Ameloblastomas are rare benign tumours. Their management can be a contentious issue due to the high risk of recurrence in some histological subtypes. We present a case of a 16-year-old boy with an ameloblastoma of his right body and ramus of the mandible. Presentation, surgical work-up and management are discussed.
Ameloblastoma, Recurrence, Management
Ameloblastomas are benign, locally invasive, polymorphic neoplasms that consist of proliferating odontogenic epithelium (usually of a follicular or plexiform pattern) lying in a fibrous stroma [1]. They are known to have a high recurrence rate and are sometimes managed aggressively with radical surgery which usually involves wide resections and free flap reconstruction. Here we present a case report illustrating that certain variants of ameloblastomas have less likelihood of recurrence hence conservative management can be a reasonable approach.
A 16-year-old boy was referred to our maxillofacial department with a swelling over the right body and ramus of his mandible. It had been gradually increasing in size over the past 3 months. There was pain on biting but no dysaesthesia to the lip or chin, discharge or altered occlusion.
On examination, he had a golf ball size swelling in the right side of his mandible. It was firm and non-tender with no associated lingual swelling.
An orthopantomogram (OPG) (Figure 1) showed a large radiolucent area in the right mandible extending from the lower right second premolar to the base of the coronoid process encompassing most of the ramus. The lower right second and third molars were encased in the lesion with root resorption of the lower right first molar.
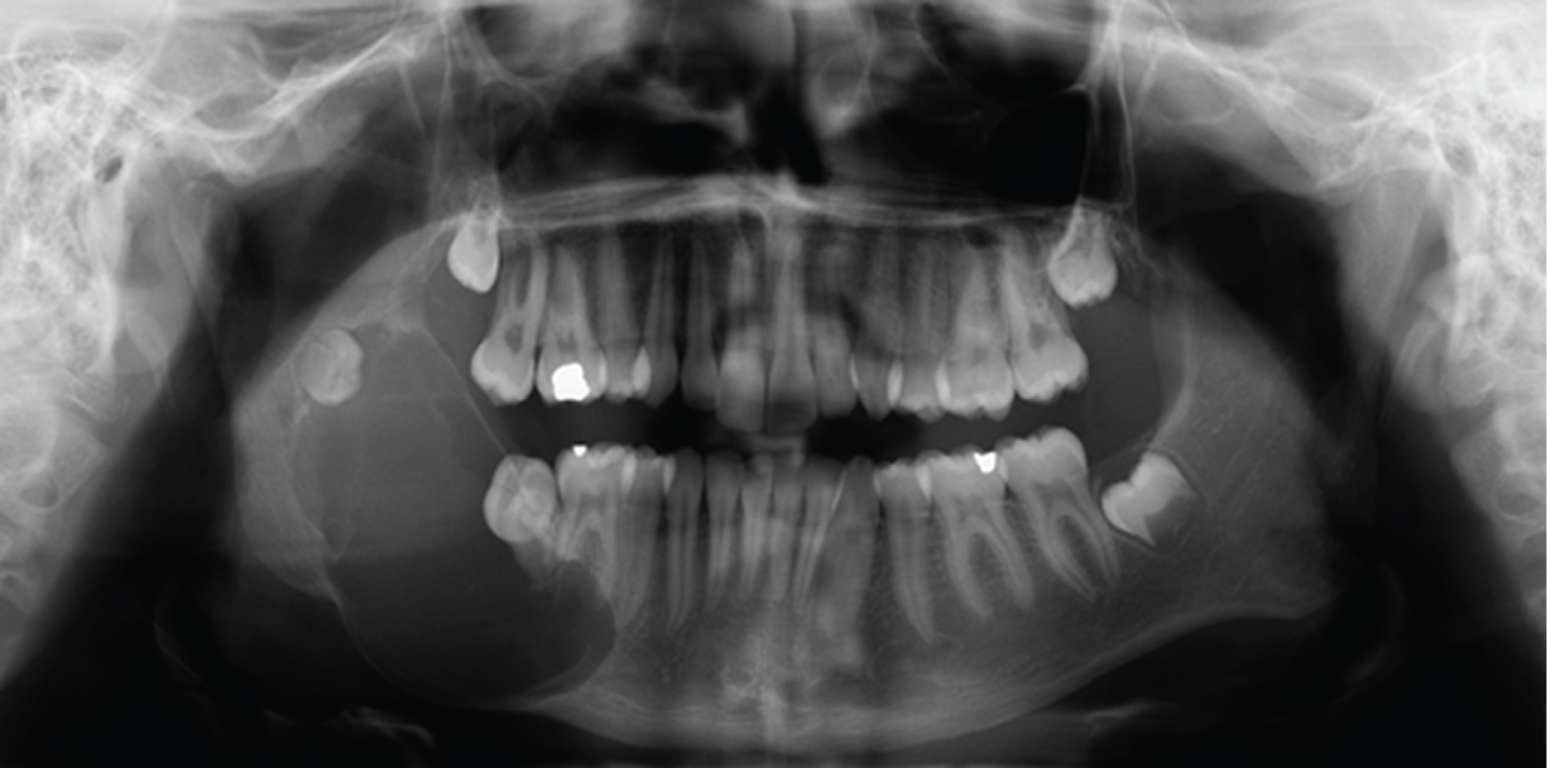 Figure 1: OPG on initial presentation, prior to enucleation. View Figure 1
Figure 1: OPG on initial presentation, prior to enucleation. View Figure 1
The CT showed an expansive cyst measuring 54 × 36 × 33 mm (Figure 2). There was resorption of the roots of the lower right first molar, displacement of the lower right second molar with the cyst emanating from the crown and of the lower right wisdom tooth. The radiological features were suggestive of a dentigerous cyst.
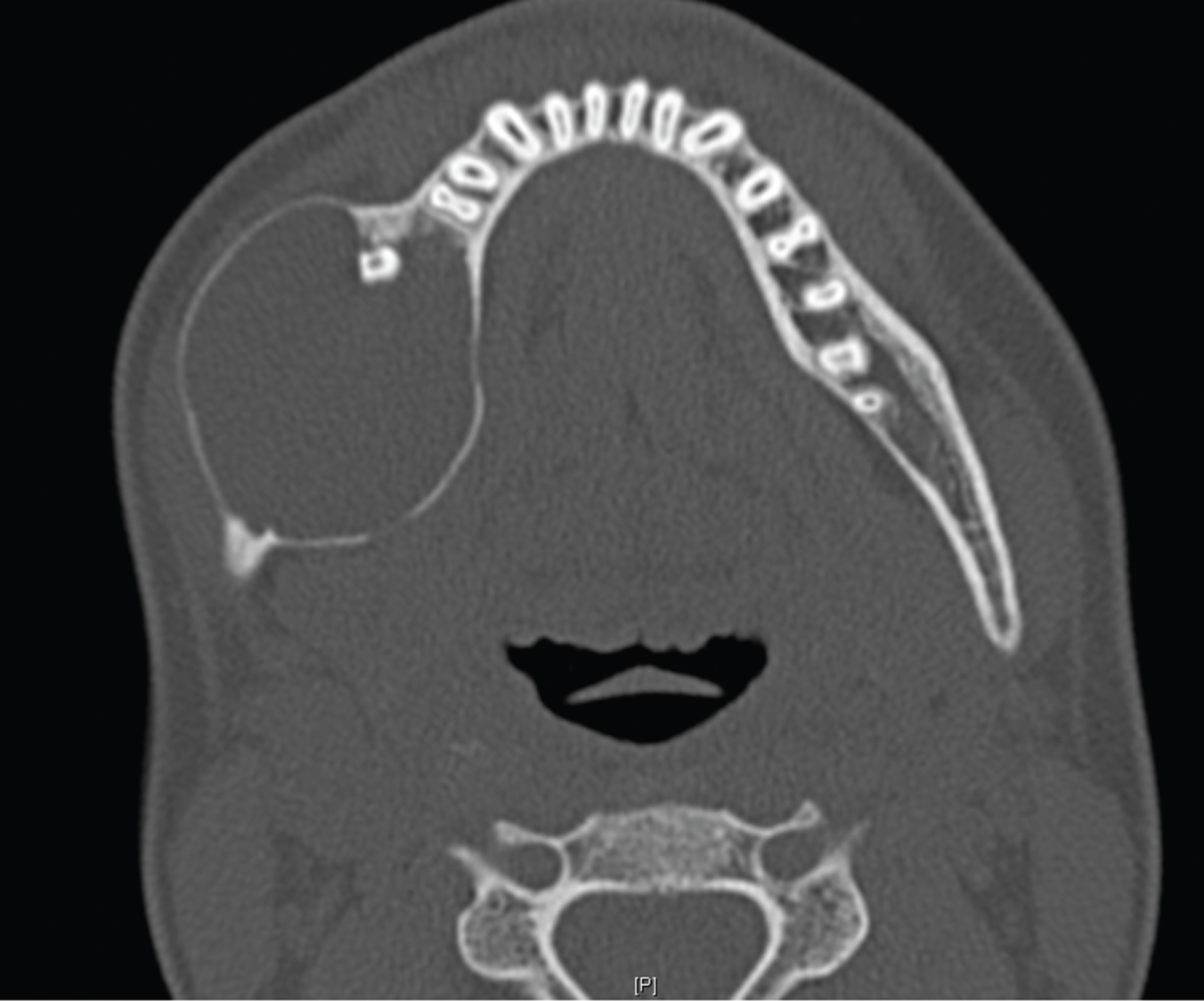 Figure 2: Initial presentation on CT. Well corticated expansile cyst right mandible. View Figure 2
Figure 2: Initial presentation on CT. Well corticated expansile cyst right mandible. View Figure 2
The patient had an enucleation of the lesion with removal of the lower right wisdom tooth. The lower right first and second molars were left in situ as the working diagnosis was a dentigerous cyst. However, the histopathology from first enucleation was suggestive of a unicystic ameloblastoma.
Serial OPGs post-operatively showed evidence of new bone formation with a well-defined lower border of mandible. At 12 months, there was evidence of recurrence on OPG (Figure 3). A CT mandible showed a cystic lesion measuring 24.4 mm (Figure 4). He was offered a resection with reconstruction or a further enucleation. The latter may require multiple operations under general anaesthetic. He opted for a second enucleation of the recurrent lesion. The histopathology showed a unicystic plexiform ameloblastoma.
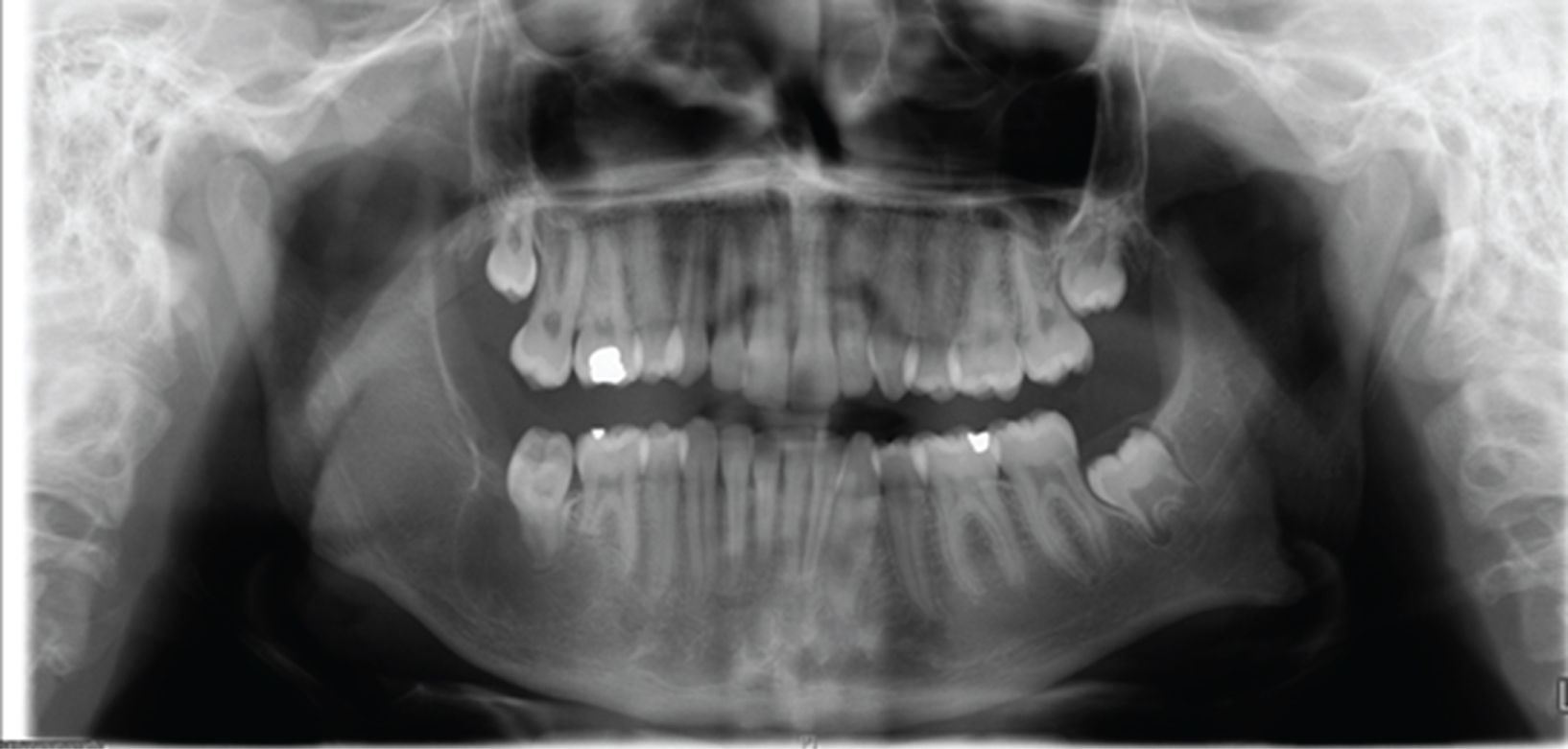 Figure 3: OPG at 12 months showing evidence of recurrence in right mandible. View Figure 3
Figure 3: OPG at 12 months showing evidence of recurrence in right mandible. View Figure 3
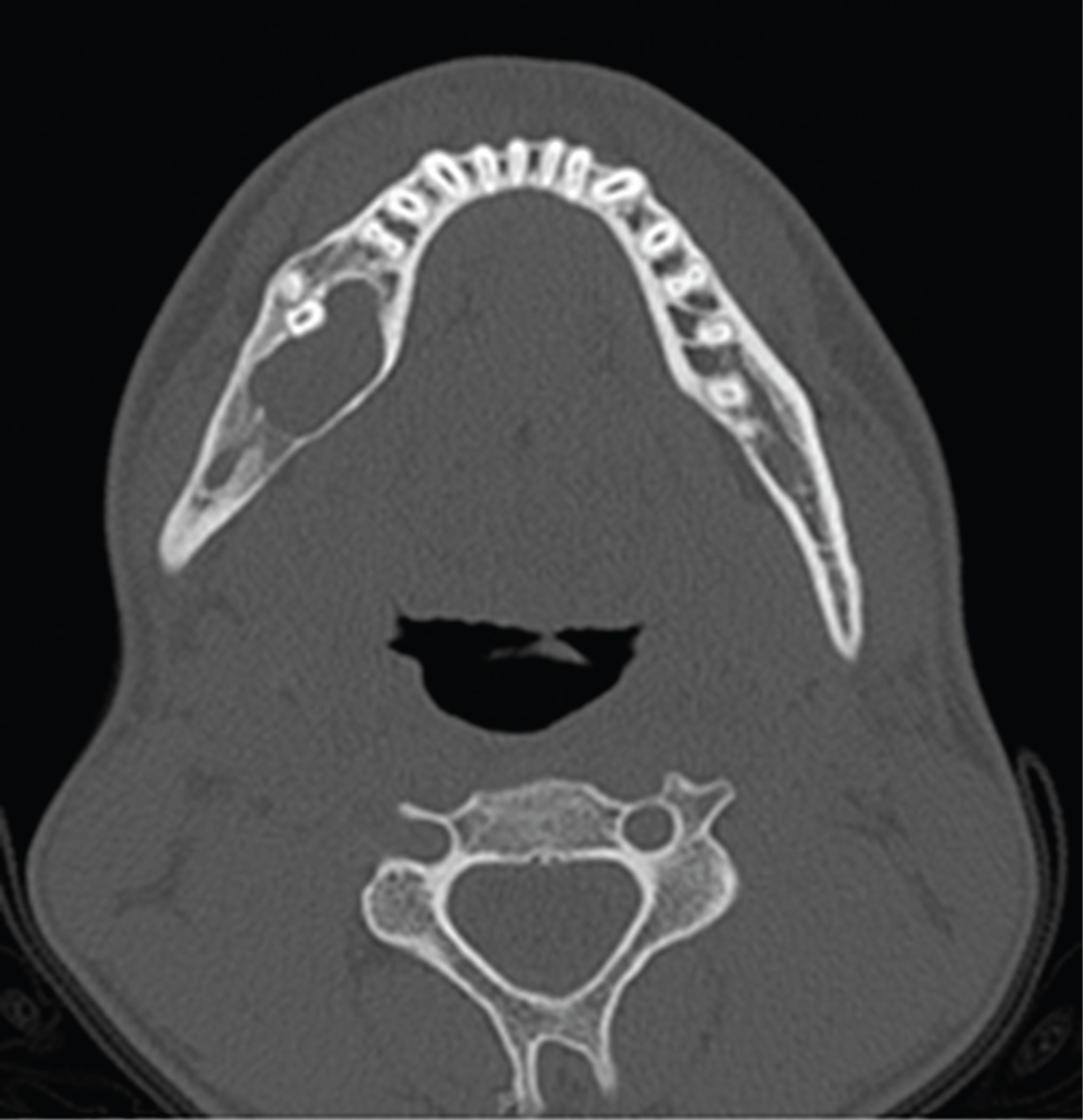 Figure 4: CT mandible at 12 months. Lesion measuring 24.4 mm at greatest dimension. View Figure 4
Figure 4: CT mandible at 12 months. Lesion measuring 24.4 mm at greatest dimension. View Figure 4
At 23 months from initial enucleation, a CT Mandible showed a cystic cavity 22 mm in maximum diameter with root resorption of the lower right first and second molars which were not mobile clinically (Figure 5). He underwent a third enucleation with extraction of the lower right first and second molars.
 Figure 5: CT mandible at 23 months after 2 enucleations. Lesion right mandible measures 22 mm in greatest dimension. View Figure 5
Figure 5: CT mandible at 23 months after 2 enucleations. Lesion right mandible measures 22 mm in greatest dimension. View Figure 5
At 33 months follow-up, the OPG (Figure 6) showed significant bone healing with no evidence of residual tumour. There is no paraesthesia to the lower lip and chin.
 Figure 6: OPG at 33 months post 2 enucleations. No evidence of residual disease. View Figure 6
Figure 6: OPG at 33 months post 2 enucleations. No evidence of residual disease. View Figure 6
This case report displays a conservative approach to managing ameloblastomas. This helps to preserve function and obviates or delays the need for radical surgery. Several studies have recommended conservative management depending on the macroscopic and radiological appearances [2-6].
There are 4 known types of ameloblastomas which are categorized according to their macroscopic appearances. These include solid/multicystic, extraosseous/peripheral, desmoplastic and unicystic types. The solid/multicystic type is slow growing and locally invasive. Histologically, it can show a plexiform or follicular pattern. Recommendation is to treat these radically due to high risk of recurrence of 50% during the first 5 years post-operatively [2,7]. The extraosseous/peripheral type is more uncommon and displays a less aggressive behaviour, hence conservative excision is the treatment of choice. The desmoplastic type displays a mix of radiolucent and radiopaque findings with diffuse margins. Radical treatment is recommended for this variant. Lastly, the unicystic type is associated with an unerupted 3rd molar 80% of the time hence radiologically gets misdiagnosed as a dentigerous cyst as was done in the case of our patient. The unicystic type has two histological appearances - luminal and mural. The luminal variant does not tend to infiltrate the cyst wall or surrounding bone, hence enucleation is sufficient. However, the mural variant infiltrates the cyst wall with possible bony invasion, hence radical treatment may be necessary [7].
Conservative approaches include marsupialization or enucleation with or without Carnoy's solution. Haq, et al. reported a series of 31 patients treated for mandibular ameloblastomas [6]. Four patients were treated by resection of the mandible and the remainder 27 patients underwent enucleation and application of Carnoy's solution. Of the 3 patients who had a recurrence, one was unicystic and 2 were solid/multicystic. None of the unilocular lesions as seen on radiograph recurred irrespective of histological subtype. Haq, et al. also state that it can sometimes be difficult to obtain a representative biopsy specimen as was the case in 4 of the 31 patients where diagnosis was altered when the main specimen was evaluated. Hence, resection in these cases would have resulted in serious consequences. They hence propose that the radiological appearance should guide management of ameloblastomas more than the histological result.
Nakamura, et al. compared the long-term results between different approaches to 78 patients with ameloblastomas [3]. They found that conservative treatments including marsupialization and enucleation followed by sufficient bone curettage were useful and reduced the need for jaw resection.
Historically, ameloblastomas were enucleated, however with the emergence of reliable microvascular reconstruction, it is not uncommon for surgeons to manage ameloblastomas with wide local resections and free flap reconstructions. However, radical treatment can leave major aesthetic and functional consequences in a relatively young group of patients (average age 36 years) [2], hence the choice of conservative versus radial treatment needs careful discussion with the patient.
Radical surgery consists of segmental bone resection or wide local excision of 10 to 20 mm margins with reconstruction, usually in the form of a free flap. Hong, et al. studied the long-term outcome on 305 patients with ameloblastomas and found significant differences in disease-free survival between those treated conservatively versus those who underwent resection with bone margin or segmental resection [5]. They advocate resection with a safety margin as the best method of management of ameloblastomas. However, in those with unicystic or plexiform ameloblastomas, conservative treatment is a reasonable approach.
The premise behind radical or segmental resection of ameloblastomas is due to its high recurrence rate. Muller, et al. conducted a systematic review and compared this with their series of 84 patients followed-up for at least 5 years [8]. They showed a recurrence rate of 75% in cases of multilocular ameloblastomas treated conservatively but only 15% in those treated by radical surgery. The recurrence rate was lower (20%) in unilocular ameloblastomas. Ueno, et al. studied 91 patients with ameloblastomas and found a 8.7% recurrence rate in those treated with radical surgery compared with 45.6% recurrence in those treated conservatively [9]. The recurrence rate was higher in the follicular than plexiform types and again as with Muller, et al. they also found higher recurrence rates in the multilocular than unilocular types.
A possible criticism in the management of our patient could be the lack of tooth extractions at initial enucleation. Normally, teeth showing involvement with, Although there appears to be an ongoing debate in the management of ameloblastomas, there is sufficient evidence to show that treatment should be based on the histological subtype. It is generally accepted that the small unicystic variants are less likely to recur and can be managed by enucleation. However, as many present as large lesions on presentation, surgeons choose the more radical approach of jaw resection. We question whether mandibular ameloblastomas merit such an aggressive approach. It seems entirely reasonable to proceed with repeated enucleations when a recurrence occurs as these tend to be localised and contained within the mandible. If patients are followed up closely with serial OPGs, recurrences can then be caught early and treated conservatively with minimal patient morbidity. In our case, we intend to follow-up our patient every 6 months with serial OPGs.
None.
None.
Not required.
None.