Polyorchidism is a rare congenital anomaly of the urogenital tract. Usually, it requires conservative management; however, this varies according to each patient. This report summarizes the possible clinical presentation and the feasible management options depending on the patients and testicular characteristics.
23 years old young male presented to our outpatient clinic with intermittent left testicular pain associated with tenderness to palpation. On the physical exam, he had a palpable mass at the upper pole of the left testis. He was taken to an MRI, which showed a normal right testis with a left mass-dependent of the upper pole of the left testis. He was discharged after pain control was achieved; however, he presented again to the Emergency Room with acute left testicular pain one week later. The physical exam was suggestive of left testicular torsion. He was taken to surgery for scrotal exploration and bilateral testicular fixation. Polyorchidism was confirmed intraoperatively.
Gonadal disorders, Urogenital abnormalities, Testis, Congenital abnormalities, Gonads
Polyorchidism or supplementary testis is a developmental anomaly defined as the presence of more than two testicles [1]. There are several forms of this feature, being triorchidism the most common one. It was first described in the XVI century on an autopsy [1]. Later, in 1880,it was confirmed on histological labeling [2]. Different theories currently have been proposed to understand this developmental anomaly. However, the exact cause is still unknown [3].
Concerning the diagnosis, supernumerary testes can be suspected on clinical examination. Although, in some cases, testicular pain secondary to torsion can be the only positive finding on the physical examination [4]. Testicular torsion represents the more frequent cause for testicular loss. It is considered a surgical emergency because of the opportunity of testicle salvage [5]. The diagnosis should be made clinically, and other causes of acute scrotum should be ruled out. In the case of polyorchidism, testicular torsion may occur by rotation of the entire content of the hemiscrotum or only of the supernumerary testicle [6].
Most authors suggest that polyorchidism should be confirmed histological and that prophylactic orchidopexy is necessary. To date, there is no known systematic analysis that shows the occurrence of polyorchidism, concomitant to malignancies, the reason why more conservative management has been proposed [4].
We present a case report of a young male of 23 years old with intraoperatively confirmed polyorchidism, along with a comprehensive literature review. We summarize the possible clinical presentation of the pathology along with its feasible management depending on the patient's testicular characteristics.
A healthy 23-year-old male showed to the outpatient clinic presenting a two-year-long left scrotal mass sensation and intermittent pain. A solid mass from the inferior pole of the left testicle was found palpated on physical examination. It was painless when palpated and independent from the epididymis. Testicular ultrasound was performed in the urology department, evidencing a left-sided testicle's lower pole round mass, with the same echogenicity as the rest of the testicle. The right testicle was normal, with dimensions of 50 × 31 × 33 mm with a volume of 27 cm3.The left testicle was 36 × 24 × 29 for 13 cm3, and the upper pole mass ipsilateral to the left testicle was 14 × 13 × 16 mm with a volume of 1.5 cm3 (Figure 1). Considering the findings suggesting a peritesticular mass, tumoral markers and a pelvic MRI were ordered.
 Figure 1: US. LT, Left testicle. SLT, Supernumerary left testicle. SLT located in the upper pole of the LT, both with similar echogenicity.
View Figure 1
Figure 1: US. LT, Left testicle. SLT, Supernumerary left testicle. SLT located in the upper pole of the LT, both with similar echogenicity.
View Figure 1
Tumor markers were within normal ranges. The MRI showed a right testicle with dimensions of 50 × 31 × 33 mm, a volume of 27 cm3, and a regular right epididymis. The left testicle had a volume of 13 cm3, an image in the inferior pole with similar characteristics to the testicular parenchyma was found, corresponding to an accessory testicle of 1.5 cm3 (Figure 2). Testicular biopsy was omitted considering the markers and the imaging characteristics.
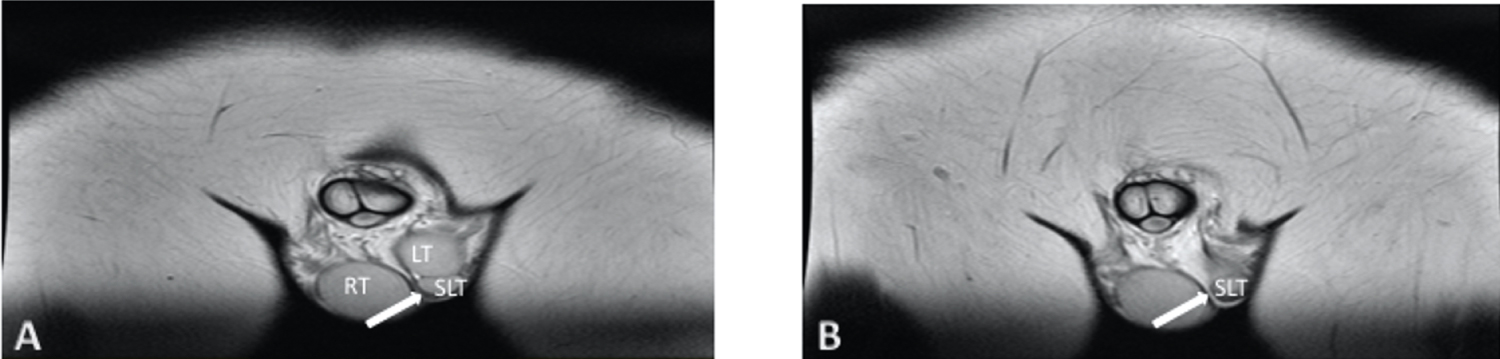 Figure 2: Figure 2A and 2B MRI. LT, Left testicle. SLT, Supernumerary left testicle, and left testicle showing similar echogenicity. SLT is located adjacent to the lower pole of the left testicle.
View Figure 2
Figure 2: Figure 2A and 2B MRI. LT, Left testicle. SLT, Supernumerary left testicle, and left testicle showing similar echogenicity. SLT is located adjacent to the lower pole of the left testicle.
View Figure 2
He presented to the Emergency Room with acute severe left testicular pain one week later. Physical examination was suggestive of left testicular torsion. A new Doppler US was performed, which showed the supernumerary testicle in the upper pole of the left testicle and with decreased vascular flow, supporting the diagnosis. The patient was taken to the OR and underwent scrotal exploration surgery confirming testicular torsion with a supernumerary testicle on the left side. Testicular fixation was performed bilaterally using a dartos pouch and fixation of the tunica albuginea to the dartos layer in the inferior aspect of the testicle with 3-0 absorbable sutures. During surgery, the continuity in the albuginea was evident, so it was considered that taking the supernumerary testicle out represented a risk for the integrity of the left testicle, leading to injury or other complications, therefore the supernumerary testicle was not removed. Intraoperative findings are described in Figure 3.
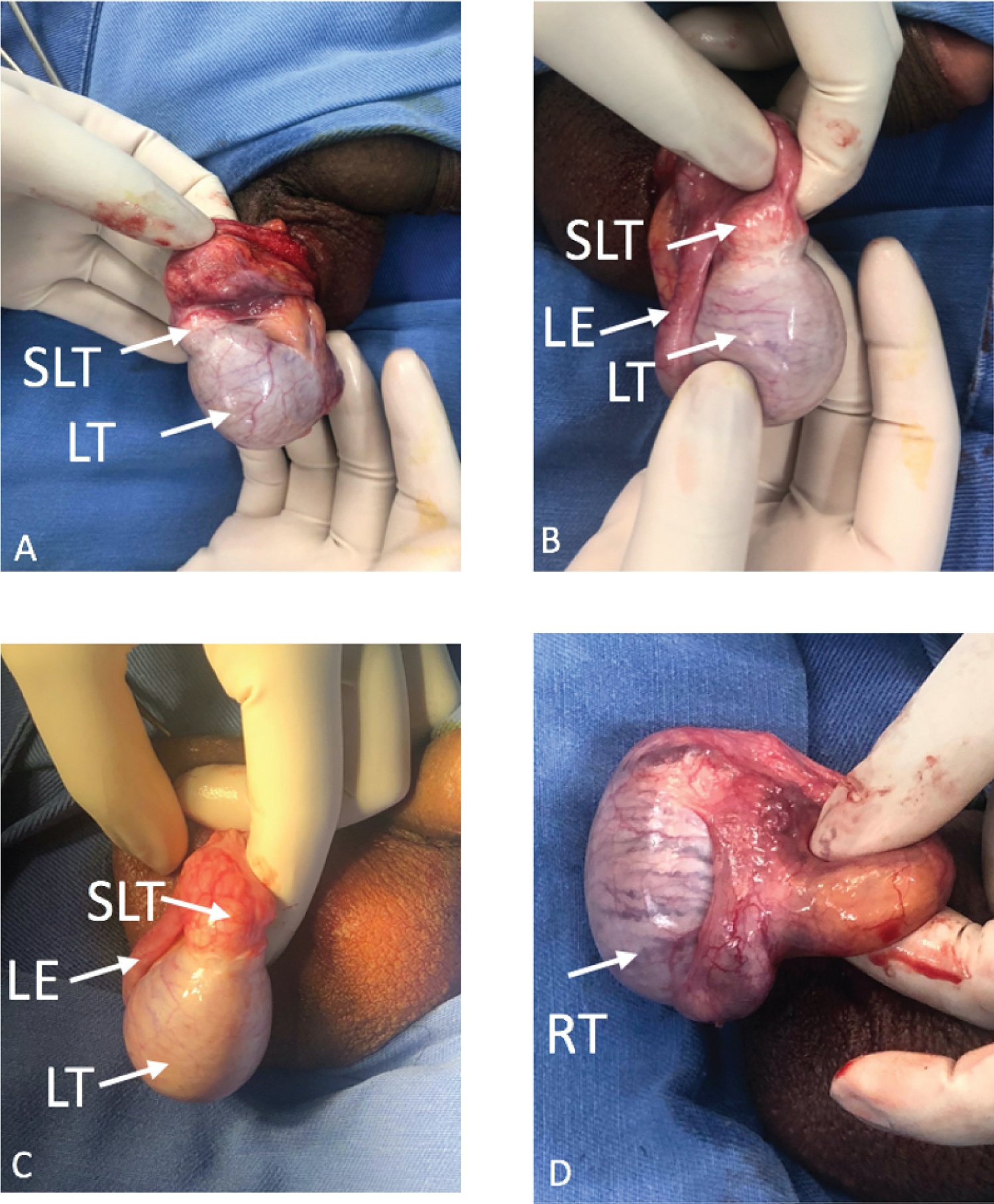 Figure 3: Operative findings A-D. LT, Left testicle. RT, Right testicle. SLT, Supernumerary left testicle. LE, Left Epididymis.
View Figure 3
Figure 3: Operative findings A-D. LT, Left testicle. RT, Right testicle. SLT, Supernumerary left testicle. LE, Left Epididymis.
View Figure 3
The patient attended a post-operatory consultation nine days after surgery. The pain was controlled, and no other complications were addressed. After four months, the patient went to another appointment; this time, he presented with testicular pain. He had a Doppler ultrasound with no changes from the previous one. Therefore, pain management was prescribed with sertraline and a short cycle of non-steroidal anti-inflammatory drugs.
We conducted a literature review in Embase using 'polyorchidism', finding 278 results dating from 1948 to January 2021. Only cases reports were considered; 200 case reports worldwide were found. A language filter was included during the literature search; only case reports written in English were included. The present manuscript aims to depict the current available understanding of this unusual feature.
In the fifth to sixth week of development, both the right and left intermediate mesoderm gives rise to a structure called the urogenital ridge. It has two portions, a lateral and wider nephrogenic portion and a more medial one, the gonadal portion. This primitive gonadal structure will receive the migration of the primordial germ cells formed in the yolk sack. Future gonads will be developed after induction and differentiation [7]. In this sense, the gonadal development in terms of quality and quantity depends significantly on an induction process. In the male embryo case, this process is determined by the presence of the SRY gene [8].
In a subsequent process, dependent on high testosterone levels and the Mullerian Inhibiting Factor (MIF), the male genital systems will derive from the Wolffian ducts. In contrast, the potentially preprogrammed Mullerian ducts will be inhibited to enhance testes' production instead of ovaries. Thus, the male paramesonephric (Mullerian) duct disappears except its upper end, which will persist as an appendix [7].
The physiologic process to develop normal testes has been widely described. Moreover, the embryologic sequences that enable supernumerary testicles are yet to be elucidated. The current debate about the matter includes theories involving irregular migrations of cell populations inducing a longitudinal duplication of the genital ridge and the presence of peritoneal mesenchymal expansions causing transverse division over the genital ridge [2,7]. The above can result in a complete or incomplete duplication with a fully separated testis and epididymis [2]. Patients with polyorchidism often present with other anomalies such as cryptorchidism, spermatic cord torsions, or neoplasms [2].
No consensus on the classification of polyorchidism has been stated. However, different authors have created distinct categorizations. In 1988, Leung, et al. described the first anatomical classification of polyorchidism according to anatomical variations [9]. Later on, in 1991, Thum, et al. published a new classification based on the embryologic origin and functionality [10,11]. Even though these two classifications helped sort this developmental anomaly, no surgical management guidance was proposed.
One year after Thum's classification system was described, Singer, et al. created a new classification based on the testes' anatomy and reproductive potential to help surgical management [7]. This system is based on the anatomic and functional arrangements and the drainage systems combined with possible surgical complications. This classification helped elucidate a management strategy [7].
Finally, in 2007, Bergholz and colleagues presented a new anatomical system regarding polyorchidism's functional taxonomy. Testis being drained by a deferent duct were classified as a type A divided into three subcategories. In A1, the drained supernumerary testis had its epididymis and vas. If the drained supernumerary testis had its epididymis but shared a common deferent duct, it is A2. In A3, the drained supernumerary testis shared a common epididymis. The testes that were not drained by a deferent duct were classified as a type B, divided into B1 and B2. In B1, the testis did have its own epididymis, while in B2, the testis did not have its own epididymis; Therefore, consisting of testicular tissue only [4]. Our patient is a polyorchidism type A3.
Commonly, patients with polyorchidism are diagnosed in childhood or teenage years due to the appearance of intermittent testicular pain associated with a palpable mass [1]. However, our patient was an adult that presented to the Emergency Room with new-onset testicular pain. The most frequent presentation is triorchidism, and the supernumerary testis is most frequently located on the left side [12], as in our patient. The location explanation might be that the left testis is more prone to subdivision because of its greater size and different vascular topographic anatomy. However, this has not been proved [12,13].
Congenital anomaly has been associated with cryptorchidism (40%), hernias (30%), torsion (15%), hydrocele (9%), and malignancy in 6% of cases [1]. This case is clinically relevant because the extra testicle caused the left testicle torsion. It corresponds to an unusual presentation, but it is a differential diagnosis that should be considered. Additionally, in some patients, polyorchidism might present as persistent fertility after vasectomy, retractable testes, or ureteropelvic duplicity, which would be explained by the common embryologic origin of the ureter and the vas [11].
Our literature review found that in two reported cases, the patients presented to the urologist with intermittent pain in the left groin, associated with long-standing mass sensation, exacerbated in a short period [14]. In other cases, the patient presented with left scrotal pain without scrotal swelling or severe pain in the scrotum of short-time evolution [15]. Our patient reported a two-year left scrotal mass sensation with intermittent pain, exacerbated one week before admission to the emergency room for testicular torsion on the left side. In the above-reported cases, there is no history of trauma. Severe pain has been present for a short time, and patients' primary concern in the emergency room was the severe onset of scrotal or groin pain. Furthermore, Bergholz, et al. found an association of polyorchidism with pseudohermaphroditism, nephrolithiasis, and infertility. Additionally, of the 140 cases with histological confirmation reported in the study mentioned above, only 23 patients (16%) presented with painless scrotal or inguinal swelling without any other symptoms or disease [16].
It is worth mentioning that most patients with polyorchidism have a standard 46, XY karyotype. Nevertheless, chromosomal irregularities such as 46, XX, XY mosaicism, and deletion of the long arm of the 21st chromosome have been reported [17].
In most cases, polyorchidism is suspected by clinical examination as an incidental finding. Still, according to Bergholz, et al. the diagnoses should be supported by images. Hydrocele, spermatocele, varicocele, Morgagni cyst, or testicular neoplasm can be mistaken for a supernumerary testis. Additionally, an undescended testis in the groin area can be wrongly diagnosed as an inguinal hernia [16].
Some authors argue that ultrasound alone is enough to make the final diagnosis [18]. However, a Doppler ultrasound or an MRI can also be helpful for diagnosis. The ultrasound will identify a scrotal mass identical to the ipsilateral testis on every ultrasonographic technique performed, as is shown in our case in Figure 1 [19]. The Doppler will report a mass separated from the testis with a gray-scale ultrasound pattern, showing similar echogenicity or slightly less echogenic than the normal testis, and provides information on the vascularity and viability of the gonad [20]. Meanwhile, on the MRI, a typical oval or round structure can be observed with the signal characteristics of the testicles: a homogeneous intermediate signal intensity on T1 and high intensity on T2. In some cases, the MRI will not provide additional information than the one found on the sonography. However, the MRI would play a confirmative diagnosis role [21].
Furthermore, new techniques cannot always differentiate between supernumerary testes and other kinds of testicular masses. Therefore, a close follow-up, including serological markers for malignancy, must be done if the patient does not undergo surgical exploration or biopsy [12].
Management of polyorchidism has been controversial since this congenital anomaly of the male urogenital tract was first described [22]. Previously, it was reasonable to remove the supernumerary testis regardless of its location because of the incidence of testicular torsion and the suspected malignancy [16].
However, in 1987, more conservative management was proposed with the advent of ultrasound and MRI [16]. Some authors have suggested that if there is no coexistent disorder and testicular tumor markers are negative for a malignant disease, surgical exploration or biopsy is unnecessary, and patients can be followed up conservatively [12].
In 2008, Khedis, et al. proposed polyorchidism management based on a simple Polyorchidism classification or a Complicated Polyorchidism. A simple case is when the supernumerary testes were in an orthotopic position without any malignancy signs or association with other abnormalities. They suggested surveillance with physical examination and testicular ultrasound in these patients. Complicated polyorchidism is defined as supernumerary testis associated with malignancy or abnormalities. In this case, they considered radical orchiectomy of all testes on the suspicious side [23]. Finally, Khedis, et al. propose that in young patients with polyorchidism plus cryptorchidism, orchidopexy and observation should be done, if feasible [23]. The management of polyorchidism depends on the patient's age, the testicular location, size, and the anatomical organization of its drainage system [24].
Polyorchidism is a rare developmental anomaly of the male genital tract whose exact causes remain unknown. Typically, patients will present to the urologist with intermittent scrotal pain associated with a mass sensation. Testicular torsion might be present in 15% of the patients. In testicular torsion symptomatic patients' scrotal exploration and fixation of the testicle is recommended. Patients must continue active surveillance after surgery. However, there is no evidence to determine how long a patient with polyorchidism must be followed up.
Not applicable.
Written informed consent was obtained from the patient for publication of this case report and images usage.
The authors declare that they have no competing interests.
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.