Several parameters are important to evaluate good oncological and functional results after robotic prostatectomy. We hypothesize that preservation or reconstruction of Retzius space can be valuable for better results outcomes, especially in terms of early continence recovery.
In October 2018, electronic searches were conducted in the following databases: Cochrane, EMBASE, PubMed and Google Scholar. Manual searches in the reference lists of all the reviews and the relevant studies were identified. Searches of abstracts of relevant congresses were made. To locate additional studies, experts in the field were contacted (Supplementary Table 1).
Table 1: Summary of all studies about Retzius-sparing robot-assisted radical prostatectomy. View Table 1
Randomized controlled trials and observational studies comparing RS X anterior approach or RSR X anterior approach for the treatment of patients with localized prostate cancer were selected.
We included 8 studies: Two randomized controlled clinical trials, three retrospective observational studies and three prospective observational studies.
In the RS-RARP group, the overall continence recovery in 1-2 weeks or 10 days or immediately after surgery was significantly faster compared to the conventional anterior approach (random effect (RE): OR = 4.17; 95% CI: 2.14-8.14; p < 0.0001).
Between the two groups in both stages pT2, there were no significant differences (RE: OR = 1.06; 95% CI: 0.62-1.81; p < 0.83 and pT3 stages (RE: OR = 1.33; 95% CI: 0.66-2.66; p < 0.42).
Between RS group and conventional anterior approach, there were no significant differences (RE: OR = 0.98; 95% CI: 0.51-1.90; p < 0.96). In the RS group compared to the previous conventional, the urinary function (IPSS) was significantly higher.
The RS-RARP group had a faster continence recovery compared to C-RARP, while we found no difference in terms of long-term urinary function or oncological outcomes.
Prostate cancer is the leading cause of death among men in industrialized countries due to oncological causes and prostate-specific antigen (PSA) screening for it is common in many countries around the world [1] is the second most common cancer and the sixth cause of cancer in men [2]. The presence of negative surgical margins, continence and erectile dysfunction are the most relevant issues for patients undergoing RARP [3].
The "pentafecta" outcomes defined the best possible scenario for radical prostatectomy. Consisting in: Absence of early complications, no positive surgical margins (PSM), continence recovery, sexual potency and absence of biochemical recurrence [4].
At the beginning of 2010, Galfano, et al. described the Retzius Sparing (RS) procedure, which allows the possibility of performing completely intrafascial prostatectomies. This technique retains the complete anatomical integrity of the "Aphrodite's veil", which contains the neurovascular bundles. Good functional results can be expected in patients undergoing a high intrafascial procedure, since several studies report the presence of nerve structures within the higher characteristics of the Aphrodite veil and the endopelvic fascia.
With the standard RALP procedure as well as with intrafascial approaches preserving Aphrodite's veil, the higher aspect of the veil has to be opened. In contrast, with the Bocciardi approach, the veil does not have to be opened at any point, providing a strong rationale for obtaining better results [5]. The preservation of the bladder neck, the preservation of the prostatic fascia among other reconstructive techniques and the total anatomical reconstruction seems to improve continence [6]. Other techniques related to the development of continence are the complete reconstruction of the Retzius space, also reducing the early and late perioperative complications [7].
The technique Retzius-Sparing (RS-RARP) in which the approach is posterior and is completely intrafascial, technically more challenging than the conventional technique, in this approach the parietal peritoneum is incised for 5-7 cm on the anterior surface of the Douglas pouch. The seminal vesicles and the vas deferens are isolated. An intrafascial plane is maintained (with complete nerve preservation whenever possible and oncologically safe). In case of adhesions, palpable disease, the surgeon will choose to follow a wider dissection plan. The vesicoprostatic junction is recognized, isolated and sectioned; the bladder neck is preserved when reasonably safe. The forward surface of the prostate is blunt dissected and isolated from the Santorini plexus without incision. The apex isolation is completed and the urethra is incised. The anastomosis is performed using a adapted Van Velthoven suture from 12 o'clock. This technique results in the preservation of all structures located in the Retzius space, such as; endopelvic fascia, Santorini plexus, pubovesical ligaments and accessory pudendal arteries. Rates of complications are relatively comparable and continence is quicker [8].
In the reconstructive technique (RSR), the Retzius space is opened, dissection of the bladder is performed, conventional technique of robotic prostatectomy is performed, the endopelvic fascia is opened and the dorsal venous complex is secured, neurovascular bundle preservation, prostate removal, anastomosis and subsequent closure of the Retzius space, closing the peritoneum thus relocating the bladder to the anterior abdominal wall and, the continence recovery was significantly faster in the RSR group compared to patients without reconstruction [9].
We led this meta-analysis and review of the literature. Evaluate the effectiveness and the postoperative outcomes of radical prostatectomy assisted by the robot that retains Retzius (RS-RARP) and Retzius space reconstruction technique (RSR-RARP) compared to conventional technique (C-RARP).
To evaluate the efficacy, effectiveness, safety and clinical, functional and oncological outcomes of Retzius sparing robot-assisted radical prostatectomy (RS-RARP) and Retzius space reconstruction technique (RSR-RARP) in comparison with the conventional or standard RARP (C-RARP) (Table 1).
1) Randomized controlled trials.
2) Comparative observational studies (including case series).
Patients with low-intermediate risk prostate cancer according to NCCN (National Comprehensive Cancer Network) Guidelines.
1) RS-RARP or posterior RARP.
2) Retzius space reconstruction RSR-RARP.
3) C-RARP or standard RARP or anterior RARP.
1) Continence recovery:
-Overall continence recovery at 1-2 week or 10 days or immediate post-op.
-Overall continence recovery at 4 weeks post-op.
-Overall continence recovery at 3 months post-op.
2) Positive surgical margins (PSMs):
-PSMs pT2.
-PSMs pT3.
3) Complications:
Complication rates.
4) Urinary function:
IPSS score at 3 months. Post-operation
Secondary outcomes:
1) Continence recovery:
-Overall continence recovery at 6 months post-op.
-Overall continence recovery at 12 months post-op.
-1 Pads/day at 4 weeks post-op.
-Time to urinary continence recovery.
2) Complications:
-Median operating time.
-Estimated blood loss.
-Length of stay.
Electronic searches: In October 2018, electronic searches were conducted in the following databases: Cochrane, EMBASE, PubMed and Google Scholar using the terms "Retzius-sparing", "posterior approach", and "robot assisted radical prostatectomy" were performed to identify studies published up to October 2018, comparing RS-RARP to C-RARP.
Searching other resources: Searches of abstracts of relevant congresses were made.
Selection of studies: PM and WP independently selected potentially relevant studies according to previously defined selection criteria. Disagreements were resolved by consensus.
Data extraction and management: After defining the studies to include and exclude by consensus, the following data were extracted from each study: First author, year of publication, study design, participants, interventions, average age of the participants, risk of bias, results and notes.
Assessment of risk of bias in included studies: To evaluate the risk of bias in the selected studies, we applied the tools of the Cochrane Collaboration, which assesses the risk of bias in six domains: Generation of sequences, concealment of allocation, blinding, incomplete results data, selective results reports and other potential biases.
Measures of treatment effect: For statistical analysis, we use Review Manager 5.3 provided by the Cochrane Collaboration. We summarized the dichotomous and continuous results in terms of odds ratios (OR) and with a standardized mean difference (SMD) with their 95% confidence intervals, respectively.
Among the trials that used the chi-squared statistic, heterogeneity was examined with a significance level of 0.10 and the I2 statistic. We considered moderate or high levels of heterogeneity at the I2 estimation above 50% and a sensitivity analysis was performed.
Assessment of reporting biases: We used a broad search strategy that included the evaluation of published and unpublished studies in order to reduce the risk of publication bias.
Data synthesis: The results were grouped when the interventions and populations had similarities and the differences were estimated using fixed and random effects models. In the absence of significant differences between the two models, the final results are presented using random effects models.
Sensitivity analysis: A sensitivity analysis was done in cases where the results were heterogeneous.
We included 8 studies: Two randomized controlled clinical trials, three retrospective observational studies and three prospective observational studies. We observed a sufficient similarity between the parameters in the studies. In all the studies, the RS-RARP and conventional procedures were compared. Dichotomous variables (recovery of continence, PSMs and complication rates) were comparable for the meta-analysis. The only study that reported data and results about recovery of potency after treatment with RS-RARP was Menon, et al. (See the Figure 1 Study flow diagram).
 Figure 1: Study flow diagram.
View Figure 1
Figure 1: Study flow diagram.
View Figure 1
Included studies: After reviewing 179 articles we determined that 8 studies met our inclusion criteria.
Excluded studies: We excluded 171 articles from the systematic review, for reasons such as the following: There was no comparison group, case report or series of cases, descriptive studies or narrative reviews.
Risk of bias in included studies: See Figure 2 Risk of bias graph and Figure 3 Risk of bias summary.
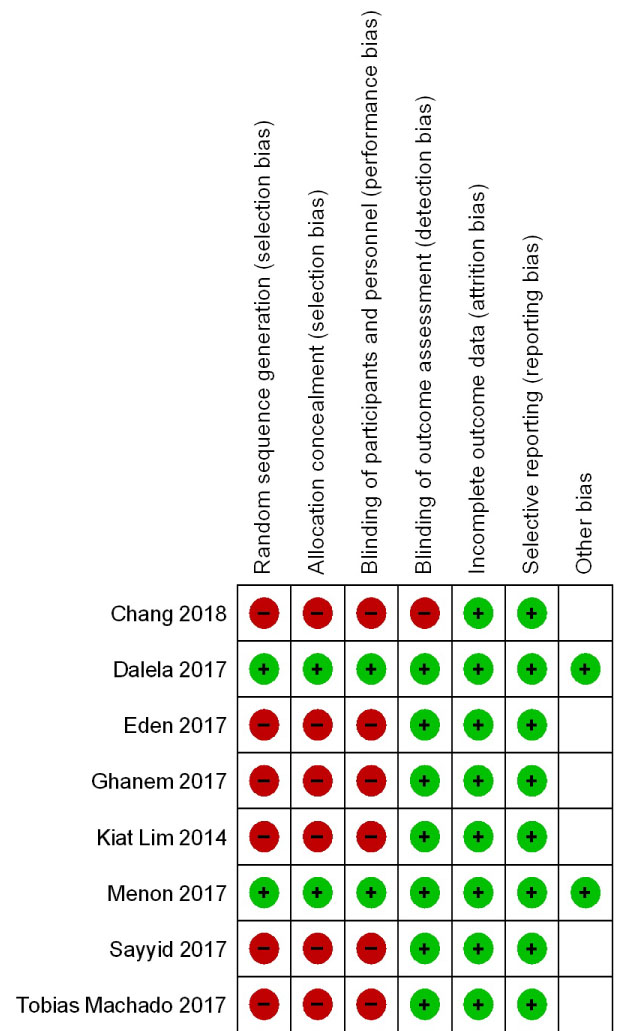 Figure 2: Risk of bias graph: Review authors' judgements about each risk of bias item presented as percentages across all included studies.
View Figure 2
Figure 2: Risk of bias graph: Review authors' judgements about each risk of bias item presented as percentages across all included studies.
View Figure 2
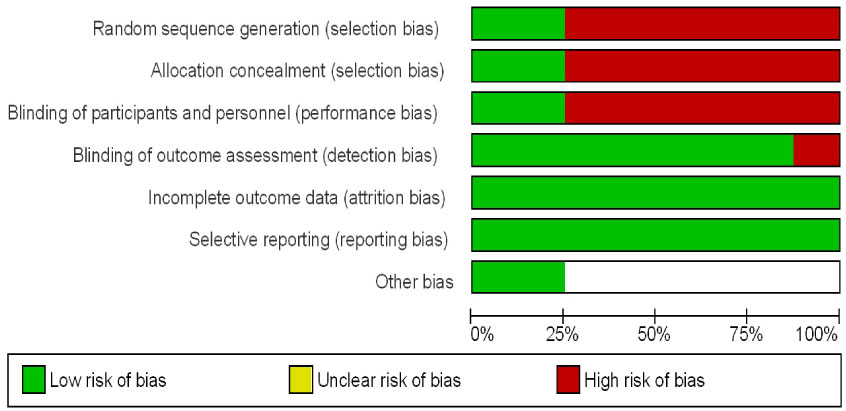 Figure 3: Risk of bias summary: Review authors' judgements about each risk of bias item for each included study.
View Figure 3
Figure 3: Risk of bias summary: Review authors' judgements about each risk of bias item for each included study.
View Figure 3
Continence Recovery: In the RS group, the overall continence recovery in 1-2 weeks or 10 days or immediately after the surgery (random effect (RE): OR = 4.17; 95% CI: 2.14-8.14; p < 0.0001, see Figure 4) was significantly faster and higher, respectively, compared to the conventional anterior approach.
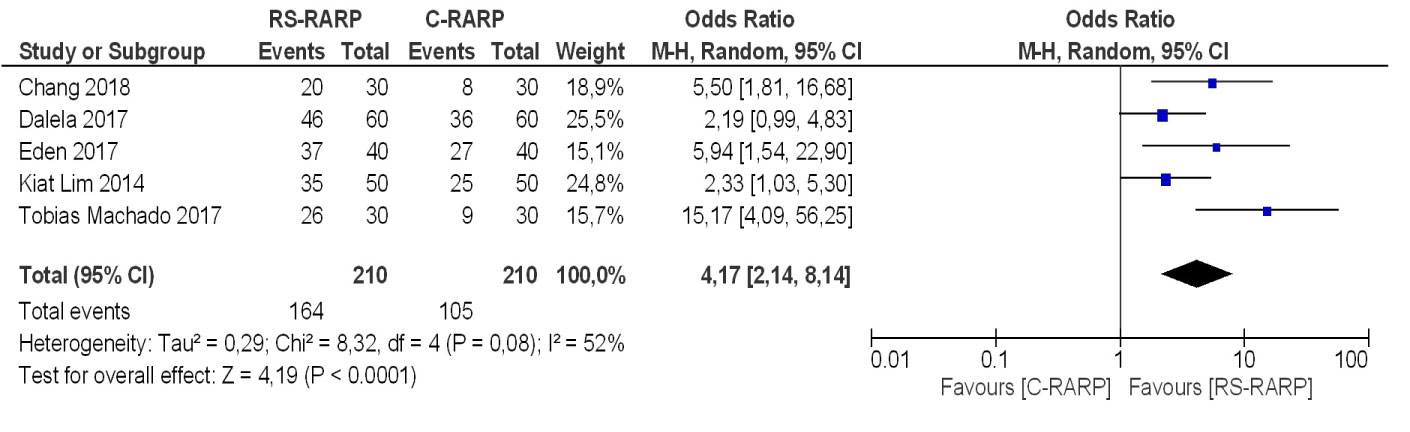 Figure 4: Forest plot of comparison: Continence recovery, outcome: Overall continence recovery at 1-2 week or 10 days or immediate post-op.
View Figure 4
Figure 4: Forest plot of comparison: Continence recovery, outcome: Overall continence recovery at 1-2 week or 10 days or immediate post-op.
View Figure 4
Similar results were found In the RS group, the overall continence recovery at 4 weeks post-op. after surgery (random effect (RE): OR = 4.61; 95% CI: 2.72-7.81; p < 0.00001, See Figure 5), In the RS group, the overall continence recovery at 3 months post-op. after surgery (random effect (RE): OR = 3.32; 95% CI: 2.07-5.32; p < 0.00001, see Figure 6).
 Figure 5: Forest plot of comparison: Continence recovery, outcome: Overall continence recovery at 4 weeks post-op.
View Figure 5
Figure 5: Forest plot of comparison: Continence recovery, outcome: Overall continence recovery at 4 weeks post-op.
View Figure 5
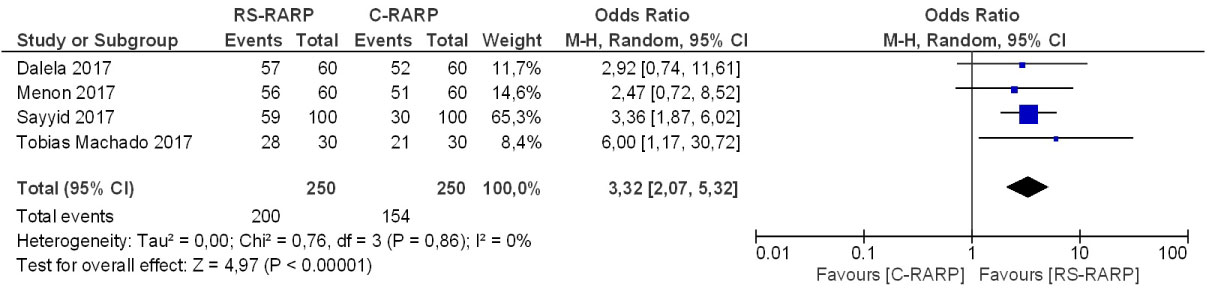 Figure 6: Forest plot of comparison: Continence recovery, outcome: Overall continence recovery at 3 months post-op.
View Figure 6
Figure 6: Forest plot of comparison: Continence recovery, outcome: Overall continence recovery at 3 months post-op.
View Figure 6
Overall continence recovery at 6 months post-op. after surgery (random effect (RE): OR = 3.70; 95% CI: 2.33-5.88; p < 0.00001, See Figure 7), In RS group, the overall continence recovery at 12 months post-op. after surgery was significantly faster compared to conventional anterior approach (random effect (RE): OR = 3.66; 95% CI: 1.17-11.46; p < 0.03, See Figure 8).
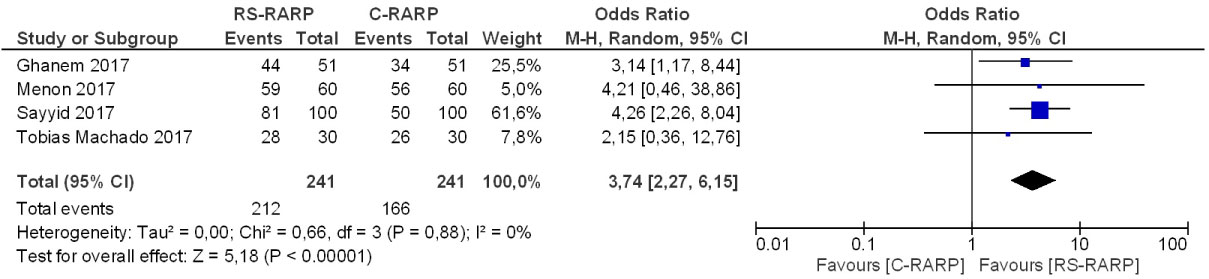 Figure 7: Forest plot of comparison: Continence recovery, outcome: Overall continence recovery at 6 months post-op.
View Figure 7
Figure 7: Forest plot of comparison: Continence recovery, outcome: Overall continence recovery at 6 months post-op.
View Figure 7
 Figure 8: Forest plot of comparison: Continence recovery, outcome: Overall continence recovery at 12 months post-op.
View Figure 8
Figure 8: Forest plot of comparison: Continence recovery, outcome: Overall continence recovery at 12 months post-op.
View Figure 8
There were no significant differences between the two groups in both stages pT2 (RE: OR = 1.06; 95% CI: 0.62-1.81; p < 0.83, See Figure 9) and pT3 stages (RE: OR = 1.33; 95% CI: 0.66-2.66; p < 0.42, See Figure 10).
 Figure 9: Forest plot of comparison: Positive surgical margins (PSMs), outcome: PSMs pT2.
View Figure 9
Figure 9: Forest plot of comparison: Positive surgical margins (PSMs), outcome: PSMs pT2.
View Figure 9
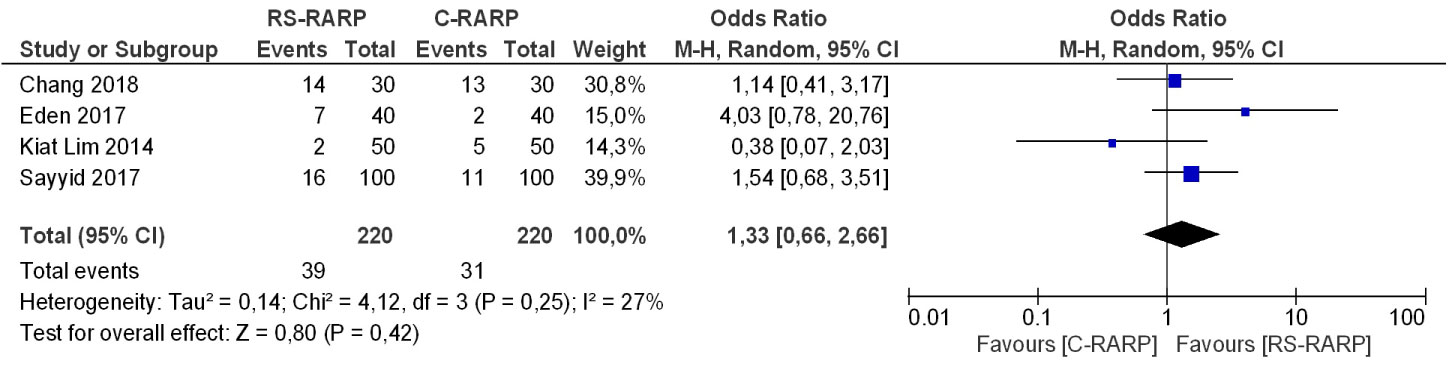 Figure 10: Forest plot of comparison: Positive surgical margins (PSMs), outcome: PSMs pT3.
View Figure 10
Figure 10: Forest plot of comparison: Positive surgical margins (PSMs), outcome: PSMs pT3.
View Figure 10
There were no significant differences between RS group and conventional anterior approach (RE: OR = 0.98; 95% CI: 0.51-1.90; p < 0.96, See Figure 11). There were no significant differences in the median operating time, in the estimated blood loss and in the length of stay, see Figure 12, Figure 13 and Figure 14 respectively.
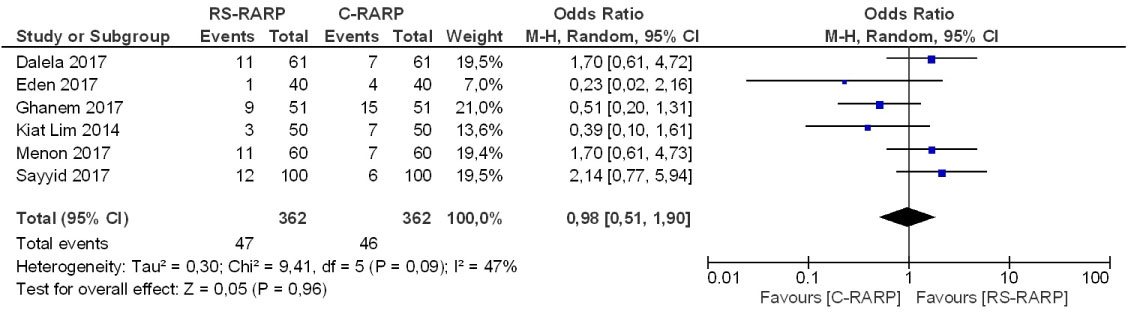 Figure 11: Forest plot of comparison: Complications, outcome: Complication rates.
View Figure 11
Figure 11: Forest plot of comparison: Complications, outcome: Complication rates.
View Figure 11
 Figure 12: Forest plot of comparison: Complications, outcome: Median operating time (min).
View Figure 12
Figure 12: Forest plot of comparison: Complications, outcome: Median operating time (min).
View Figure 12
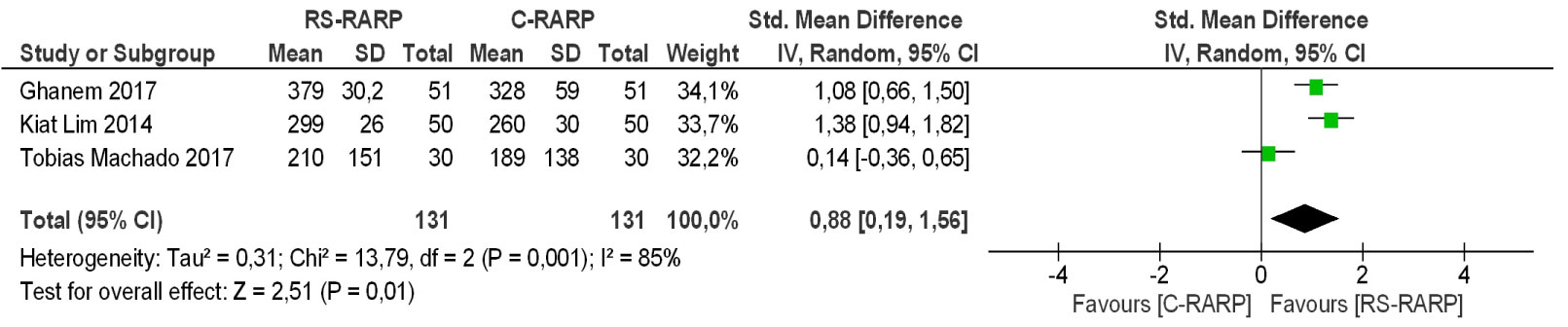 Figure 13: Forest plot of comparison: Complications, outcome: Estimated blood loss (ml).
View Figure 13
Figure 13: Forest plot of comparison: Complications, outcome: Estimated blood loss (ml).
View Figure 13
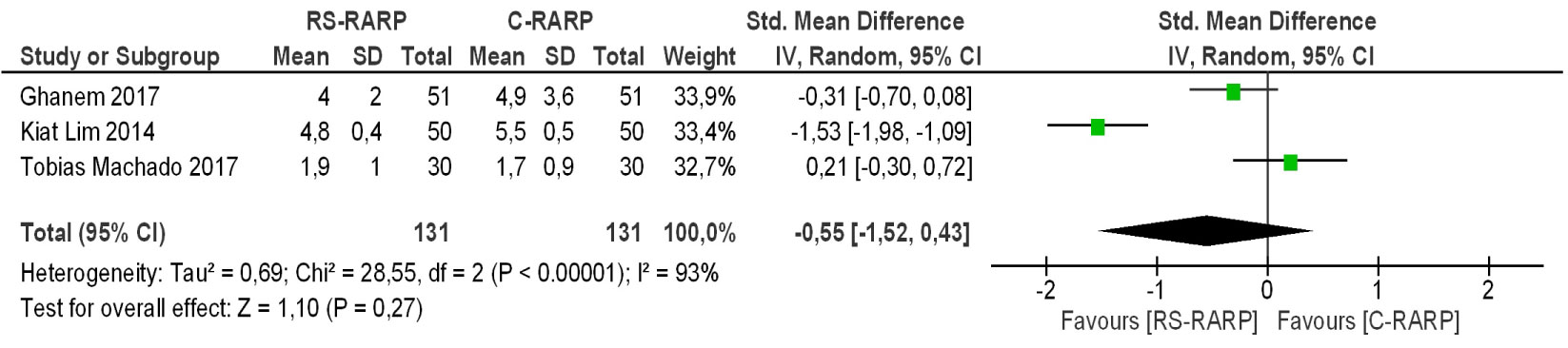 Figure 14: Forest plot of comparison: Complications, outcome: Length of stay (days).
View Figure 14
Figure 14: Forest plot of comparison: Complications, outcome: Length of stay (days).
View Figure 14
We assessed urinary function with the International Prostate Symptom Score (IPSS) at 3 months post-operation, graduating patients with mild, moderate and severe symptoms as was significantly favourable in RS group compared to conventional approach (RE: SMD = -0.25; 95% CI: -0.46 - -0.05; p < 0.01, See Figure 15).
 Figure 15: Forest plot of comparison: Urinary function, outcome: Mean IPSS score at 3 months.
View Figure 15
Figure 15: Forest plot of comparison: Urinary function, outcome: Mean IPSS score at 3 months.
View Figure 15
In recent years, various techniques have been developed in order to achieve a faster continence. In patients under RARP, the fastest continence rates are reached at 2 to 6 months after surgery. The 2017 Annual Report of Intuitive Surgical Inc. stated that Da Vinci prostatectomy had a significant increase in recent years [10]. The growth in the realization of this procedure motivates the need to innovate the techniques to improve specific results.
One of the limitations of the technique (RS-RALP) is the lack of global experience, therefore few preceptors to help teach this technique that is more challenging than the conventional one described at the beginning of this millennium, another limitation of the technique that It makes (RS-RALP) remain a little hidden is the small workspace that it offers compared to conventional technique, something that can make surgery difficult when the prostates are very large or very attached which sometimes obliges the surgeon to go for an extrafacial plane [9].
There were no statistically significant differences between the 2 techniques RS-RARP vs. C-RARP (RE: OR = 0.98, 95% CI: 0.51-1.90, p < 0.96), Galfano, et al. [5] in their first case report reported as complications 2 vesical perforations, in the second work of Galfano, et al. reported a complication due to prostate fossa bleeding which was re-operated, another patient with severe abdomen due to intestinal hernia through a lateral portal, another subject to embolization of a branch of the gluteal artery due to bleeding, 8 transfusions were required in group 1 and 4 in group 2 [8].
Concerning the work of Menon [11] the most common difficulty was symptomatic lymphocele that required percutaneous drainage, occurred in 9 of 120 patients (7.5%), a patient with RS-RARP required reoperation, and a patient with C-RARP required reintervention 3 months later due to an umbilical hernia, no urethral stenosis was existent in any patient.
In the paper of Ghanem [9] which compares conventional technique with reconstruction of the extra-peritoneal space of Retzius shows that general complications do not diverge in the 2 groups, only the hernias in the portals were lower in the RS-RARP technique compared with C-RARP.
As stated by Lim, et al. [12] no significant differences were observed regarding the length of hospital stay, bleeding and intra- and post-operative complications.
We can say that the more we practice this technique the more experience we will have, which could possibly lead to fewer complications.
PSM are uniformly associated with an increased risk of biochemical and local disease, are considered as an adverse result that could be associated with the failure of the surgery, could be an indicator of recurrence, as well as the need for secondary treatment after RARP. 1 PSM can also cause significant psychological distress in men with commensurable PSMs compared to those who have negative margins [13-15]. Regarding biochemical recurrence (BCR), they are unfavorable pathological findings as extra-prostatic extension and seminal vesicles or invasion of the bladder neck. BCR is defined as a relapse of prostate cancer, the most important indicator of recurrence is the specific antigen (PSA > 0.2 ng/mL) after surgery [13,16,17]. Dalela, et al. in his randomized study reported that the probability of BCRFS was 0.91 (95% CI 0.83-1.0) for anterior versus 0.91 (0.83-0.99) for posterior RARP (p = 0.5) [18]. The incidence of PSM after RP depends on several issues, including tumor biology, patient characteristics, pathological evaluation method, and surgeon's experience, surgical and potentially surgical technique.
Our current meta-analysis revealed that the PSM were not significantly different between the C-RARP and the RS-RARP. Similarly, in a series of two case studies of RS-RARP, one by Galfano in [8] and the other by Santok and colleagues [19] that contain 200 and 294 cases respectively, PSM was found in 25.5% and 22.7%, respectively. On the other hand, some authors have recognized values of PSM slightly higher in those who received RS compared to the conventional technique.
In the work of Lim, et al. [12] there were no differences in the rates of (PSM) there was more tumor extension in the anterior face in the RS-RARP technique compared with the C-RARP, in the subgroup analysis pT2 and pT3 there were no significant differences in the PSM rates. Eden, et al. Obtained results in which [20] PSM were the same for RS-RARP and C-RARP, the location of anterior PSM was higher but without significant value (5.0% vs. 0.0%, p = 0.49).
Based on these previous results, some investigators have advised against performing RS-RARP if the tumor involves the anterior region. With the respect of Menon [11] deserves it was found that there were no statistically significant differences between the 2 groups in the proportion of non-focal margins, which was 11.7% for RS-RARP and 8.3% for C-RARP. In the work of Chang [21] the margin involved in the RS-RARP group was 9 patients (23.3%) compared to 8 patients of C-RARP (26.7%, p = 0.261), without significant differences. These negative results could be related to the learning curve of this novel approach and it's expected to be improved over time as shown in C-RARP. However, some other investigators did not report these similar findings in their studies [22].
RS-RARP allows a rapid recovery of continence; this was shown as a great advantage that was described in most studies of RS-RARP vs. C-RARP. In the RS-RARP group compared to the C-RARP After surgery, the general recovery of continence was quicker in the RS-RARP approach, we must take into account the maximum preservation made of the structures in the anterior part of the prostate gland such as puboprostatic fascia pubovesical ligaments, NVB and Santorini's Plexus (DVC) [23]. These structures participate in an important way, helping the recovery of continence, including the reconstruction of the Retzius space after transperitoneal RARP as stated by Ghanem, which found a faster early continence rate on their cases.
Compared to 48% in the C-RARP, 71% of the men subjected to RS-RARP were continent at the first week of removal of the probe (p = 0.01) [18] with respect to the study de Ghanem, et al. The continence rate was high in both groups (96% for RS-RARP and 94% for C-RARP) [9]. However, continence recovery (i.e., 0 pads) was significantly faster in the RSR-RARP group compared to the control group (p = 0.01). Also in the work of Menon [11] At 6 and 12 months after surgery 98.3% of men treated with the technique of RS-RARP and 93.3%. Treaties with the C-RARP were socially continents [11]. Concerning the work of Lim, et al. East reports that the immediate continence was significantly higher at 7 days in the group of RS-RARP, although no significant difference were reported at the end of 1 year.
The preservation of Retzius space structures could lead to a more anatomical and physiological environment for the previous individual continent status.
The perceptions of preservation of the neurovascular bundles become more and more significant; preservation could partially affect the recovery from the emotional and psychological point of view of the patient [24]. The RARP that preserves the nerves involves different surgical techniques, such as intrafascial or interfascial, anterograde or retrograde approach; meanwhile, there is a lack of randomized controlled trials to define which technique is superior to another. The individual anatomical factors of patients can affect these techniques and approaches; therefore, the surgeon experience is important to decide which surgical technique is more suitable, always trying to reach for incremental nerve preservation [25].
In the work of Galfano [8], he reports that he is the only author who reports sexual function data in his second work of RS-RARP reports 7 powerful patients aged < 65 years who underwent bilateral intrafascial nerve preservation.
In surgery, 40.4% of group 1 versus 40% of group 2 reached their first sexual intercourse within 1 month; at 1 year of follow-up, these figures had increased to 81% compared to 71%, respectively (p = 0.162) [8]. In the work of Menon [11] with C-RARP vs. RS-RARP one year after surgery (69.2% vs. 86.5%) they obtained sufficient erection for intercourse and (44.6% vs. 44.1%) obtained in the SHIM score a score of 17 or more [11].
We can conclude that in the majority of studies used in our meta-analysis, the results regarding sexual potency are not well informed, and more clinical trials are needed to evaluate sexual function in this scenario.
The literature on RS-RARP has few well-designed studies and large participants where long follow-up is carried out. The access has proven to be safe and feasible although technically more challenging than the conventional technique and possibly requiring a longer learning curve. This meta-analysis shows that the RS-RARP and RSR-RARP compared to the conventional technique, achieves a faster continence, the complication rates and the PSMs have similar rates, and no conclusion regard erectile dysfunction could be done.
There are other predictors that can influence the functional and oncological results other than the technique used such as the patient's age, the preoperative IPSS and the SHIM score, the existence of diabetes mellitus, the surgeon's experience, the extent of the tumor and many others. The boundaries of observational studies, short follow-up, short study time and small data in our meta-analysis may avoid a definitive conclusion. Randomized future clinical trials are required to validate and confirm our suggestions.
To our families.
WEPG, MTM and PAMM: Conceptualization, data management, formal analysis, research, methodology, project management, supervision, data presentation, manuscript preparation (development of the original draft), writing (revisions and editions).
MCB: conceptualization, data management, research, preparation of manuscript (development of the original draft), writing (revisions and editions).
PRA and LEP: Conceptualization, data management, research, preparation of manuscript (development of the original draft), writing (revisions and editions).
No conflicts of interests.