The antibiotic prophylaxis for prostate biopsy is not well established, usually is based on fluoroquinolones, but there is an increase of resistance. We explore the efficacy of Fosfomycin trometamol in comparison with ciprofloxacin plus cefoxitin as prophilaxis of this procedure.
A total of 432 transrectal ultrasound guided prostate biopsies were performed: 241 patients received prophylaxis with cefoxitin 2 g i.v. 1 hour before the procedure combined with ciprofloxacin 750 mg p.o. 1 hour before and 8 hours after the procedure A total of 184 patients received prophylaxis with single dose of fosfomycin trometamol 3 g oral the night before the procedure Adverse events in the 30 days following the procedure were analyzed.
Related to overall complications of prostate biopsy, no significant differences were found between prophylactic regimens. No significant differences were found between groups in percentage of both infectious (2.9 vs. 2.2, p 0.64) and non-infectious complications (6.6 vs. 4.9, p 0.24). Percentage of prostatitis (2.2 vs. 2.9, p 0.64), sepsis (0 vs. 1.66, p 0.14) and hospital admissions (1.09 vs. 1.66 p 0.7) in fosfomycin group was lower than in cefoxitin plus ciprofloxacin group without reaching statistically significant differences.
The cohort that received fosfomycin trometamol in our study did not show a higher rate of infectious complications compared with the cohort that received cefoxitin plus ciprofloxacin. Fosfomycin-thrometamole is a safe and effective prophylactic alternative for use in transrectal ultrasound prostate biopsies.
Prostate cancer is the most common malignant solid tumor in men > 70 years and the second cause of death due to cancer [1]. Clinical suspicion is based on an abnormal digital rectal examination (DRE) or persistently elevated prostate-specific antigen (PSA) levels. The main risk factors are: Family history of prostate cancer, advanced age, race, and PSA kinetics [2].
The standard diagnostic procedure is ultrasound-guided needle prostate biopsy, mainly by transrectal approach. It is recommended to take 10-12 core biopsies, bilaterally, from the base to apex of the peripheral zone of the prostate gland, with additional cores from suspicious areas [3].
Transrectal ultrasound-guided (TRUS) prostate biopsy is typically a well tolerated procedure with low morbidity rate. The most frequent complications include hematospermia, hematuria, rectal bleeding and infections [3].
Increased bacterial resistance to antibiotics and the great variability between different geographical regions difficult the establishment of an antibiotic standardized prophylaxis protocol. In recent years, the increase of resistance to fluoroquinolones (FQ) in E. coli and the turn up of ESBL-producing Enterobacteriaceae have raised the question of the appropriateness of using FQ monotherapy as antibiotic prophylaxis for TRUS procedures [2-5]. Fosfomycin trometamol (FT) it is being proposed as a valid prophylactic option for TRUS prostate biopsy [6-9], since it is an oral antibiotic that can be taken as a single dose, so facilitating patient compliance, and also helps reducing the use of broad-spectrum antibiotics [1,10-13]. Before 2007 we used to perform antibiotic prophylaxis with ciprofloxacin. Due to increased antibiotic resistence we moved to cefoxitin plus ciprofloxacin protocol in 2007. In 2015, forced by an intermitent shortage of cefoxitin in our hospital we had to change our antibiotic profilaxies. We decided to switch to single-dose FT.
The aim of the present study is to compare the efficacy of antibiotic prophylaxis for TRUS prostate biopsy in a cohort receiving a single oral dose of FT and a cohort receiving intravenous cefoxitin prophylaxis combined with ciprofloxacin orally.
A retrospective observational cohort study was carried out between January 2014 and September 2016 at the Hospital del Mar, Barcelona, a 420-bed university hospital that performs approximately 200 TRUS prostate biopsy procedures per year. The study involved the collaboration of medical professionals from the Urology, Radiology, Infectious Diseases and Pharmacy departments.
During this period, a total of 432 TRUS guided prostate biopsies were performed: 241 patients received antibiotic prophylaxis with cefoxitin 2 g i.v. 1 hour before the procedure combined with ciprofloxacin 750 mg p.o. 1 hour before and 8 hours after the procedure (Group A). On the other hand, 184 patients received antibiotic prophylaxis with single dose of FT 3 g oral the night before the procedure (Group B) (Figure 1).
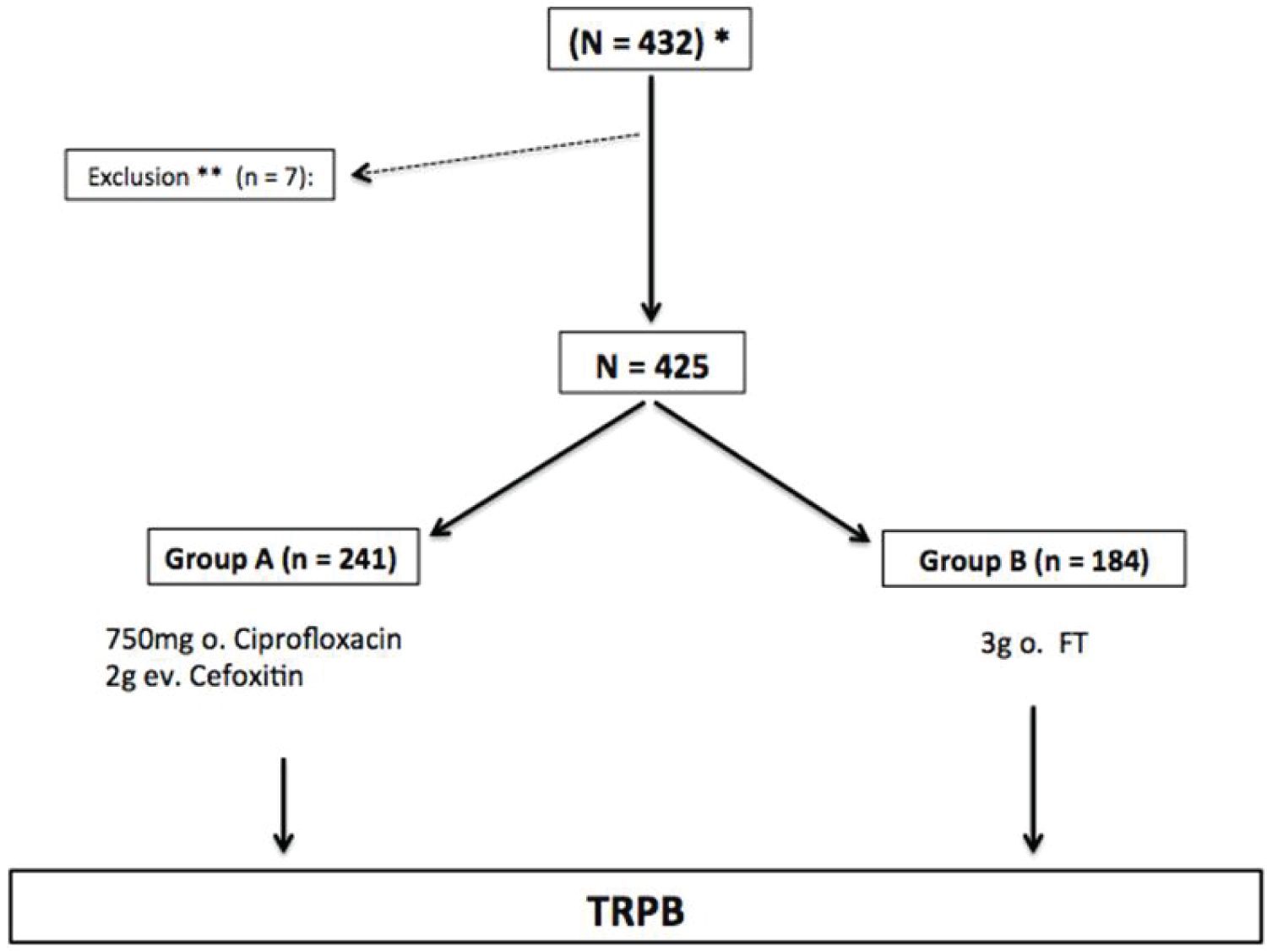 Figure 1: Flow diagram.
Figure 1: Flow diagram.
*Abnormal digital rectal examination and/or elevated PSA > 10 ng/ml, persistently elevated PSA > 4 ng/ml associated with low free; total PSA ratio (< 20%), control biopsy in patients being closely monitored for low-risk prostate cancer; **Allergy or intolerance to antibiotics administered in the study or under a different prophylactic regimen.
View Figure 1
Description of the protocol: Before the procedure, all patients were tested using the urine dipstick test. If leukocytes were present in the urine, a urine culture was performed and targeted antibiotic treatment administered. The procedure was rescheduled after a negative urine culture was obtained. A rectal enema was given in all cases (139 mg/mL sodium dihydrogen phosphate anhydrous and 32 mg/mL disodium hydrogen phosphate anhydrous in rectal solution) approximately 3 hours before the procedure. Anticoagulant and antiplatelet drugs (excluding acetylsalicylic acid 100 mg) were withdrawn 2-7 days before the procedure and re-introduced 2-5 days after, based on clinical criteria and comorbidities. During this period, anticoagulant therapy was replaced by low molecular-weight heparin at prophylactic doses, and antiplatelet therapy by 100 mg acetylsalicylic acid depending on criteria of hematology department.
All patients were provided with information about the procedure and possible post-biopsy complications and signed the specific informed consent for the performance of TRUS prostate biopsy. A transrectal transducer (EC9-4) with a biopsy needle guide (Sterile transvaginal needle guide, CIVCCO®) was used to develop the procedure.
The patient was informed of the need to consult the emergency department of the hospital if complications developed, such as hematuria, fever and/or local symptoms. A control visit was made in the first 30 days to assess any adverse effects associated with the TRUS prostate biopsy.
The inclusion criteria were: Abnormal digital rectal examination and/or elevated PSA > 10 ng/ml, persistently elevated PSA > 4 ng/ml associated with low free total PSA ratio (< 20%), or control biopsy in patients being in active surveillance protocol for prostate cancer.
The exclusion criteria were: Urinary tract infection, allergies or intolerance to the prophylactic antibiotics included in the study (n = 7). A total of 425 patients were included in our study.
The baseline variables were: Age, body mass index (BMI), diabetes mellitus, anticoagulant therapy, antiplatelet therapy (100 mg acetylsalicylic therapy was not considered a risk for bleeding), previous symptoms of lower urinary tract infection (LUTI) and type of biopsy (first or repeat).
The variables analyzed were all expected complications in the 30 days following the procedure: a) non-infectious: Bleeding lasting 3 days or more (hematuria, hematospermia, rectal bleeding), acute urinary retention (AUR) and perineal pain lasting 3 days or more; b) infectious: Prostatitis, orchiepididymitis and sepsis (defined as: Heart rate > 90 per minute, axillary temperature > 38 ℃ or < 36 ℃, leukocyte count > 12,000 uL or < 4,000 uL, normal leukocyte count but with > 10% of immature cell forms present and/or respiratory rate > 20 rpm pCO2 < 32 mmHg); c) number of hospital admissions and d) death.
All recruitment and research protocol were approved by the ethics committee, CEIC- Parc de Salut Mar, Barcelona, Spain.
The Mann-Whitney U test was used for quantitative variables and the Chi-squared test for comparison of qualitative variables. For multivariate analysis, a logistic regression model was performed (adjusted odds ratios). The STATA statistical software package, version 15 (STATA Corp., Texas, USA) was used for statistical analysis, with p < 0.05 being considered statistically significant.
A total of 425 patients were included in the study. The baseline characteristics are compared in Table 1. Patients in group B were older and presented higher prevalence of diabetes than patients in group A. Related to overall complications of TRPB prostate biopsy (Table 2), no significant differences were found between prophylactic regimens. Likewise, no significant differences were found between groups in both infectious and non-infectious complications. Nevertheless, it is worth to notice that percentage of prostatitis, sepsis and hospital admissions in the FT group (group B) was lower than in the cefoxitin plus ciprofloxacin group (group A) but not reaching significant differences. No deaths were related to performing TRUS prostate biopsy during the study.
Table 1: Baseline characteristics by prophylactic group. View Table 1
Table 2: Complications after TRUSBP according to prophylactic group. View Table 2
The presence of complications of any kind 30 days after the TRUS procedure by prophylactic group is shown in Table 2.
There were 7 the cases of prostatitis in group A, 5 of them with E. coli one of them beta-lactamase AmpC plasmid producer. One case due to susceptible Klebsiella pneumoniae and the last one with negative urine culture. Three of the E. coli were resistant to cephalosporins and fluoroquinolones In group B, 4 cases of prostatitis were detected: 2 urine cultures were negative and in the other two E. coli was isolated, one of them resistant to cephalosporins and FQ. It should be noted that all the microorganisms isolated in the cultures of the overall cohort were sensitive to FT.
Four cases of sepsis occured, all in the cefoxitin + ciprofloxacin group. Blood cultures were performed in all cases of sepsis, of which 2 were negative and in the remaining 2, E. coli AmpC plasmid producer and multisensible K. pneumoniae were isolated with the same antibiogram as in urine cultures. It should be noted that the E. coli AmpC plasmid producer isolated, only was sensitive to carbapenems and FT, and the patient was treated with FT 50 mg every 8 hours per 30 days with resolution of sepsis and subsequently negative urine culture.
The hospital admissions in group B (2 patients), were due to non-infectious complications (severe hematuria), while all the admissions of group A (4 patients) were due to urinary sepsis secondary to TRUS procedure.
Antibiotic prophylaxis in TRUS prostate biopsy significantly reduces bacteriuria and urinary infections and consequently hospitalization rates [1,2,14,15]. Although the procedure carries a low incidence of complications, in some cases may lead to severe sepsis and even death [14-17]. In our series, we detected low rate of life threatening complications requiring hospital admission: 4 patients due to urinary sepsis (0.9%). Likewise, the implementation of prophylactic protocol based on FT has been shown to be effective, with low infectious complication rates (2.2%) and no case of urinary sepsis, although without showing statistically significant differences compared to the previous prophylactic regimen, based on ciprofloxacin plus cefoxitin.
In 2007, we introduced a new antibiotic prophylaxis protocol for TRUS prostate biopsy procedures based on cefoxitin 2 g iv + 2 doses of 750 mg ciprofloxacin po, promoted by the increase in Enterobacteriaceae resistant to fluoroquinolones and ESBL-producing bacteria in our environment, similar to the percentage estimated in Spain between 2013 and 2016 by the EARS Net 2016 (31-35%) [18]. The 2007 protocol was based on the microbiological characteristics of bacteria isolated from urine cultures, including those with ESBL-producer Enterobacteriaceae [19]. Urinary sepsis due to ESBL-producing Enterobacteriaceae (mainly ESBL-producing E. coli) is a well known problem and the continued use of FQ as prophylaxis for TRUS procedures helped increase antimicrobial resistance. For this reason, and also because of the problem of shortage of cefoxitin in our hospital, the antibiotic prophylaxis protocol for TRUS was reconsidered, switching to FT in monodose.
FT is a bactericidal phosphonic acid derivative that acts on the cell wall inhibiting peptidoglycan synthesis. It is mainly excreted by the kidneys. After a 3 g oral dose, urinary drug concentrations remain higher than 100 micro g/ml for 30-48 hours [20,21], thus ensuring high penetration into the prostate tissue [12,15,20]. The fact that urinary levels of the drug remain high for more than 24 hours, together with its excellent safety profile [20], means that it can be administered the night before the procedure, so facilitating patient compliance. FT exhibits very high activity among Enterobacteriaceae, including beta-lactamase producers, and at the same time reduces antimicrobial resistance in these pathogens to broad-spectrum antibiotics [20]. Its pharmacokinetic characteristics, easy of patient compliance and susceptibility of Enterobacteriaceae make FT an effective alternative for TRUS.
There is some literature supporting the use of FT in prophylaxis for TRUS prostate biopsy. Lista, et al. [22] conducted a randomized prospective study including 312 patients who were treated with ciprofloxacin and 359 with single-dose FT, and Ongün, et al. [10] carried out a retrospective descriptive study of 620 patients, comparing single-dose oral FT with single-dose ciprofloxacin or levofloxacin [23]. Both studies concluded that FT was a valid alternative in prophylaxis for TRUS prostate biopsy, since no statistically significant differences between groups were found. In our study, an almost 50% drop in cases of post-TRUS procedure prostatitis was observed among patients receiving prophylaxis with FT versus those receiving cefoxitin + ciprofloxacin, which represented a considerable reduction in post-biopsy sepsis and hospital admission in this group, although the differences were not statistically significant.
Use of targeted antimicrobial prophylaxis based on pre-biopsy screening of rectal cultures to identify Enterobacteriaceae was recently suggested as a possibility [20,21,24-26]. Kisa, et al. [25] analyzed the risk factors for infectious complications and FQ and FT resistance in Enterobacteriaceae isolated in rectal swab cultures obtained 3-7 days before TRUS biopsy. Patients without risk factors received ciprofloxacin or FT prophylaxis regardless of the results of the rectal culture, while those with risk factors received targeted antibiotic prophylaxis using ciprofloxacin or FT. Of the 110 patients included in the study, FQ resistance was detected in 60.9% of pre-biopsy swabs, and FT resistance in only 2.7%. There were no statistically significant differences between groups with respect to infectious complications. The authors concluded that ciprofloxacin prophylaxis should be given or not depending on the presence of risk factors and then targeted according to the results of the rectal culture, while the use of FT as antibiotic prophylaxis was completely independent of these two factors. We did not analyze the resistance patterns of the causative uropathogens of post-TRUS infections in our study due to the low incidence of adverse events, although the number of patients with infectious complications was higher in the group with FQ prophylaxis than in the one treated with FT prophylaxis. The two groups were comparable in terms of risk factors. According to commented findings, new studies should be focused on analyzing the risk factors for infectious complications post-TRUS prostate biopsy. This would allow the physician detect the subjects with the highest risk and therefore provide antibiotic prophylaxis based on rectal swab.
The main limitation of our study is the low rate of infectious complications after TRUS prostate biopsy, that could be the meaning of not seeing statistical differences between groups and didn't allow us to analyze the resistance patterns of the causative uropathogens. Obviously, its retrospective nature and the small cohort of patients that is used also could reduce the impact of the study.
In conclusion, it can be state that the use of FT in antibiotic prophylaxis for TRUS biopsies could be a valid alternative, since those patients who received it as prophylaxis in our study did not show a higher rate of infectious complications compared with the previous prophylactic regimen. This observation, together with the fact that FT is easy to administer and reduces the appearance of resistance to broad-spectrum antibiotics, leads us to consider that single dose FT is a safe and effective prophylactic alternative for use in TRUS biopsies.