Tuberculous meningitis (TBM) is the most fatal form of the Mycobacterium tuberculosis infection. Its diagnosis remains difficult due to poor suspicion of the disease especially in the case of pregnancy. We bring to your attention a 27-year-old pregnant woman who came to the emergency department with headache and nausea. With high clinical suspicion and early treatment with Meropenem 3x2 gram, Levofloxacin 2 x 500 mg, Amoxicillin Clavulanate 3 x 1 gram, Ethambutol 1 x 25 mg/kg body weight, Pyrazinamide 1 x 15 mg/kg body weight and 0.4 mg/kg body weight Dexamethasone resulted in patient's recovery. The immune tolerant state of pregnancy and its relationship with the M. tuberculosis infections needs further research. Clinicians need to think about the TBM and other tuberculosis infections for prompt diagnosis and early treatment.
Tuberculous meningitis, Tuberculosis, Pregnancy
Tuberculosis (TB) is an infectious disease caused by a group of Mycobacterium species called the Mycobacterium Tuberculosis (MTB) complex. Tuberculosis is still one of the leading causes of death from an infectious disease, with more than 10 million people getting diagnosed with tuberculosis each year [1].
Globally, an estimated 9.8 million (range, 8.8-10.9 million) people fell victim to TB in 2020, a number that has been declining very slowly in recent years. There were an estimated 1.28 million (range, 1.21-1.36 million) TB deaths among HIV-negative people in 2020 [2].
Drug-resistant TB continues to be a public health threat. Worldwide in 2020, nearly 160.000 people developed rifampicin-resistant TB. The highest risk populations for TB are children and immunocompromised such as HIV infected and major risk factors for developing TB are, undernourishment, HIV, alcohol use disorders, smoking and diabetes [2]. Despite pregnancy cannot be clinically defined as immunosuppression, it has an immunosuppressive process to prevent rejection of the fetus [3].
TB can affect many systems, especially the respiratory system but the most fatal form of TB is Tuberculous meningitis (TBM). The diagnosis of TBM remains difficult as its suggestive clinical features occur with widely variable frequencies. Fever, headache, and meningeal irritation signs are its cardinal features [4].
The incidence of TB during pregnancy is increasing in both developed and developing countries, a recent systematic review of latent TB in pregnancy revealed a prevalence of 14 to 48% in the United States, with skin test positivity varying with ethnicity, representing a significant opportunity to potentially impact upon the development of TB disease in both the mother and the infant [5].
It is important to underline that diagnosis of TB and TBM is even more challenging during pregnancy because most of the presenting symptoms can be attributed to state of pregnancy itself. This report focuses on a case of a 27-year-old pregnant woman presenting with headache and nausea whose symptoms began one week earlier. Because of her rapid deterioration in mental state a lumber puncture was performed urgently, and she was diagnosed with TBM. Early diagnosis and treatment led to a dramatic improvement in her mental state and maintenance of fetal viability.
A 27-year-old women gravida 3 para 2 (2 alive) with estimated gestational age at presentation of 27 weeks came to the emergency department (ED) with headache and nausea which began one week ago. These complaints thought to be because of pregnancy, and she was discharged after a prescription. When she had a fever of 38.5 degrees, nausea, vomiting and altered state of consciousness for 2 days; patient was brought back to the ED. She had neck stiffness and on physical examination and her Glasgow Coma Scale (GCS) score was 4/15 (E2M1V1). No history of cough, weight loss, night sweats or any contact with a known tuberculosis case. Her medical and gynecological history is unremarkable other than she is a known alpha thalassemia trait. She has not been on any medications other than vitamin supplements for pregnancy and the drugs which was prescribed when she came to the ED for the first time. She does not smoke, drink alcohol, or use illicit drugs.
Because of her positive physical examination and her altered level of consciousness a Magnetic Resonance Imaging (MRI) was ordered. MRI showed an infarction area which was located on the left temporoparietal lobe (Figure 1). The neurologist who was on call interpreted that infarction as not clinically relevant and suggested that this might be a case of encephalitis or meningitis. So, a lumbar puncture (LP) was performed. On LP, cerebrospinal fluid (CSF) protein was 6250 mg/dL, CSF glucose was 8.6 mg/dL while blood glucose was 116 mg/dL. CSF white cell count was 0.496 103 /µl and nearly 70% of them were polymorphonuclear leukocytes. With the LP results a diagnosis of TBM was made and the patient started on first line anti-tuberculous drugs which consists of 300 mg Isoniazid, 300 mg Rifampicin, 1.5 g Ethambutol, 2 g Pyrazinamide. Due to patient's worsening condition and need for a closer monitoring patient was admitted to the intensive care unit (ICU).
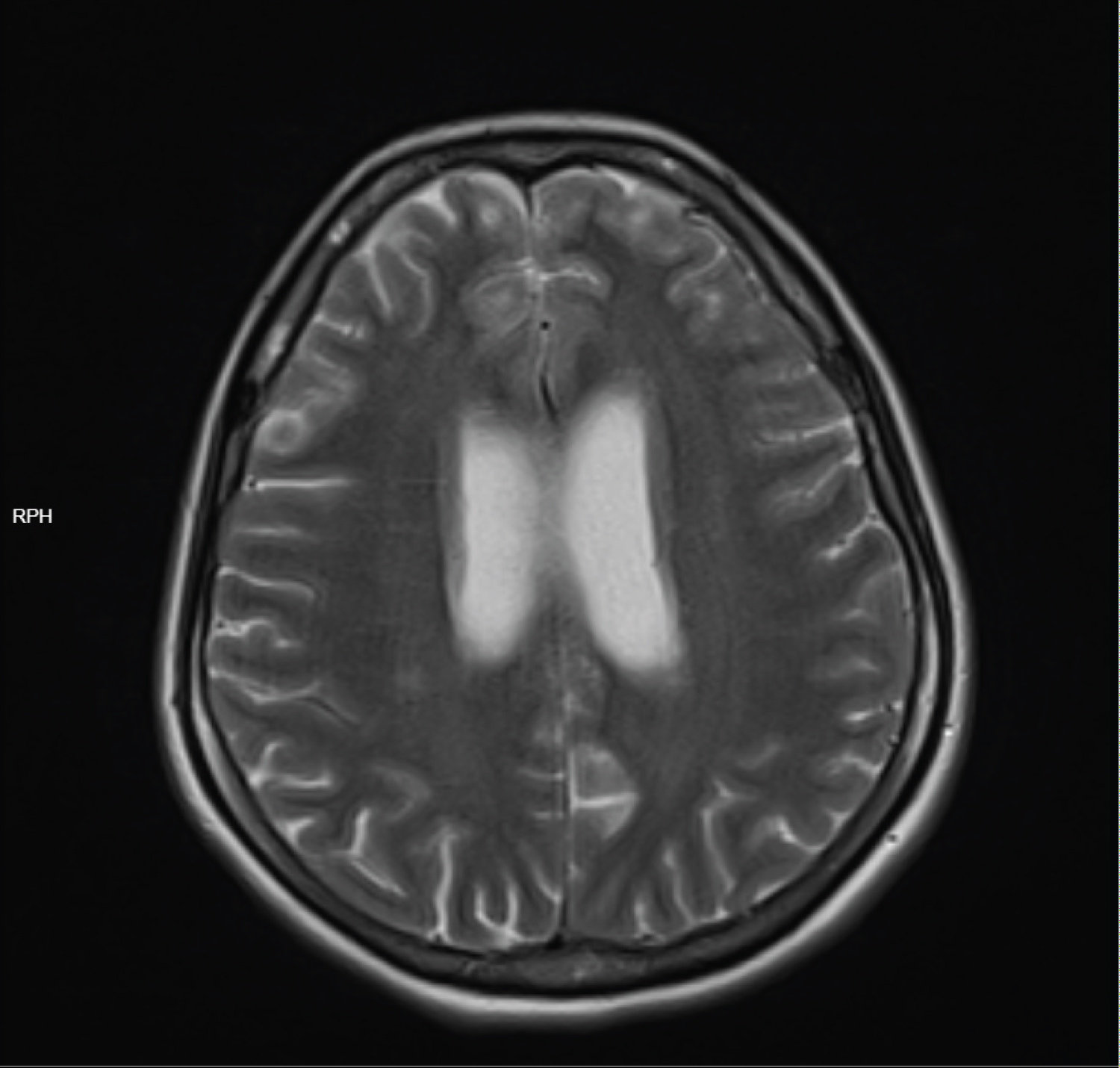 Figure 1: Brain MRI.
View Figure 1
Figure 1: Brain MRI.
View Figure 1
After her admission to the ICU, another LP was performed and the collected CSF was sent for direct gram stain and culture for bacteria, Mycobacterium tuberculosis PCR and tests for ruling out other causes of meningitis which includes pathogens such as Herpesviridae and Cryptococcus species and due to pregnancy, a thorax CT couldn't be performed to see if she has pulmonary TB. With the joined team of Obstetrics Gynecology and Infectious Diseases a chest X-ray and QuantiFERON test was the path decided on to evaluate pulmonary tuberculosis. X-Ray showed consolidation on the right upper lobes, and QuantiFERON test came as positive (Figure 2).
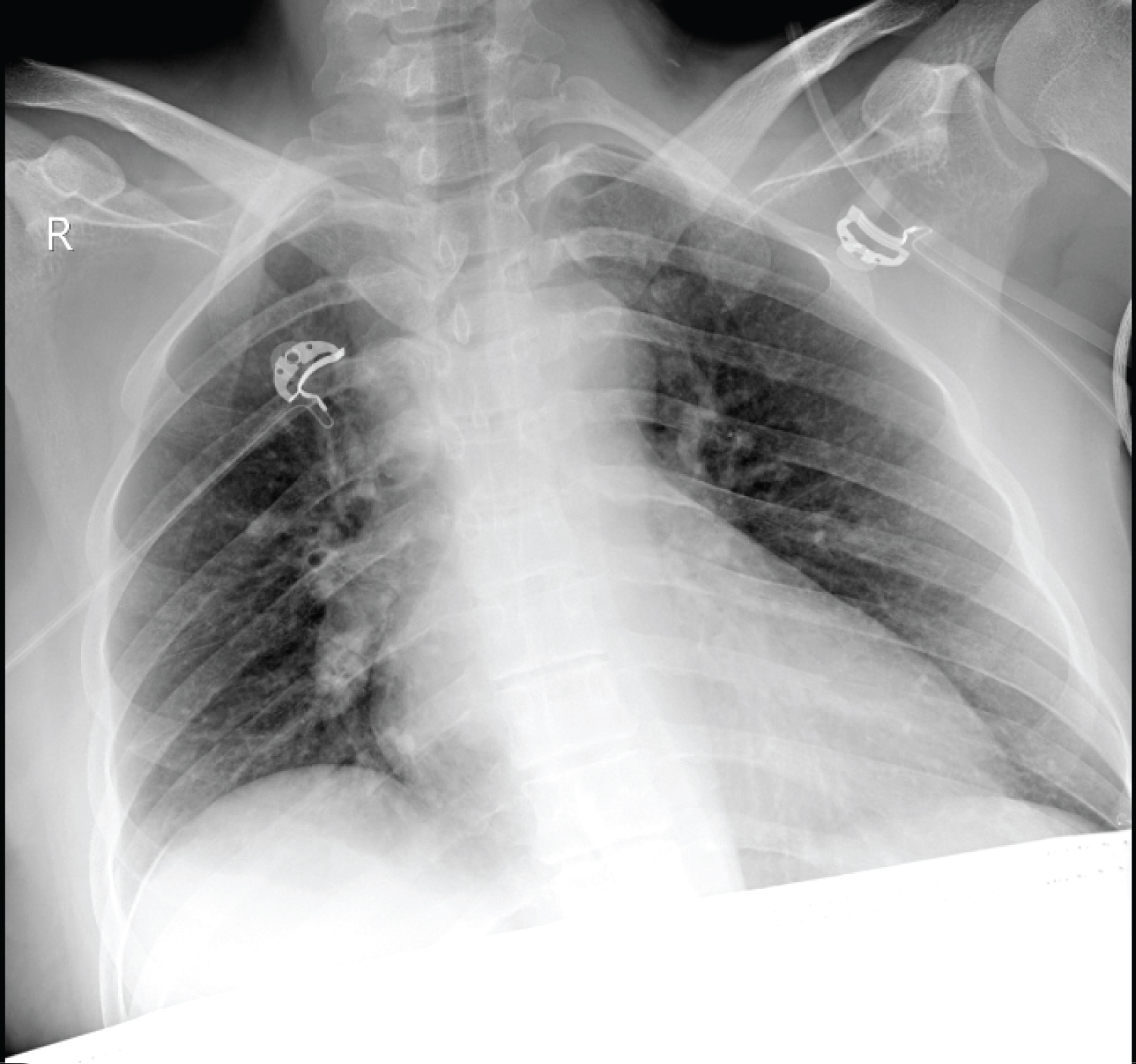 Figure 2: Chest X-ray.
View Figure 2
Figure 2: Chest X-ray.
View Figure 2
Patient's GCS deteriorated to a score of 3 on her second day in the ICU, on the same day CSF Mycobacterium Tuberculosis PCR result came back as positive and the laboratory reported Isoniazid and Rifampicin resistance in this strain of M. tuberculosis. After a consultation from infectious diseases her medications were changed to Meropenem 3 x 2 gram, Levofloxacin 2 x 500 mg, Amoxicillin Clavulanate 3x1 gram, Ethambutol 1 x 25 mg/kg body weight, Pyrazinamide 1x15 mg/kg body weight and 0.4 mg/kg body weight Dexamethasone.
Clinical improvement was observed by the 10th day with patient coming out of 10/10/2022the coma. The patient's condition continues to improve at the time of this report.
TBM is a rare but deadly disease, its risk factors are like those of pulmonary TB which includes undernourishment, HIV and other immunocompromised states and coming from an endemic area [1]. Although TBM is very rare in immunocompetent individuals, pregnancy is known to be an immune tolérante state [5]. So, this might explain the either the reactivation of the bacilli or the susceptibility to the new infection.
Untreated TBM is associated with a high incidence of neurologic impairment and mortality therefore a clinical suspicion and starting early treatment is vital for the patients [6]. However, the diagnosis of TBM is troublesome during pregnancy due to initial symptoms of TB can be dismissed as they are commonly nonspecific symptoms which can be seen during pregnancy.
There is research which show pregnancy can be considered a risk factor for TB infections and TB reactivations can be seen during pregnancy [7,8]. During pregnancy there's a down regulation of T helper 1 lymphocytes which leads to an immune suppressed state, also the IL-2 and IFN gamma modulation leading to decreased Natural Killer cell activity [9,10]. Therefore, TB infections are common during pregnancy. Especially in areas with high incidence of HIV infections and high risk for TB infections WHO recommends antenatal TB screening program [11]. Even though TB infections are common during pregnancy; extra pulmonary forms of TB such as central nervous system TB (for example, TBM, cerebral tuberculoma), TB pericarditis, genitourinary TB etc. are very rare during pregnancy, mostly these cases can be found as case reports. Our case describes a TBM in a pregnant woman who had cerebral infarcts as a complication.
TB in pregnancy is important due to two principal reasons. Firstly, there can be a delay in diagnosis. Due to some symptoms of TBM can be masked by the state of pregnancy itself such as vomiting or nausea. Also, there's a problem with radiological imaging; to avoid fetal radiation exposure one cannot easily obtain a chest X-Ray and rule out TB. In that perspective we can say that in our case, we intervened without too much of a delay in diagnosis. Because the nausea, vomiting and headache began in the third trimester, it is unlikely to be caused by hyperemesis gravidarum; and the presence of neck stiffness and altered state of mind led us to consider meningitis as a diagnosis.
Second principal reason is that the treatment of TB in pregnancy can be challenging and the effects of the drugs on the fetus must be considered also. Especially drug resistant TB cases and extra pulmonary TB infections are known to be more problematic to treat and only case reports provide guidance for management of MDR-TB in pregnancy. First line drugs for the treatment of TB are all classified as pregnancy category C and can manifest different fetal side effects. In the treatment of pulmonary TB in pregnancy, INH, RIF, ETB and PRZ are recommended but in the case of central nervous system TB there are only case reports to use as a guide.
Main difference in our case, this patient had INH and RIF resistant TBM; therefore, we started the patient on Levofloxacin + Amoxicillin/Clavulanate + Ethambutol + Pyrazinamide promptly. Even though our patient was on her third trimester, the following must be closely monitored: MDR-TB's effects on both the mother and the fetus, both ETB and PRZ can be found in the mother's milk and what effects can these drugs do to a newborn and lastly PRZ caused jaundice.
In literature there a high complication incidence in TBM cases, including tuberculoma, hydrocephalus, encephalomyelopathy, radiculomyelitis, and cranial nerve palsies. In 6-47% of the TBM cases a cerebral infarct can be seen [12-14].
Pathophysiological the necrotizing panarteritis and secondary thrombosis due that in the small and medium sized arteries of the brain causes these infarcts. In our case, multiple nonspecific hyper-intense gliotic lesions in the both cerebral hemispheres on the corona radiata level are seen in the MRI. Accompanying that on the left cerebral hemisphere next to the posterior horn of the inferior parietal lobe a chronic parenchymal encephalomalezia and gliozis area are seen. With these MRI signs we started dexamethasone and low molecular weight heparin in the early stages of the disease.
We think that because our patient was diagnosed and hospitalized early, adherence to the treatment was not a problem. This is one of the criteria that sets our case apart. With a nearly successful treatment which is still ongoing we present a difficult case of MDR-TBM.