Delirium is a very frequent alteration of postoperative behavior in children. Tonsillectomy surgery is related to severe sleep apnea and does not indicate benzodiazepine premedication. Non-premedication is directly related to the presence of negative behaviors. Dexmedetomidine is a safe option for children with obstructive sleep apnea (OSA) since it does not affect airway tone.
The main aim of this retrospective observational study is determining whether intranasal dexmedetomidine premedication decreases the incidence of preoperative anxiety, postoperative delirium, and the need for postoperative sedatives and opioids in children undergoing tonsillectomy.
83 patients aged between 2 and 11 years were enrolled in a retrospective observational study in two groups according to receiving 1 µg/kg of intranasal dexmedetomidine premedication or not. Preoperative anxiety was assessed using the Yale Preoperative Anxiety Scale (YPAS). Postoperative Delirium was measured with the Pediatric Anesthesia Emergency Delirium (PAED) at 15, 30, and one hour after admission into the Postanesthetic Care Unit (PACU). Demographic data, intra-operative analgesics, post-operative opioids and sedatives administered, post-operative bleeding and perioperative respiratory adverse effects (PRAEs) were collected.
Study groups were comparable. The incidence of preoperative anxiety was 57.89% in non-premedicated compared to 26.67% in the dexmedetomidine group (p = 0.008). The delirium at 30 minutes was 52.63% in non-premedicated compared to 28.89% in premedicated (p = 0.048). Anxiety or delirium occurred at any time was 92.11% in non-premedicated compared to 68.89% in premedicated patients (p = 0.0194). No statistically significant differences were found in the need for intraoperative or postoperative opioids or postoperative sedatives, bleeding, or PRAEs. No cases of hypotension, bradycardia have occurred.
The incidence of preoperative anxiety and delirium in children without premedication is very high. Premedication with 1 µg/kg intranasal dexmedetomidine reduces preoperative anxiety and the incidence of anxiety and delirium at any time in the perioperative period.
Dexmedetomidine, Premedication, Delirium, Children, Pediatric
Delirium or agitation upon awakening is a very frequent alteration of postoperative behavior in children (up to 80%), especially at school age and general anesthesia with sevoflurane. It is accompanied by an increased risk of self-injury, bleeding from surgical bed dehiscence, and requires a higher dose of sedatives, which can delay discharge [1-3]. In addition, non-premedication has been related to preoperative anxiety in children of up to 65% and is directly related to the presence of negative behaviors such as postoperative delirium [4]. Anxiolysis before induction of anesthesia is, therefore, an important aspect of pediatric perioperative planning.
Benzodiazepines are the most widely used drugs as preoperative anxiolytic medication in pediatric patients [5]. Tonsillectomy surgery is related to postoperative delirium [1] but because of the risk of perioperative respiratory adverse events (PRAEs) in obstructive sleep apnea (OSA), benzodiazepines are not indicated as premedication in these patients.
Dexmedetomidine is a potent α2 adrenoreceptor agonist with analgesic effects without causing respiratory depression like opioids, so it may be safer. It also has sedative effects by inhibition of the locus coeruleus, reducing agitation, and sympatholytic effect by decreasing the release of norepinephrine in the sympathetic nerve endings. Dexmedetomidine is 8 times more powerful and more specific (α2/α1, 1620/1) than clonidine (α2/α1, 220/1) allowing it to have fewer side effects [4,6,7].
Administration of Dexmedetomidine at the end of surgery or continuous infusion has better results in terms of preventing postoperative delirium than bolus propofol at the end of surgery or continuous intraoperative ketamine administration [8].
Currently, the United States Food and Drug Administration (FDA) approves sedation through intravenous bolus and continuous infusion up to 24h in intubated adults, areas outside the intensive care unit (ICU) and the operating room environment. However, in Europe, it is indicated for sedation of adults in the ICU and non-intubated adult patients, before and/or during diagnostic or surgical procedures that require sedation. Although there is currently no worldwide approval for administration to the pediatric population in the operating room, the favorable pharmacological effects of dexmedetomidine combined with its limited adverse effect profile have facilitated its introduction into the perioperative environment and in children as compassionate use [9].
Dexmedetomidine, administered in dose even in higher than recommended, has been shown as a safe option for children with OSA since it does not affect airway patency and tone [9].
Nowadays, most studies of postoperative agitation in children have been performed with single or continuous intravenous doses of dexmedetomidine. Although the ability of dexmedetomidine to decrease preoperative anxiety has been studied, the data are limited in defining the dose and route of administration in premedication for the reduction of postoperative anxiety and postoperative pain [7].
It is hypothesized that intranasal dexmedetomidine premedication decreases the incidence of preoperative anxiety, postoperative delirium, and the need for postoperative sedatives and opioids. We have therefore designed a retrospective observational study with the main aim of determining whether this is achieved in children undergoing tonsillectomy ± adenoidectomy. Incidence of adverse respiratory effects, bleeding or reintervention will also be evaluated.
Our study was designed to analyze the effect of dexmedetomidine premedication in children on the incidence of delirium and agitation after tonsillectomy ± adenoidectomy. After obtaining approval of the Pediatric University Hospital Niño Jesús (Madrid) ethical committee, and written informed consent from parents or legal representatives, 83 patients were enrolled in a retrospective observational study following the STROBE statement.
Children with OSA aged between 2 and 11 years, scheduled for tonsillectomy surgery under general anesthesia using sevoflurane for induction and maintenance were included. Children who underwent adenoidectomy only, with total intravenous general anesthesia, a previous diagnosis of delirium, children who received intraoperative and/or postoperative dexmedetomidine or with contraindication for the use of dexmedetomidine were excluded.
Patients were included in one of the study groups according to receiving dexmedetomidine premedication or not: GROUP A (not premedicated) or GROUP B (Premedicated). The administration of benzodiazepines or opiates as a pre-medication was contraindicated in all patients included for OSA following the premedication hospital's protocol.
Group A patients received 1 µg/kg of intranasal dexmedetomidine with atomizer 45 minutes before the intervention. Group B patients received no anxiolytic premedication.
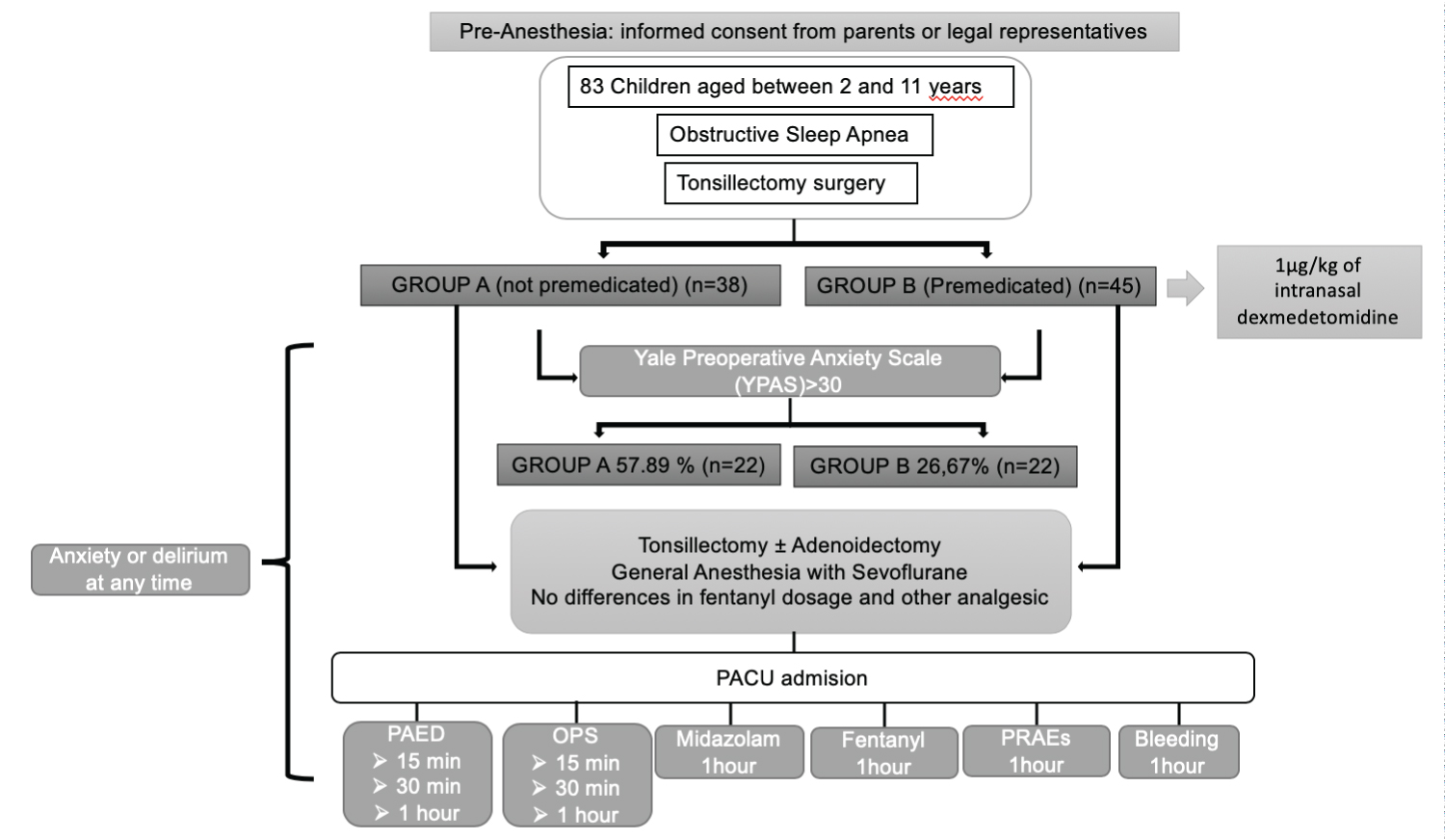 Figure 1: Study procedure. View Figure 1
Figure 1: Study procedure. View Figure 1
Blood pressure (BP) and heart rate (HR) were measured before premedication and 30 minutes later. A drop in BP or HR > 30% was considered a hemodynamic event.
Preoperative anxiety was assessed using the Yale Preoperative Anxiety Scale (YPAS) [10] by anesthetic staff trained on the scale.
During anesthesia, drug doses and programming parameters of different devices were standard.
After surgery, patients were transferred to the post-anesthesia care unit (PACU) where they received analgesic treatment following our hospital's mild-moderate pain protocol.
Delirium on awakening from anesthesia was measured by the Pediatric Anesthesia Emergency Delirium (PAED) [11] at 15, 30 and 1 hour after PACU admission. A value of PAED > 10 in any measurement was considered delirium and midazolam 0.5-1 mg/kg was administered.
Postoperative pain was assessed using an objective pain scale (OPS) [12] at 15, 30, and 1 hour after admission into the PACU. If rescue analgesia was required (OPS > 3), fentanyl 0.5 µg/kg was administered.
Demographic data (Table 1), premedication administered, intra-operative anesthetics and analgesics, post-operative opioids and sedatives administered, post-operative bleeding and PRAEs were collected.
Table 1: Demographic Data: Data are listed as "% (value)" or as "median [interquartile range]". P-Values are by Mann-Whitney U for continuous data and by Chi-square for % measures, or by Fisher´s exact test when cell counts were less than 5 for qualitative data. View Table 1
Quantitative data were checked for normal distribution by the method of Kolmogorov-Smirnov-Lilliefors. Differences between subgroups were analyzed by a Student's t-test or the Mann & Whitney U test depending on their distribution. Categorical data were analyzed by a Chi-square test with Yates's continuity correction. A p-value of 0.05 was considered significant.
Statistical analysis was performed using R 3.6.1 binary for MAC OS × 10.13.6.
Sample size calculation has been performed to obtain a power of 80% with an alpha error of 5% and using the data published by G Guler, et al. [13].
Finally, 83 children were included. Study groups were comparable in terms of demographics and intraoperative fentanyl doses (Table 1).
The incidence of preoperative anxiety measured with the YPAS scale was 57.89% (22) in the non-premedicated patients compared to 26.67% (12) in the dexmedetomidine premedicated patients (p = 0.008).
The delirium defined as a PAED > 10 at 15 minutes, was registered in the 63.16% of the non-premedicated children, and in the 42.22% (24) in the premedicated group (p = 0.09). At 30 minutes it was 52.63% (19) in non-premedicated patients compared to 28.89% (13) in premedicated patients (p = 0.048) and at one hour it was 10.53% (4) in premedicated patients compared to 22.22% (10) in premedicates (p = 0.26) (Figure 2).
Anxiety or delirium occurred at any time in the postoperative period of 92.11% (35) in non-premedicated patients compared to 68.89% (31) in premedicated patients (p = 0.0194).
No statistically significant differences were found between patients with or without dexmedetomidine in adverse respiratory events: bronchospasm (0% vs. 2.63% (1); p = 1), desaturation (15.56% (7) vs. 18.42% (7); p = 0.958) or stridor (4.44% (2) vs. 10.53% (4); p = 0.521).
No cases of hypotension, bradycardia, post-operative bleeding, or need for reoperation have occurred.
Pre-operative anxiety in non-premedicated children is a serious issue that can occur in up to 65% and it is associated with negative behaviors such as nightmares, enuresis, night crying, and postoperative delirium [4]. In our study, we found a slightly lower frequency (57.89%) that decreased to less than half (26.67%; p = 0.008) with the use of intranasal dexmedetomidine (Figure 2).
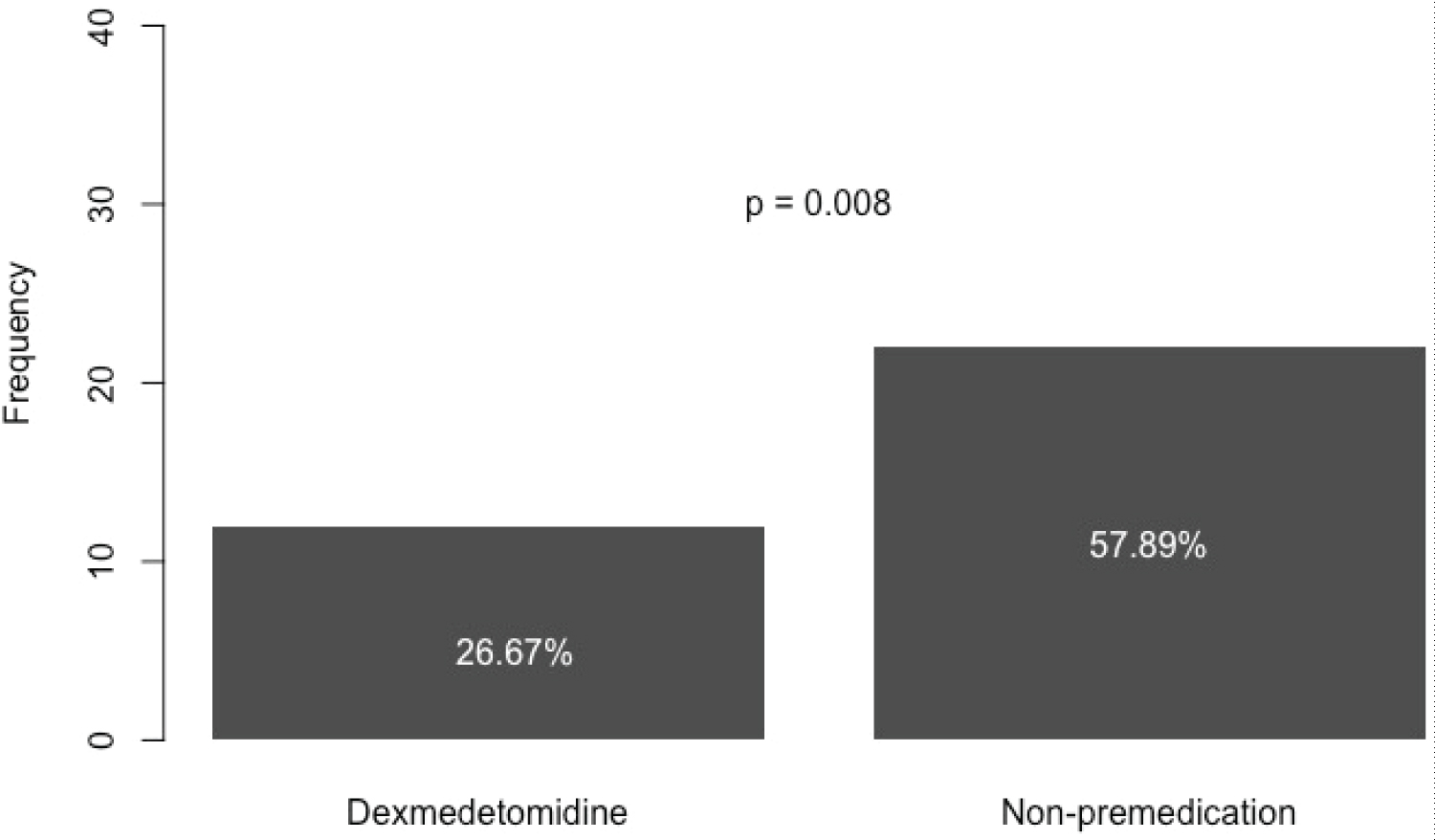 Figure 2: Preoperative anxiety. View Figure 2
Figure 2: Preoperative anxiety. View Figure 2
To measure preoperative anxiety, we used the YPAS scale. It can be used in the pediatric patient and has demonstrated good validity and reliability, both intra-observer and interobserver in numerous clinical trials [1,10].
The intranasal administration of dexmedetomidine was decided to achieve better bioavailability. In pediatric patients, oral transmucosal administration ends up being swallowed, thus losing bioavailability (16%) compared to intranasal of up to 84% [9,14,15].
Another of the primary objectives of the study was to compare postoperative delirium in premedicated versus non-premedicated patients as the risk of negative behavior is 3.5 times higher in children who experienced preoperative anxiety, being this an independent predictor [1,4].
Delirium is a dissociated state of consciousness during recovery from general anesthesia with no eye contact with caregivers, inconsolably, disorientation, and involuntary physical activity. It generally begins when the child wakes up from general anesthesia and can take up to 45 minutes to recover [7], so it was decided to measure it within the first hour after surgery. The pediatric anesthesia emergence delirium (PAED) scale of Sikich and Lerman [11], has been used as it is the only validated scale in the pediatric population [9]. A PAED value > 10 is considered delirium.
The incidence can be up to 80% depending on different risk factors such as age (older in preschool and school-age), type of anesthesia (use of sevoflurane for a faster awakening) or the type of surgery [2,8,16]. We observed in our study a high incidence (non-premedicated 68.42% vs. premedicated 53.33%) of postoperative delirium at any time postoperatively. We found no statistically significant differences between the study groups except at 30 minutes after the end of surgery when the incidence of delirium was lower in the group receiving dexmedetomidine. The incidence of postoperative delirium at 15 min and 30 min roughly coincides with the incidence of preoperative anxiety in non-premedicated, and the incidence of postoperative delirium found in premedicated at 30 minutes and one hour is also similar to the incidence of preoperative anxiety in this group, so the appearance of postoperative delirium in those with preoperative anxiety may be related. However, at 15 minutes the incidence of delirium in premedicated does not coincide with the incidence of preoperative anxiety. Pain does not seem to explain the increase in delirium in the first 15 minutes (OPS = 1). One of the possible explanations could be a residual effect of inhaled anesthetics in this period. Also, postoperative delirium at one hour decreases in non-premedicated, possibly related to the residual effect of midazolam that they needed to treat the higher incidence of this complication that they presented at 15 and 30 minutes (Figure 3).
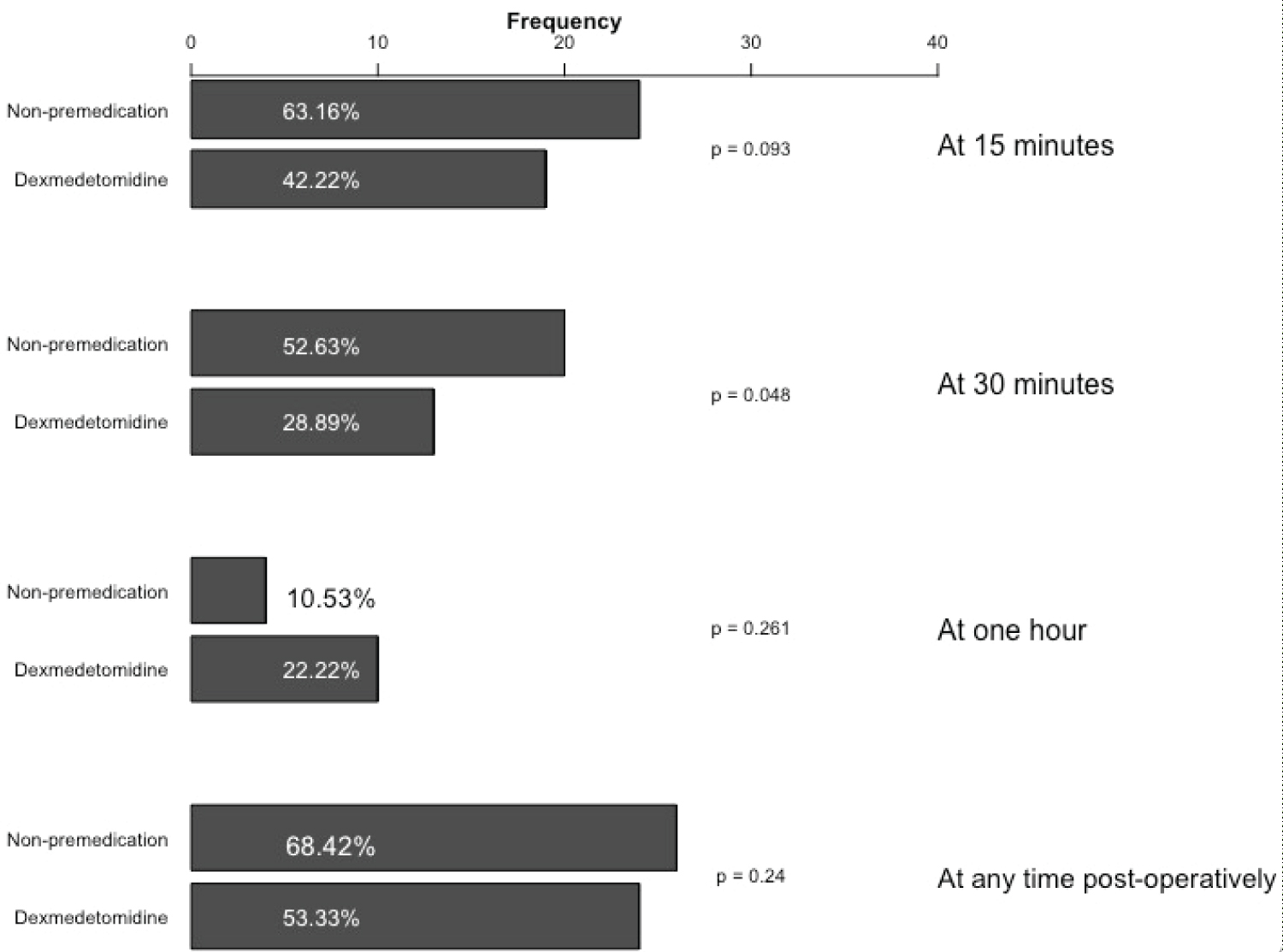 Figure 3: Postoperative delirium. View Figure 3
Figure 3: Postoperative delirium. View Figure 3
It is especially striking that 92.11% of non-premedicated children suffered from anxiety or delirium at any time in the perioperative period, decreasing to 68.89% with dexmedetomidine premedication with a statistically significant difference (p = 0.019) (Figure 4).
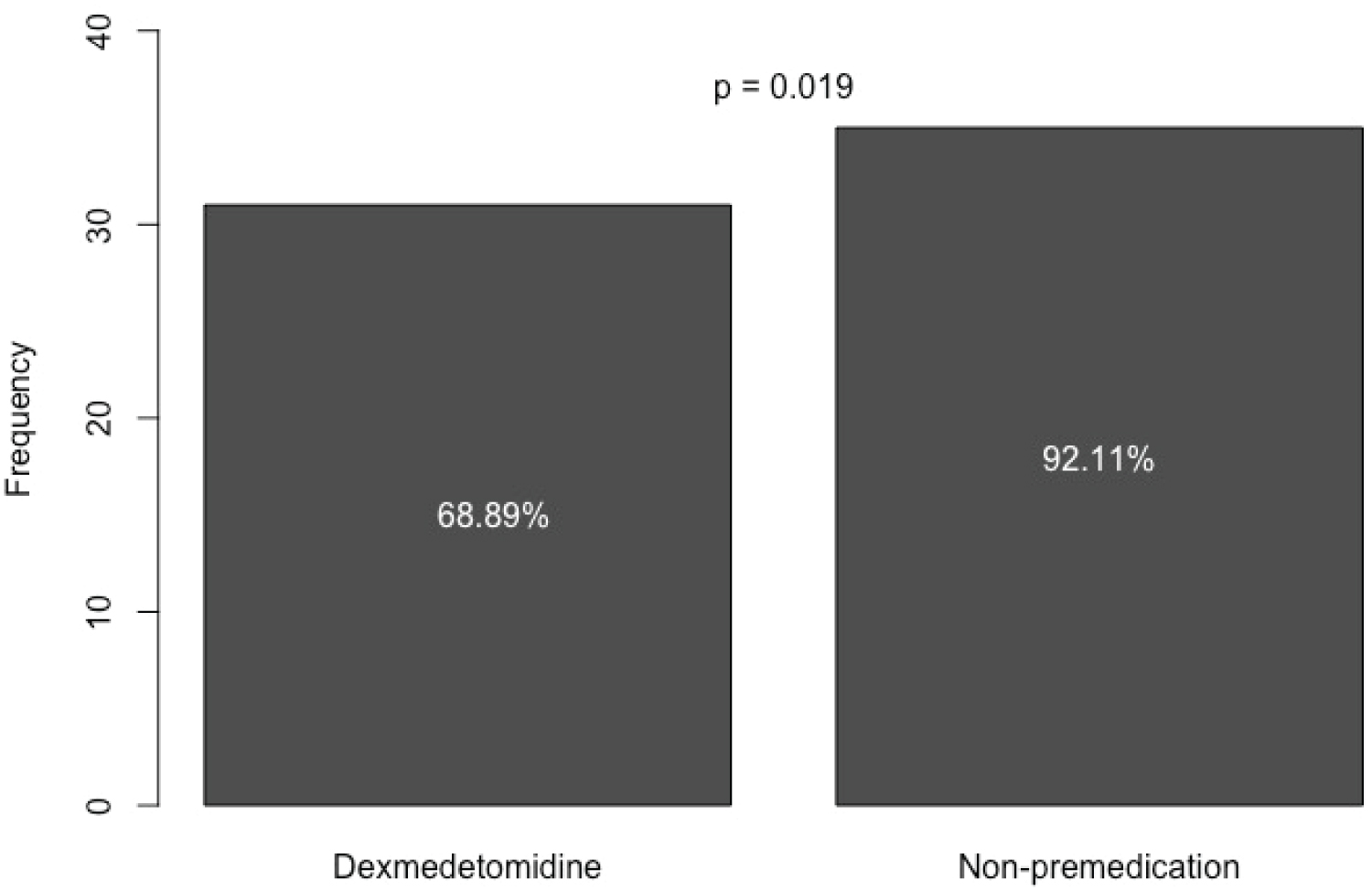 Figure 4: Anxiety or delirium at any time. View Figure 4
Figure 4: Anxiety or delirium at any time. View Figure 4
Several risk factors may have influenced these results. In this case, the comparable age range in both groups, the use of sevoflurane in 100% of the anesthetics collected, and the type of surgery (tonsillectomy) have been a risk factor for the appearance of delirium. In addition, these OSA patients should not receive premedication with benzodiazepines because they could increase postoperative apnea and PRAEs, so if they aren't premedicated, the risk factors are increased [1-3].
Inadequate pain control is another possible cause of postoperative delirium [1]. The fact that dexmedetomidine is a potent α2 adrenoreceptor agonist allows it to have analgesic effects, attenuating the stress response without respiratory depression [6,17]. Due to these effects, the meta-analysis of He, et al. concludes that the intraoperative use of dexmedetomidine is as effective as the use of opioids to prevent postoperative pain and delirium [6]. In our case, dexmedetomidine was administered only as a premedication and not intra-operatively, therefore the results did not reach this conclusion. In this study, intraoperative fentanyl requirements, postoperative pain or postoperative fentanyl did not show statistically significant differences.
Dexmedetomidine also has sedative effects [7]. Thanks to these effects, it reduces agitation and reduces the consumption of postoperative sedatives in PACU [6,18]. Regarding the midazolam needs of this study, in the postoperative period, they were higher in the non-premedicated group but without statistically significant differences.
Regarding PRAEs, it was hypothesized that less use of opioids or perioperative sedatives could decrease their appearance. There was a higher incidence of bronchospasm, desaturation, and stridor in children without premedication, but these differences were not statistically significant. Therefore, we cannot affirm that premedication with 1 µg/kg dexmedetomidine decreases PRAEs, possibly because this premedication alone failed to decrease the need for opioids and postoperative sedatives.
Although delirium resolves spontaneously, adverse effects such as self-injury or bleeding from the surgical site may occur during its course [19]. In this case, there has been no postoperative bleeding event or need for reoperation.
The most common adverse reactions from dexmedetomidine use are hypotension, hypertension, and bradycardia. These effects have occurred mainly with the use of intravenous dexmedetomidine, especially rapid bolus instead of perfusion [20,21]. In our case, there was no event of hypotension or bradycardia, possibly because the dose was low, and it was administered intranasally.
Although according to this study, with premedication with dexmedetomidine 1 µg/kg, anxiety or delirium has been decreased by 23.22% at any time of the perioperative period, it is necessary to think about how to decrease it even more. Since dexmedetomidine even at high doses of 3 µ/kg/h maintains airway tone even in children with OSA [9], it would be feasible to increase the premedication dose and/or add an intraoperative dose or infusion. Further studies are needed to know the safe dose in children and the timing of administration, which results in decreased postoperative delirium, pain, and sedation, and perioperative opioid requirements without producing side effects.
Nowadays, most studies of postoperative agitation in children have been performed with single or continuous intravenous doses of intraoperative or postoperative dexmedetomidine.
Also, the ability of dexmedetomidine to reduce preoperative anxiety has been studied, but although delirium has been described as a negative behavior of preoperative anxiety, there are no studies that relate the decrease in postoperative delirium with a decrease in preoperative anxiety thanks to a correct premedication. The data are limited in defining the dose in premedication or if it would be necessary to add an intraoperative dose of intravenous dexmedetomidine to reduce not only preoperative anxiety but also postoperative delirium and pain.
With this study we want to see if premedicated children have less preoperative anxiety and so then less postoperative delirium without intraoperative intravenous doses. It is hypothesized that intranasal dexmedetomidine premedication decreases the incidence of preoperative anxiety, postoperative delirium, postoperative pain and the need for postoperative sedatives and opioids.
This study has several limitations including non-randomization and the absence of double-blind.
Although it was indicated that premedication is performed 45 minutes before the start of surgery following the protocol approved by the hospital's pharmacy service, the lack of knowledge of the exact time of the start of surgery has led some patients to be transferred to the operating room before or after the effect.
The incidence of preoperative anxiety in preschool and school-age children who are going to undergo tonsillectomy surgery is very high and this can lead to postoperative delirium in a large number of patients.
Premedication with intranasal dexmedetomidine reduces preoperative anxiety and the incidence of anxiety and delirium at any time in the perioperative period.
At a dose of 1 µg/kg, no event of hypotension or bradycardia occurred. There was also no postoperative bleeding event or need for reoperation, nor was the occurrence of PRAEs decreased.
At these doses, there was no decrease in postoperative pain or less need for intraoperative or postoperative opioids or postoperative sedatives.
More studies are needed to establish effective and safe doses in pediatric patients of both preoperative and intraoperative dexmedetomidine.
Patricia Catalán Escudero: The conception and design of the study, patient recruitment, data collection, interpretation of data, and drafting the article.
Adolfo Ramos Luengo: Study design and data analysis and interpretation of data, revising it critically for important content.
Eva Delgado Encinas: Data collection and revising the article critically.
Ernesto Martínez García: Patient recruitment, revising it critically for important content.
The authors declare no competing interests.