Polycystic kidney disease is a multisystemic familial inherited disease. A symptomatic treatment approach is the standard modality for autosomal dominant polycystic kidney disease (ADPKD) complications and life-long 50% chronic renal failure risk, as renal transplantation is the only definitive treatment. We aimed to explain the anesthesia management of our patient who had an 18 kg cyst removed. There are various complications that; include hypertension, urinary tract infections, hematuria, pain due to solid organ compression, liver cysts, and hernias. Comprehensive preparation, including detailed anamnesis and physical examination, communication and multidisciplinary evaluation, are essential to prevent morbidity and mortality.
Polycystic kidney disease, Renal failure
ADPKD: Autosomal Dominant Polycystic Kidney Disease; PKD: Polycystic Kidney Disease; PKD-1: Polycystic Kidney Disease-1; PLD: Polycystic Liver Disease; ECG: Electrocardiography; ASA: American Society of Anesthesia; IV: Intravenous; MOY: Multiple Organ Failure; ARDS: Acute Respiratory Distress Syndrome; DIC: Disseminated İntravascular Coagulation
Polycystic kidney disease (PKD) is a multisystemic familial inherited disease, which includes its autosomal dominant polycystic kidney disease (ADPKD) form and recessive form [1].
Its recessive form is often seen in pediatric patients and symptomatic in childhood, while the dominant form may be asymptomatic up to adulthood [2]. The autosomal dominant form has an incidence of one per 1000 live births, and its most common transmission occurs due to "Polycystic Kidney Disease-1" (PKD-1) ve "Polycystic Kidney Disease-2" gene families. In this form, the disease is generally compensated to the fifth decade, and patients are usually diagnosed with acute kidney disease upon their first admission. Incidentally, early diagnosis may be observed in patients whose abdominal imaging for other pathologies were requested and those whose scanning was ordered due to known familial history.
A symptomatic treatment approach is the standard modality for ADPKD's complications and life-long 50% chronic renal failure risk, as renal transplantation is the only definitive treatment. Renal replacement therapy must be utilized for patients on the waiting list or those not candidates for transplantation [3]. Intracranial bleeding due to aneurysms and long-term renal failure complications, including hypertension, dyslipidemia, and proteinuria, are the leading causes of mortality among ADPKD patients. Liver involvement is the most frequently seen extrarenal manifestation of ADKPD. Polycystic liver disease (PLD) is a hereditary condition characterized by multiple biliary system-originated cycs in the liver parenchyma. PLD is not limited to as a component of ADPKD (MIM173900 and MIM173910 gene mutations) and may be seen as a separate entity from patients without ADPKD. Any renal involvement may be diagnosed with PLD due to a different mutation pathway (MIM174050 gene mutation) [1]. With age, a general increase in count and size of liver cysts are expected, with %80 of patients over 60 years being diagnosed with liver cysts [3].
In this case presentation, we planned to discuss anesthetic management of an ADPKD with bilateral nephrectomy and hepatic cyst resection. Written and informed consent was obtained from the patient "for the publication of this Case Report".
A sixty-nine-year-old male patient (107 kg, 174 cm, Body Mass Index: 35.3) was on follow-up with end-stage renal failure secondary to ADPKD. The patient has been on a once peer weekly dialysis program for the last year, performed via the brachial arteriovenous fistula. Excluding anemia (Hemoglobin 10.3 mg/dL) and elevated creatinine level (Creatinine 8.6 mg/Dl), both attributed to chronic renal disease and dialysis, his laboratory results were average. His medication plan included an Alpha-adrenoreceptor antagonist, dihydropyridine calcium channel blocker, methyldopa, HMG-CoA reductase inhibitör, and xanthine oxidase inhibitor. Desaturation (SpO2 %86-88) was seen in the prone position, and the patient's other vitals were found within average values. A pulse rate of 87/min was observed in electrocardiography (ECG) in sinus rhythm. No pathological findings were present on the chest X-RAY, and the echocardiography revealed an ejection fracture of %59 and left ventricular concentric hypertrophy. The patient was given a Mallampathy score of IV and classified as American Society of Anesthesia (ASA) III. The local ethics committee approved the study, the patient gave informed consent to it, and written approval was received. Due to progressive mass effect, abdomen distention (Figure 1), and organ dysfunction, the patient was scheduled for bilateral nephrectomy and hepatic cyst resection.
 Figure 1: Preoperative and postoperative abdomen photography.
View Figure 1
Figure 1: Preoperative and postoperative abdomen photography.
View Figure 1
After standard monitorisation, heart rate of 110/min and blood pressure of 170/105 mmHg were noted, with the other vitals deemed normal. 2.5 mg midazolam was given intravenously (IV) for premedication, and 2 gr cephazolin was used as prophylaxis. An IV dosage of 1 mg/kg lidocaine, 2 mg/kg propofol, 1 mcg/kg fentanyl and 0.6 mg/kg rocuronium was utilized for induction of anesthesia. After preoxygenation, the patient was intubated and connected to the ventilator without any complications. The tube placement was confirmed with end-tidal carbon-dioxide monitorisation. A video laryngoscope was on site in case of difficult intubation during the process. Maintenance of anesthesia was done by 2.2 MAC sevoflurane and IV infusion of remifentanil and rocuronium. The central catheter was placed in the right jugular vein by ultrasonography guidance for central access. After Allen test negativity was confirmed, the right radial artery was cannulated for invasive monitorisation. Intermittent arterial blood gas sampling and central venous pressure measurement were performed. Precautions for hypothermia were taken, and in case of hemorrhage, blood and blood products were prepared. Hypotension with the average arterial blood pressure below 65 mmHg was observed at the second hour of operation, and IV noradrenaline infusion was initiated. Bilateral nephrectomy and hepatic cyst resection were successfully performed, with the total mass weight removed being 18 kg (Figure 2 and Figure 3).
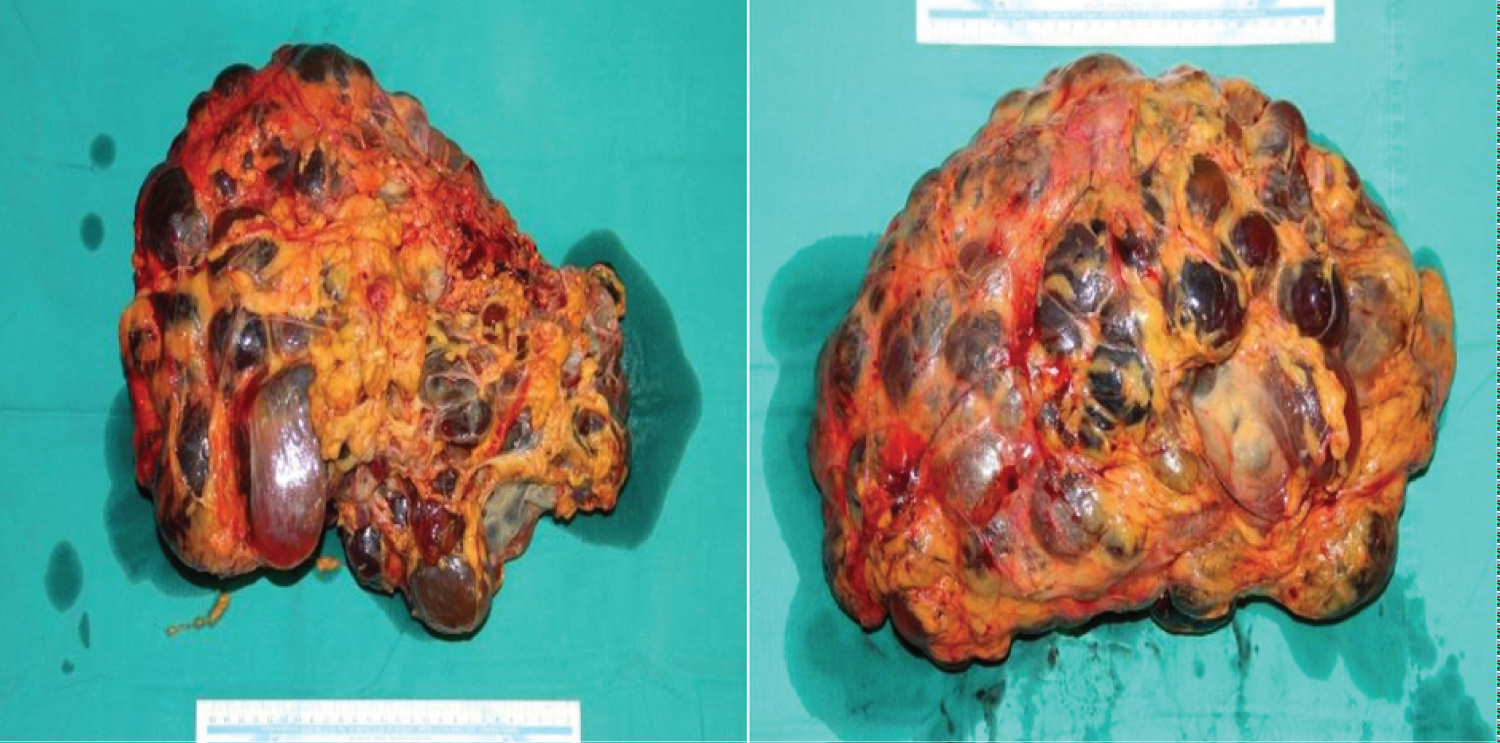 Figure 2: Nephrectomy materials.
View Figure 2
Figure 2: Nephrectomy materials.
View Figure 2
 Figure 3: Resected hepatic cysts.
View Figure 3
Figure 3: Resected hepatic cysts.
View Figure 3
The patient's respiration pattern and peak inspiratory pressure improved after resection. The operation lasted for 4 hours, with 3000 ml balanced solution and 500 ml % dextrose (in which 5% albumin was present) as IV fluid maintenance. 200 mg sugammadex was utilized for neuromuscular blockade reversal. The patient was extubated after confirmation of spontaneous respiration with sufficient tidal volume and spontaneous opening of the eyes (Figure 1). Afterwards, 100 mg tramadol IV and patient-controlled analgesia with morphine infusion were prepared for pain management. The patient was then transferred to the intensive care unit without any complications.
Autosomal dominant polycystic kidney disease (ADPKD) is the most common life-threatening single gene-disease, and its frequency is between 1/500 and 1/1,000 [1,2]. It is characterized by an increase in the volume of the kidney with renal and extrarenal fluid-filled cyst formation, a decrease in GFR, and the inability of kidney function. In general, they present with end-stage kidney disease in the 40-70th year of life and become candidates for kidney transplantation. However, they have to go to a unilateral or bilateral nephrectomy because there is insufficient space for the graft kidney.
There are various complications associated with ADPKD. These; include hypertension, urinary tract infections, hematuria, pain due to solid organ compression, stroke symptoms due to intracranial aneurysm rupture, liver cysts, and hernias. In addition, mortal complications that progress to intra-abdominal sepsis due to infection, abscess, and rupture of cysts can also be observed [1,4]. Zahir, et al. [4] presented a 52-year-old female patient known to have bilateral polycystic kidney disease with end-stage renal disease. The patient applied with a septicemia diagnosis, and ruptured infected cysts were observed in the laparotomy. The patient who developed multiple organ failure (MOY), acute respiratory distress syndrome (ARDS), and disseminated intravascular coagulation (DIC) was discharged from the intensive care unit on the postoperative 20th day.
Hypertension is a severe complication of ADPKD because of increased RAAS activity, and effective treatment is essential to reduce morbidity and mortality in ADPKD patients. Our patient also had uncontrolled hypertension despite multiple antihypertensive medications in the preoperative period. After monitoring the patient, blood pressure (BP) was measured as 170/105 mmHg. Due to increased glomerular filtration rate and changed volume status, titration should administer anesthetic drugs, and caution should be exercised in sudden hypotension. After induction of anesthesia, the patient's blood pressure could be kept at optimal values with the appropriate depth of anesthesia, but hypotension developed in the patient after removing organs filled with giant cysts. After adequate intravascular volume was achieved by avoiding fluid overload, the patient was started on noradrenaline infusion, and the mean arterial pressure was kept within average values. In addition to PKD, our patient also had giant liver cysts (figure liver). PLD is typically asymptomatic, but symptoms become more common with advancing age with dialysis and transplantation facilities. Common complications related to masses or cysts are hepatomegaly, portal hypertension, ascites, portal vein, vena cava compression, jaundice, bleeding, shortness of breath, early satiety, weight loss, gastroesophageal reflux, and pain in the lumbar region [1,3]. Due to delayed gastric emptying because of mass effect and gastroesophageal reflux, the patient was considered to have a full stomach, and aspirators were prepared before intubation. Our patient's preoperative saturation values ranged between 86-88% due to increased atelectasis, decreased functional residual capacity, and lung compliance due to mass compression. After being taken to the operating table, preoxygenation was provided by giving the ramp position. Considering the possibilities of difficult intubation and aspiration, we intubated the patient with a video laryngoscope.
In the light of the literature, ADPKD is a familial single gene mutation, and anesthesia management has been reported in a few cases before. However, massive 18-kg kidney and liver cysts were removed in our case, and it is the second-largest cyst excision after Ekser, et al.'s [5] 22-kg nephrectomy.
In conclusion, the anesthetic management of ADPKD requires considerable attention; the patient's vital signs, volume status, and depth of anesthesia should be well evaluated. Comprehensive preoperative preparation, including detailed anamnesis and physical examination, communication with the surgical team, and multidisciplinary evaluation, are essential to prevent morbidity and mortality, reducing the length of hospital stay and cost.
CY: This author helped in the anesthesia administration, follow-up, and writing of the case; ME: This author helped in the anesthesia administration and writing of the case; NC: This author took part in determining the anesthesia method of patients, patients’ follow-up, and case presentation controls.
None.