Introduction: Primary penile sarcoma has an incidence of 0.6 in 100,000 patients in developed countries. Risk factors such as radiotherapy have been identified, which can generate mutagenesis of the irradiated tissue adjacent to the irradiation field. Given the increase in survival of patients that received radiotherapy, the incidence of radio-induced sarcomas has increased. We report the first documented case in Latin America of radio-induced undifferentiated sarcoma of the penis.
Materials and Methods: Case report and literature review.
Results: We report the case of an 89 year-old male patient, who consulted due to a 9-month history of intermittent urethrorrhagia, penile pain and priapism. It is noteworthy that he received radiotherapy for prostate adenocarcinoma. Ultrasound and MRI of the pelvis confirmed a tumor dependent on the right corpus cavernosum, and it was decided to take a biopsy of the mass. Biopsy of the lesion showed a high-grade undifferentiated sarcoma. He underwent radiotherapy and surgery, he had an unfavorable evolution and died shortly after.
Conclusion: Radio induced sarcomas of the penis are rare and usually have a poor prognosis due to delayed diagnosis. Its early diagnosis is difficult because the initial symptomatology is nonspecific, very similar, for example, to that of Peyronie's disease. Thus, a suspicion and timely identification can impact the prognosis of these neoplasms.
Primary mesenchymal tumors of the penis are rare. More than 95% of penile neoplasms correspond to penile squamous cell carcinoma [1]. However, isolated cases of penile sarcomas have been reported in the literature; its clinical characteristics include the appearance of a mass, associated with pain, bleeding and urinary obstruction. Malignant lesions show a greater predilection for the proximal region of the penis while for benign, it is the distal and can be divided into superficial or deep depending on the involvement of the corpora cavernosa [2,3].
Radio therapeutic treatment is a risk factor for the development of neoplasms, which is associated with mutagenesis of the irradiated tissue adjacent to the radiation field, including organs at risk. Regarding to penis, case reports related to radio induced neoplasms have mostly been secondary to radiotherapy for skin carcinomas located on the penis [4]. Concerning to neoplasms secondary to radiotherapy for localized prostate adenocarcinoma, bladder and rectal neoplasms are the most frequent, sarcoma of the penis are extremely rare with only one case reported in the literature [5,6].
89-year-old male patient, ECOG 2, who consulted due to a 9-month history of intermittent urethrorrhagia, penile pain and finally priapism. He had weight loss, with no other additional symptoms.
15 years ago, he was treated for high-risk localized prostate adenocarcinoma T2cNxM0 with external beam radiotherapy for a dose of 70 Gy in 36 fractions and androgen deprivation therapy (ADT) for 2 years. Then restarted ADT one year before consulting for the present condition, apparently due to biochemical recurrence.
Genital examination showed indurations of the proximal and middle third of the corpora cavernosa, without edema or erythema, in the distal third a soft exophytic lesion was palpated towards the right lateral face suggestive of hematoma, glans penis without alterations. Urethrorrhagia is evident. On digital rectal examination, a flat prostate was palpable, no nodules were identified. Testicles without lesions. Given non-ischemic priapism of unclear etiology with suspicion of tumor infiltration, prostate-specific antigen (PSA), urinalysis, penis and urinary tract ultrasound were requested.
Urine analysis showed hematuria, no germs isolated in urine culture, PSA in 7 ng/ml, stable with previous nadir value. Ultrasound of the penis shows an alteration in the morphology of the corpora cavernosa and corpus spongiosum with partial loss of their contours. Two hypoechoic collections are observed in the right lateral aspect of the penis adjacent to the cavernous body, located in its distal and proximal portion, with a volume of 6.6 cc and 5.9 cc, respectively. It is not possible to assess the integrity of the tunica albuginea and Buck's fascia due to the previously described findings. The skin shows no alterations. Ultrasound of the urinary tract showed mild right pyelocalyceal dilation, without alterations in the bladder, prostate and kidneys. Given these results a bone scan and contrast-enhanced MRI of the abdomen and pelvis were requested.
Abdominal MRI showed liver with simple cystic lesions, bilateral simple kidney cysts and dilatation of the collecting system and right ureter. In the pelvis, a mass with poorly defined contours is evident which involves the right crura and compromises the corpus cavernosum on this side and the corpus spongiosum in the proximal third, displacing the urethra to the left, without having a cleavage plane with the tunica albuginea. The mass has an intermediate signal in T1, has a heterogeneous enhancement after contrast medium administration and maintains an intermediate signal in T2, being quite heterogeneous with hypointense centers, there is no evidence of regional adenopathies (Figure 1). Bone scan with showed no evidence of disease.
 Figure 1: MRI of pelvis. The mass is of intermediate signal in T1, it has a heterogeneous enhancement after the administration of contrast medium.
View Figure 1
Figure 1: MRI of pelvis. The mass is of intermediate signal in T1, it has a heterogeneous enhancement after the administration of contrast medium.
View Figure 1
A percutaneous biopsy of the mass was taken, with a sample composed of medium and large sized cells with eosinophilic cytoplasm, oval nuclei, some eccentric, rosetoid organization around the blood vessels, with extensive necrosis. Immunohistochemistry markers were performed being CK7, CK20, P63, CK134, CD45, CD34, desmin, caldesmin and BLC2 all negative. KI67 with a cell proliferation index of 47%, vimentin was strongly positive, SMA (anti smooth-muscle actin) negative. Based on the above results, the mass was reported as high-grade undifferentiated pleomorphic sarcoma, highly malignant (Figure 2). A stromal neoplasm was ruled out since the neoplasm was CD34 negative and because of its the clinical behavior.
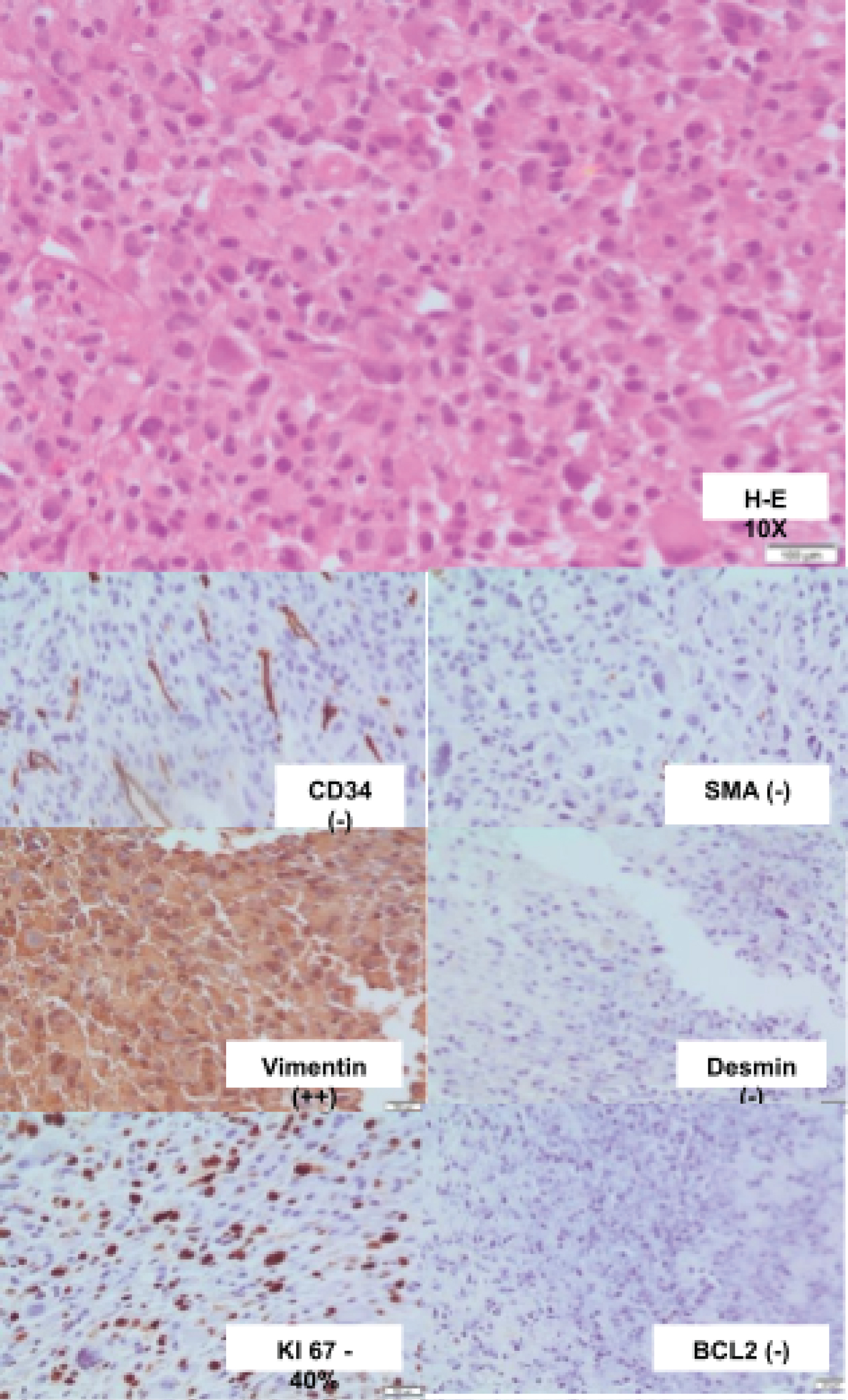 Figure 2: Histology and immunohistochemistry of percutaneous biopsy of penis. Strongly positive for vimentin, KI 67 40%, negative for other markers.
View Figure 2
Figure 2: Histology and immunohistochemistry of percutaneous biopsy of penis. Strongly positive for vimentin, KI 67 40%, negative for other markers.
View Figure 2
Given a diagnosis of locally advanced high-grade undifferentiated pleomorphic sarcoma of the penis dependent of the corpora cavernosum, most likely radio-induced with deterioration of the functional status, he was taken for local management with radiotherapy and subsequent surgery.
Shortly after the patient presented a rapid local progressive evolution, with increased bleeding requiring transfusion (Figure 3), and soon after died.
 Figure 3: Local clinical progression. There is evidence of increased local tumor involvement with ulceration and bleeding.
View Figure 3
Figure 3: Local clinical progression. There is evidence of increased local tumor involvement with ulceration and bleeding.
View Figure 3
Primary penile sarcomas are rare, with only few cases reported in the literature. Different subtypes of primary penile sarcoma exist, being the Kaposi sarcoma, angiosarcoma, leiomyosarcoma, and epithelioid sarcoma the most common and pleomorphic sarcoma the rarest [7]. We report the second case worldwide of an undifferentiated pleomorphic sarcoma of the penis that meets criteria for radiation-induced malignancy.
The prognosis of sarcomas depends on several factors. One is whether the lesion is superficial or deep; superficial lesions are those originating from the dartos muscle layer, the piloerector complex and the muscular walls of superficial vessels situated outside the albuginea. They present as a small tumor in the distal shaft or the penile prepuce. Superficial lesions are slow growing tumors that are likely to recur locally with fewer propensities for metastases. Instead, deep lesions which are those arising from the proximal portions of the corpora cavernosa or corpus spongiosum. Clinically they are poorly circumscribed, firm, non-tender masses that infiltrate surrounding tissues and cause urinary obstruction. Deep lesions show a greater propensity to metastasize and have a poorer prognosis. The other important factor related with poor prognosis is tumor size, degree of differentiation, and metastatic invasion [8,9].
Secondary malignant neoplasms (SMN) are late complications associated with exposure to genotoxic treatments, such as radiotherapy. The universally accepted criteria for determining a radiation-induced neoplasm are the modified Cahan criteria; these propose that for a neoplasm to be considered radiation-induced, it must be fulfilled that: the tumor is in the irradiation field, there is a sufficient latency period generally greater than 4 years, the primary and secondary tumor have different histologies and the tissue where the secondary tumor originates had to be metabolically normal prior to irradiation [10,11].
Primary penile sarcomas typically appear as an asymptomatic, unremarkable, cutaneous or subcutaneous nodule without superficial skin abnormalities. Later manifestations are very unspecific and includes sensation of a painless nodule or induration of the corpus cavernosum, penile deviation, obstructive voiding symptoms, dysuria, or erectile pain [12].
The most common penile sarcomas are those of vascular origin specifically the angiosarcoma of the penis which is the most common penile sarcoma. It should be noted that these are the most frequent radiation-induced neoplasms, with most cases due to radiation for squamous cell carcinoma of the penis. Kaposi sarcoma have been described which usually have cutaneous manifestation and are associated with HIV infection. A distinctive feature of Kaposi sarcoma is that it doesn't have a deep location in the penile shaft, which is common in the other sarcomas of vascular origin [1,13-15].
Malignant peripheral nerve sheath tumors (MPNSTs) are rare soft-tissue sarcomas that arise from the peripheral nerves and are derived from Schwann cells. These tumors primarily arise in the setting of neurofibromatosis. MPNST of the penis are rare with only 8 cases reported in the literature, three of which are not associated with neurofibromatosis. Because MPNSTs have an inherently aggressive nature and can originate from multiple cell types, diagnosis is difficult [16].
Leiomyosarcomas are the most frequent penile sarcomas of myogenic origin [3]. Epithelioid sarcomas of the penis are a malignant soft tissue tumor of unclear cell type and origin [17]. These tumors are usually slow growing and are well known for their high propensity for local recurrence with regional and distant metastases [18].
Primary undifferentiated pleomorphic sarcoma of the penis is extremely rare, with only 4 cases reported in English literature and essentially represents a diagnosis of exclusion. The average tumor size was 5 cm and prognosis was associated with local recurrence and progression distance [7,9,19,20].
A systematic review and meta-analysis aimed to determine whether there is an association between exposure to radiation therapy for prostate cancer treatment and subsequent second malignancies. 21 studies were analyzed in which they reported patients with confirmed adenocarcinoma of the prostate treated with commonly used forms of radiotherapy. Controls were patients who did not undergo radiotherapy. The authors found a possible association between radiotherapy for the treatment of prostate cancer and an increased risk of bladder, colorectal, and rectal cancers. It is notable that odd ratios to radio induced neoplasm's increased with a longer latency period (5 years versus 10 years). Although there was an increase in risk, the absolute rates of these secondary cancers remain low [5].
Regarding to penile sarcomas secondary to prostate radiation, after extensive literature searches, we only found two case reports. One was reported by Hakky, et al. the case is about a 70-year-old patient with a history of interstitial brachytherapy for a prostate adenocarcinoma, who was diagnosed with a secondary malignancy consisting of a locally advanced penile sarcoma involving the prostate and base of the bladder as well. He was taken for surgical resection. The report does not specify the type of sarcoma nor the time or duration of radiotherapy [21].
The other case which is similar to ours was reported by Sugiara, et al. is of a 47-year-old patient who consulted for pain and indurations of the penis. He was diagnosed with prostate adenocarcinoma 11 years ago and required radical prostatectomy, with subsequent management with ADT and radiotherapy. Physical examination documented a hardening that appeared to be in the corpus cavernosum with a maximum diameter of 9 cm. A biopsy of the mass was taken and showed findings suggestive of an undifferentiated high grade pleomorphic sarcoma. He was taken for surgical resection but 4 months after the operation he had local recurrence with rapid growth and recurrent bleeding. Thoracoabdominal CT multiple reported lung metastases. Patient died 2 months later. In this case, the diagnostic criteria of Cahan were met, so the possibility of radiation-induced sarcoma was considered [6].
There is no standardized management for penile sarcoma, given its low incidence. Treatment approach for penile sarcomas includes partial or total penectomy. The goal of surgery is complete removal of the lesion with clear margins and, if applicable, of other affected organs. Total penectomy is indicated in masses larger than 2 cm or if there is involvement of deep structures. In palliative care, penectomy may resolve bleeding and pain [22].
Adjuvant radiotherapy after mass resection is beneficial in high-grade tumors. Sarcomas are generally poorly radiosensitive and chemo sensitive neoplasms [23], so radiotherapy or chemotherapy have not been used extensively in undifferentiated sarcomas of the penis. It has been described in metastatic disease the use of anthracycline-based chemotherapy regimens such as doxorubicin and ifosfamide or doxorubicin and dacarbazine as first-line therapies, and taxane-based regimens in the second-line setting [7].
The insidious onset of most primary penile sarcomas usually leads patients not seek medical care for several months to years, waiting until the mass eventually grows and becomes symptomatic, being frequent that at time of consultation patients have large tumors with metastatic disease. Furthermore, given its unspecific symptoms and rarity, primary penile sarcoma is often misdiagnosed as Peyronie disease or another benign disorder. So treatment of primary penile sarcomas often occurs late in the disease process [7]. Patients with deep lesions, a large tumor size and a low degree of differentiation have high local recurrence rates and development of metastases with the common metastatic sites being lung (90%) and bone (8%), regional lymph node metastases are uncommon. A patient who has a deep lesion with metastases and extensive tumor involvement, its disease is incurable and will have a high mortality rate [8,9,24] which is exemplified in the present case. Hence, the best approach for the management of these malignant penile lesions is early diagnosis and treatment before invasion occurs.
This is the first case reported in Latin America and the second case worldwide of radiation induced undifferentiated sarcoma of the penis. Sarcomas of the penis are rare and should be considered as a differential diagnosis in cases of pain and induration of the penis since an early and timely identification can impact on patient prognosis.
None.
The authors declare that they have no competing interests.
Written informed consent was obtained from the patient for publication of this case report and accompanying images.