A 46-years-old male with the history of multiple sclerosis applied to urology outpatient clinic with frequency, urgency, incontinence, and nocturia. Urodynamic evaluation presented Valsalva-induced urge incontinence, which was an unusual finding for an MS patient. Here we present an MS patient with the urodynamic finding of Valsalva-induced urge incontinence.
Multiple sclerosis, Incontinence, Urgency, Valsalva-induced
Multiple sclerosis (MS) is a chronic progressive demyelinating disease of the central nervous system, mostly affecting the people between 20-45 years of age with a female predominance [1]. Although the etiology is uncertain, Ebsteinbarr virus, sunshine, smoking and vitamin D, combined with an individual's genetic background, play important roles in etiology [2]. Multiple sclerosis is a predominant disease affecting nearly 2.1 million people around the world. The prevalence rates vary between 40 and 220 per 100.000 and the annual incidence rates estimate 2.3 and 11.6 per 100,000 [3,4].
Symptomatology of MS ranges widely according to the location of lesions in the central nervous system. Lower urinary tract symptoms (LUTS) are common in MS patients with an incidence of 50-80% [5]. Urgency and/or urge incontinence is the predominant urinary tract symptoms in MS patients. Urge incontinence is defined as; the involuntary loss of urine associated with urgency. The rate of stress type incontinence in MS patients is less than urge incontinence and it is defined as the complaint of any involuntary loss of urine on effort or physical exertion or on sneezing or coughing [6].
Urodynamic studies documented that detrusor overactivity (DO), detrusor-sphincter dyssynergia (DESD) and detrusor underactivity are the main urodynamic findings of MS patients [3,4]. Here we present a male patient with MS who had proven urodynamic valsalva induced urge incontinence.
A 46-years-old male patient applied to urology outpatient clinic with frequency, urgency, and incontinence. The patient was voiding in every hour during the daytime and had nocturia (3-5 voiding/night). He also reported frequent incontinence episodes both during daytime and nighttime every day. The duration of symptoms was three years and they werehad been aggravated in the last six months. There were no obstructive symptoms. The patient had no co-morbidities and he was under the treatment of daily Glatiramer set at 20 mg. He applied to neurology outpatient clinic three months ago with weakness and numbness in the lower extremities and urinary incontinence. Neurological examination was consistent with paraparesis, lower extremity hypoesthesia, brisk deep tendon reflexes at lower extremities, and extensor plantar reflexes bilaterally. Brain magnetic resonance imaging showed periventricular demyelinating lesions without contrast enhancement (Figure 1a). Cervical and thoracal spinal magnetic resonance imaging (MRI) was consistent with demyelinating lesions without contrast enhancement (Figure 1b and Figure 1c). Lumbar puncture performed and positive oligoclonal band obtained. The diagnosis of the patient was multiple sclerosis.
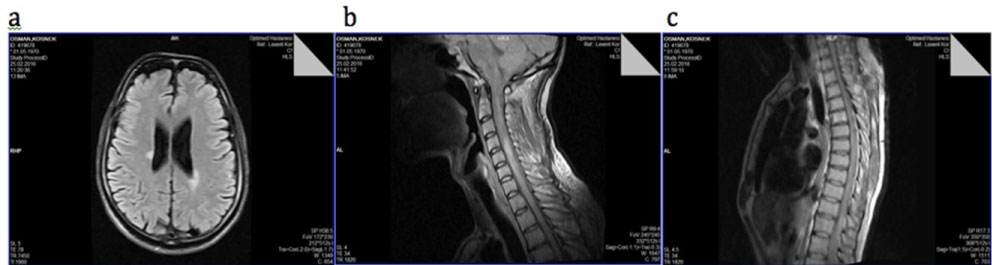 Figure 1: T1-weighted images of cranial, cervical and thoracal spinal MRI show demyelinating lesions. a) Cranial image; b) Cervical image; c) Thoracal image.
View Figure 1
Figure 1: T1-weighted images of cranial, cervical and thoracal spinal MRI show demyelinating lesions. a) Cranial image; b) Cervical image; c) Thoracal image.
View Figure 1
The urinalysis, urine culture and biochemical evaluation (total serum PSA and serum creatinine) were within normal ranges. Urinary system ultrasonography showed no abnormality. During the uroflowmetric assessment, patient voided 212 ml of urine with a maximum voiding rate of 16.2 ml/sec. Suprapubic ultrasonography showed 10 ml of post-voiding residue. On 3-days voiding diary, patient voided 10-12 times in daytime and 3-5 times per night with a range of 50-100 ml. of bladder capacity. He also reported frequent incontinence episodes at various times of day and night.
Urodynamic evaluation was performed according to the International Continence Society (ICS) standards (Aymed Medical Technology, Turkey) with an infusion rate of 20 ml/min [7]. The patient did not indicate the first sensation during bladder filling. According to our clinical urodynamic protocol, the patient was alerted to cough in every 50 ml of bladder filling. We observed an increase in detrusor pressure reaching to 136 cm H2O just after a cough at the volume of 50 ml. This contraction induced urinary flow of nearly 10 ml and resolved spontaneously. The second detrusor contraction was noted at the point of 100 ml infusion just after a cough and reached to 139 cm H2O. This contraction also induced urinary flow of 37 ml and resolved spontaneously. A third contraction was observed at the volume of 150 ml, which was even occurred after a cough, and this contraction caused leakage of 65 ml. These leakages continued in the same fashion during urodynamic evaluation, and we were not able to evaluate the exact maximum cystometric capacity (Figure 2). We repeated the test with other types of provocations like cold saline infusion and hand washing, but we did not observe detrusor overactivity related to these provocations. During the second urodynamic evaluation, the only detrusor overactivity was noted spontaneously at the volume of 150 ml, which resulted in micturition. The maximum cystometric capacity on the second urodynamic evaluation was 378 ml. The external sphincter activity was determined by superficial electrode EMG activity. The external sphincter activity was normal.
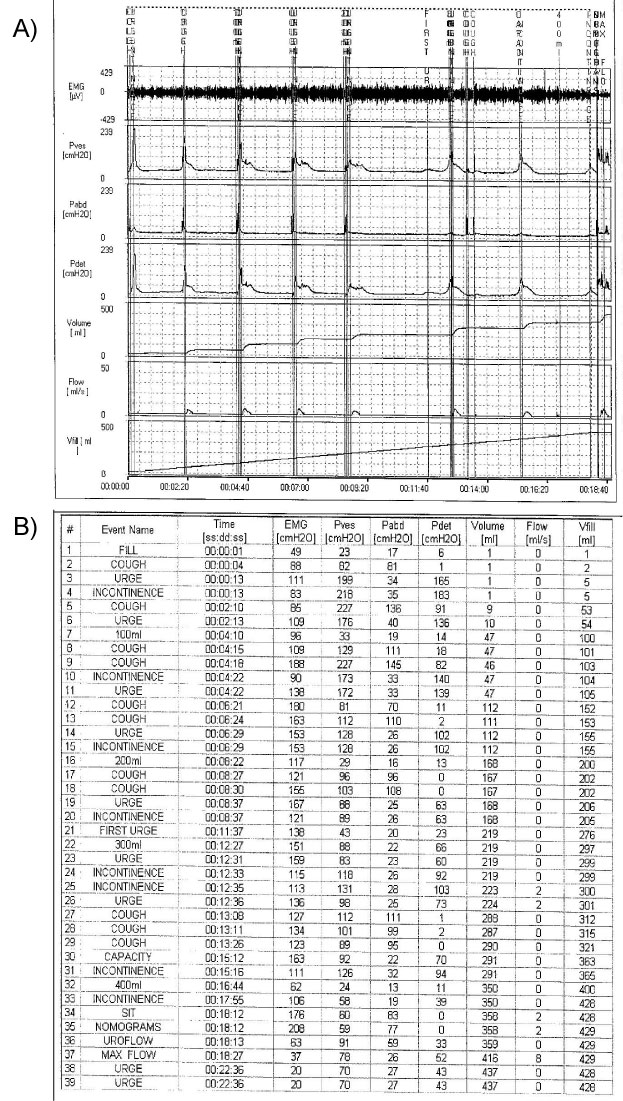 Figure 2: The urodynamic investigation of a patient demonstrating the unexpected type of incontinence; stress-induced urge incontinence.
View Figure 2
Figure 2: The urodynamic investigation of a patient demonstrating the unexpected type of incontinence; stress-induced urge incontinence.
View Figure 2
Multiple sclerosis is a demyelination disease of the central nervous system that causes impairment of conduction velocity in axonal pathways. This impairment causes several neurological abnormalities including urological dysfunctions. The most common urological symptoms in MS are urinary incontinence and frequency. Impaired bladder emptying and voiding dysfunction can also be observed. The main urodynamic findings related to these symptoms are neurogenic detrusor overactivity, detrusor sphincter dyssynergia, and detrusor underactivity. Neurogenic detrusor overactivity is the most common urodynamic finding representing 25-100% of all urodynamic findings [8]. The second most common urodynamic finding is detrusor sphincter dyssynergia (3-71%). These two conditions may be observed in the same patient, which complicates the situation and increase the risk of the upper urinary system. Even, impaired detrusor contractility and areflexia may be found in 3-73% of patients [9]. The urodynamic investigation is recommended in every neurogenic bladder patient to document the function or dysfunction of lower urinary tract [10]. Different urodynamic findings may be present in MS patients, and this represents the complexity of the disease. The wide range of lower urinary tract symptoms in MS patients is related to the disease characteristics. The demyelination process can be seen in every part of the central nervous system from lateral corticospinal columns to the lumbosacral cord. Several studies tried to demonstrate the relationship between lower urinary tract symptoms and the location of demyelination, but none of them was able to explain a significant relation [11,12].
Urgency and urinary incontinence are the main lower urinary tract symptoms of MS patients. Neurogenic overactivity is mostly responsible for these symptoms. Our patient also applied to the outpatient clinic with urgency and urge incontinence. Detrusor overactivity was also supposed to be the reason for urinary incontinence, and the patient received antimuscarinic treatment for three months. Even after dose escalation, the patient did not benefit from antimuscarinic therapy. As the patient was resistive to medical treatment, urodynamic evaluation was performed. Urodynamic evaluation significantly demonstrated incontinence episodes with Valsalva, which was diagnosed as Valsalva-induced urge incontinence. This pattern of the urodynamic finding was an infrequent finding for an MS patient. Although the studies related to MS demonstrated the high rate of detrusor overactivity and detrusor sphincter dyssynergia, there is no study showing the presence of Valsalva induced urge incontinence in patients with MS. According to our knowledge, this is the first case report documenting the Valsalva-induced urge incontinence in a male MS patient.
The unstable pattern and location of the demyelination area along with the associated edema are responsible for the alteration in both the neurologic and urologic features of the MS. In general, suprasacral plaques will cause varying degrees of detrusor hyperreflexia and sacral plaques will result in detrusor hypocontractility [13]. Valsalva-induced urge incontinence is a unique situation related to the reflex arch of the bladder. The flow of urine to proximal urethra induces a reflex detrusor contraction, which is an essential mechanism for normal voiding. This reflex arch can cause a pathological situation, as the bladder outlet is open due to internal sphincter dysfunction and pelvic muscle weakness. Although this pathology was defined in women, it is scarce among men who have stronger sphincter function. Presence of Valsalva-induced urge incontinence at our patient gave rise to the idea that MS might also affect internal sphincter function. Internal sphincter muscle of urethra constricts the internal urethral orifice and is under control of the sympathetic nervous system. Sympathetic nerves arise from the intermediolateral nucleus of the lateral grey column at the level of T1 to L2-L3, which is near the middle of the spinal cord. Our patient has demyelinating lesions at the thoracal spinal cord at the T6-7, T8-9, T9-10 and T10-11 levels. The sympathetic nervous system involvement at the thoracal spinal cord may be the main reason for internal sphincter dysfunction that might induce Valsalva-induced urge incontinence.
Multiple sclerosis patients show different clinical presentation due to the heterogeneity of the demyelination area. Detrusor overactivity is the main urodynamic finding of MS patients. Valsalva-induced urge incontinence is a rare phenomenon for MS patients and might be related to the lesion at the sympathetic trunk. Clinicians must be aware of this unexpected situation.