper, et al. stated that most reviewed studies did not report any statistically significant differences in any spirometry parameters between populations with and without pleural plaques [8]. Our patient did not undergo spirometry examination because he was asymptomatic, even if we did the spirometry, the result would not differ from normal patient.
The patient had a history of pulmonary TB in 2000. A study on the relationship between asbestosis and pulmonary TB determined that there was no statistically significant difference in the incidence of tuberculosis in patients with asbestosis and healthy people. A historical cohort study looked at the prevalence of pulmonary TB in workers with asbestosis in Hong Kong and found the prevalence of PTB infection was high in these subjects [9]. Old tuberculosis infection often causes calcified or non-calcified visceral pleural thickening near the lung apices [10]. Calcified pleura are also seen as a result of prior infection (either pyogenic, tuberculous or fungal) although usually unilateral, more extensive and in continuity [11]. The pleural plaque in our patient occurred before the pulmonary TB. The CXR in 2000 when the patient was diagnosed as TB had already shown the pleural plaque (prior to TB). The plaque in our patient was also located in the lower half of right hemithorax in dorsal area while pleural calcification of TB occurs in the apices, so the plaque was not due to TB. Based on our findings, the pleural plaque in our patient was caused by the occupational asbestos exposure.